
Abstract
Abstract
Virtual reality (VR) has been used by clinicians to manage pain in clinical populations. This study examines the use of VR as a form of distraction for dental patients using both subjective and objective measures to determine how a VR system affects patients' reported anxiety level, pain level, and physiological factors. As predicted, results of self-evaluation questionnaires showed that patients experienced less anxiety and pain after undergoing VR treatment. Physiological data reported similar trends in decreased anxiety. Overall, the favorable subjective and objective responses suggest that VR distraction systems can reduce discomfort and pain for patients with mild to moderate fear and anxiety.
Introduction
O
Pain perception has a strong psychological component. In order to experience pain, conscious attention is required. 2 Distraction has been found to take a patient's attention away from pain. Attention given to pain often determines not only the level of pain being reported, but also the distress levels. By encouraging a patient to focus his/her attention on other thoughts, less attention is available for the pain.4,5 Virtual reality (VR) utilizes advanced technologies to create virtual environments (VE) that allow patients to be immersed in an interactive, simulated world. 6 These advanced systems interact at many levels with the VE, stimulating sights, sounds, and motion to encourage immersion in the virtual world to enhance distraction from pain. 7
Other studies have also shown that involving the patient in a VE reduced their reported levels of pain during medical procedures such as chemotherapy, physical therapy, burn wound changes, and surgery (see Table 1).8–11 In one study where children either played video games or navigated through a VE while receiving wound care for their burns, exposure to VR lessened their reported pain ratings as compared with playing video games. 12 In another controlled study, adult burn patients undergoing physical therapy reported less pain while involved in VR than those that only participated in standard physical therapy. 13 Evidence shows that VR is effective in reducing pain in children with cancer, as chemotherapy-related symptom distress was reduced significantly immediately after using VR during treatment. 14 Specifically for dental work, another clinical study observed that dental patients undergoing plaque removal below their gum line experienced considerable reduction in pain when using VR compared to participants that watched a movie and to participants that did not have any type of distraction. 15
Research involving the concept of distraction has shown that techniques used in the past such as concentrating on deep breathing or watching a movie are less effective than using VR. This study examines the efficacy of using VR to control dental pain using both patient reported surveys and physiological measurements to evaluate fear and pain before and after dental treatment. Dental fear has been measured with questionnaires such as the Dental Anxiety Scale and Dental Fear Survey, as well as the Dental Fear Interview. While there are numerous self-report instruments that measure various aspects of the sensory, affective, and evaluative components of pain, only a few tools have been developed that directly assess fear and anxiety associated with pain. This study will integrate both subjective and objective variables to determine a more effective way of measuring and reducing both pain and distress.
Methods
Setting and patients
We recruited five adult patients for the study on a voluntary basis as they came for their dental treatments at the Scripps Center for Dental Care in La Jolla, CA (Dr. John F. Weston, D.D.S.) (see Fig. 1).

Patient in treatment room.
Outcome measures
Patients first completed the Dental Anxiety Scale and Amount of Fear Scale. The Dental Anxiety Scale is a 4-item questionnaire that asks about fear of dental treatment. The Amount of Fear Scale is a 45-item, Likert-type (1–5 scale) verbal report instrument used to assess dental fear. The survey provides a total dental fear score.
A post-experience questionnaire was created by the investigators to assess patient treatment preference and effects of the VR distraction system. This questionnaire includes the presence questionnaire (from Usoh et al. “Using Presence Questionnaires in Reality,” Witmer & Singer, Vs. 3.0), and STAIP-AD Test form Y (from Consulting Psychologists Press).
The Procomp+ biofeedback device by Thought Technology was used to assess physiological measures. This device is an advanced biofeedback and psychophysiological data acquisition system. It measures electromyogram (EMG), temperature, galvanic skin response (GSH), electroencephalogram (EEG), heart rate variability, heart rate, and respiration rate (see Fig. 2).
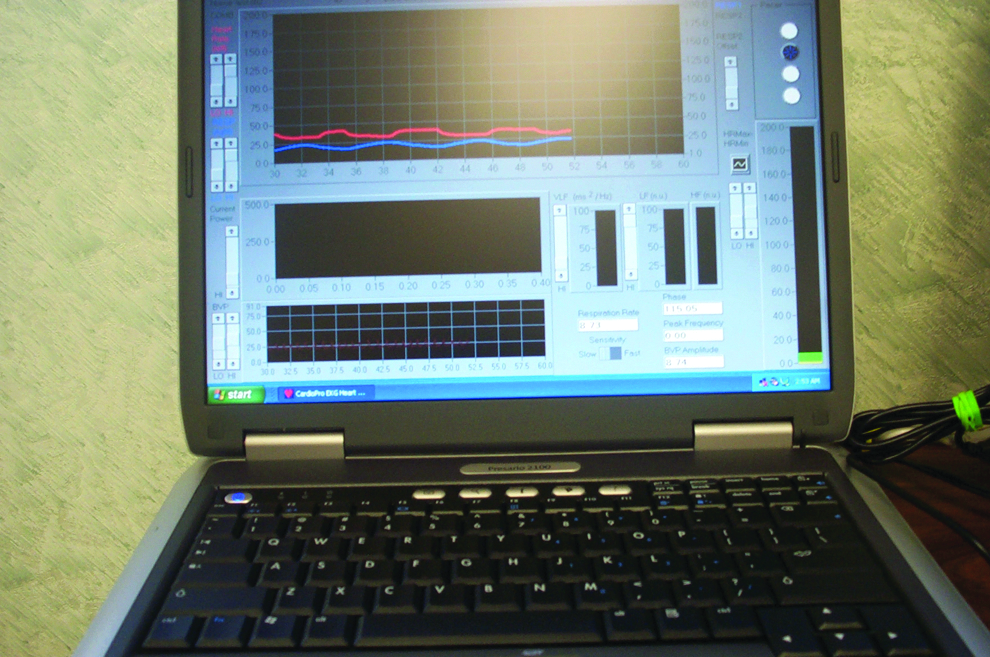
Psychophysiological monitoring and biofeedback equipment.
Procedures
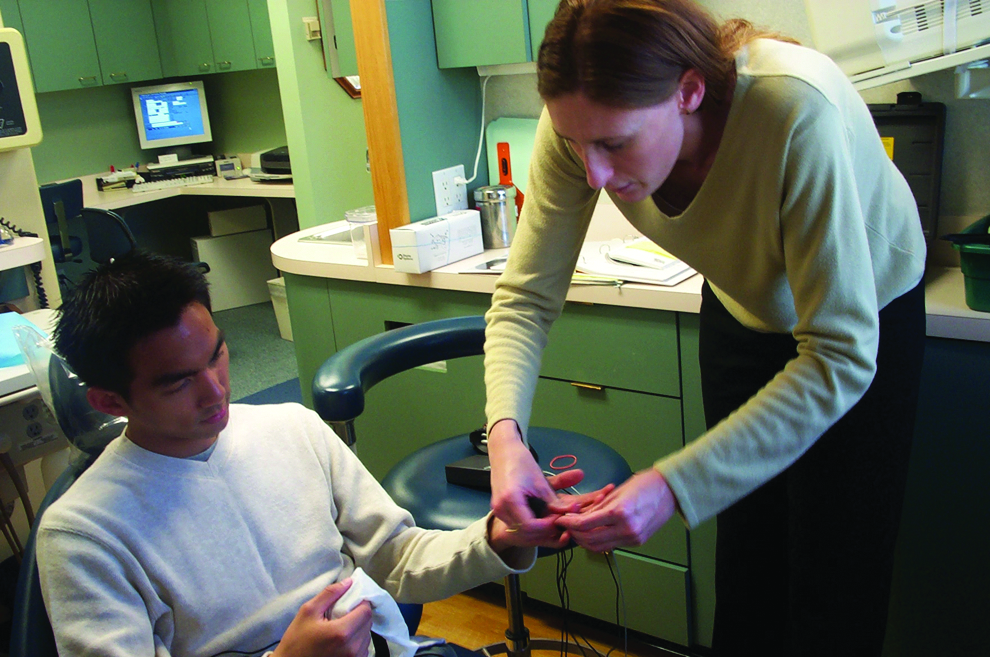
Before we began treatment, the patients completed the questionnaires. We also recorded demographic information, the date of last treatment, and the details about the dental procedure. We attached seven sensors to the patients' fingers, abdomens, and arms to gather physiological information. The clinician performed the dental treatment without the use of the VR distraction system for 5 minutes (see Figs. 3 and 4) and then performed it with use of the VR distraction system for 5 minutes (see Fig. 5).
Measurement without the virtual reality (VR) distraction system.

Biofeedback sensors and wireless trackball.

Measurement with VR distraction system.
The VEs included relaxing nature worlds where the patients could navigate through beaches, forest, mountains, and other pleasant areas. The patients self-navigated to provide a further sense of control.
Results
Standardized questionnaires
Scores for the pre/post questionnaires, including their sub-scales, are shown in Table 2.
0.4 for all patients; −1.5 for patients 1–4.
We evaluated the differences between pre/post self-evaluation scores (post−pre score=changes) with the t test (see Table 3).
For part I of the self-evaluation questionnaire (Ho:u=0, Ha:u<0), the p value is 0.56. This is strong evidence to support that the true mean of the change is >0, that is, treatment increased the scores for patients. Data from part II has a p value of 0.1875 (except patient 5 data; it is obvious that the value 8 is an outlier), supporting that using the VR distraction system decreased the anxiety for patients.
Physiology
We analyzed physiological measures (such as the heart rate and respiration rate) along with order and condition (after use of the VR distraction system and after nonuse of the system). In these analyses, several significant effects were shown (see Figs. 6 and 7; Tables 4–6).
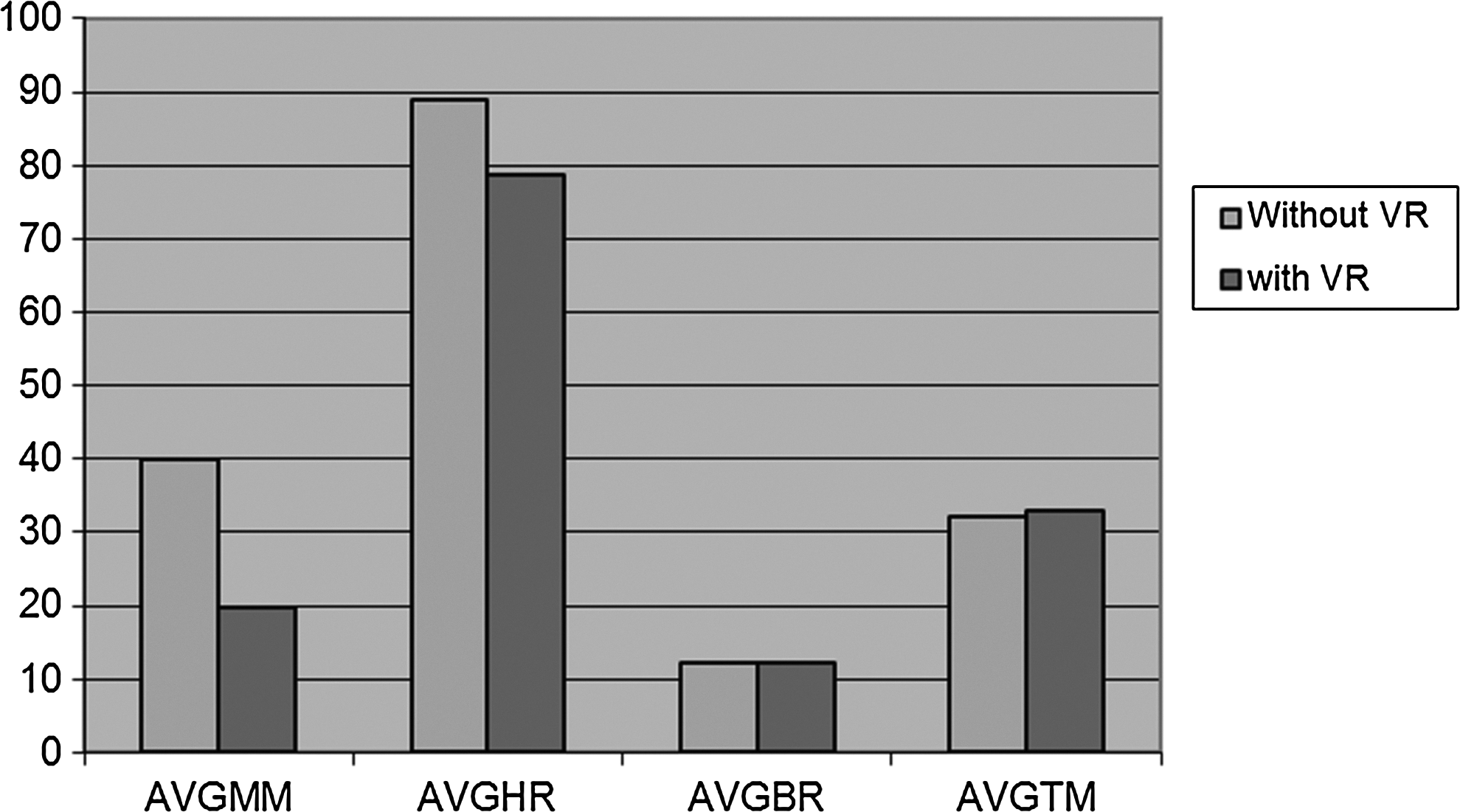
Results show a trend of factors related to fear and anxiety reduction with VR distraction.
Evaluation outcome chart (heart rate, respiration rate) example.
Within the EKG data, LFN increased an average of 14.968 for four of the five patients after VR distraction. The average increase of the LF frequency band most likely indicates effectiveness of the VR distraction in reducing anxiety.
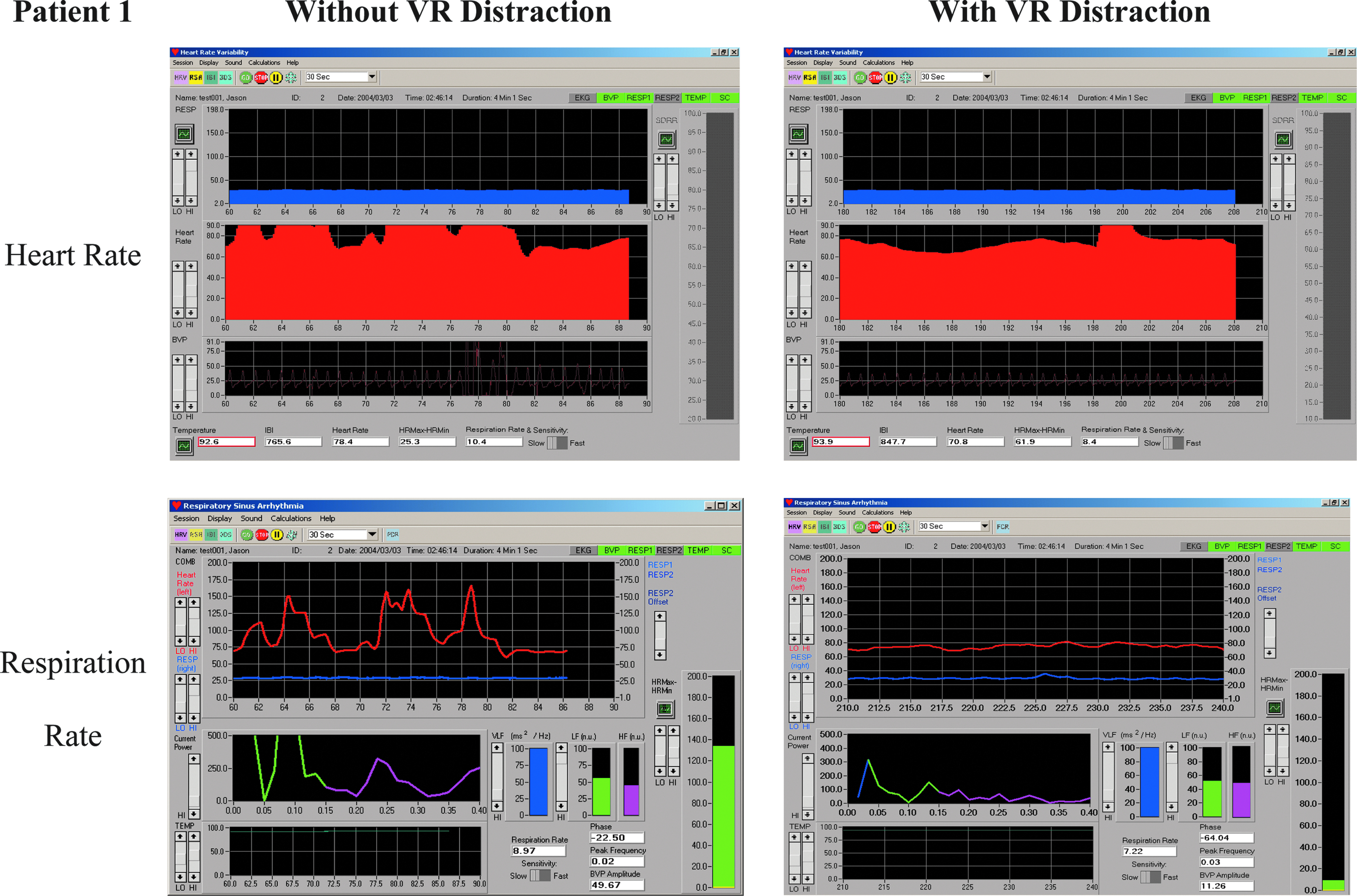
HRV is characterized by three main components: the high frequency (HF) component (0.15–0.40 Hz) measures the influence of the vagus nerve in modulating the sinoatrial node. The low frequency (LF) component (0.04–0.15 Hz) provides an index of sympathetic effects on the heart, particularly when measured in normalized units. The very low frequency (VLF) component (0.003–0.04 HZ) reflects the influence of several factors on the heart, including chemoreceptors, thermoreceptors, the renin-angiotensin system, and other nonregular factors. Almost all of the variability from a short-term spectral analysis of HRV is captured in these three components. An example of one of the patient's EKG data is shown in Figure 8 to visualize the comparative features.
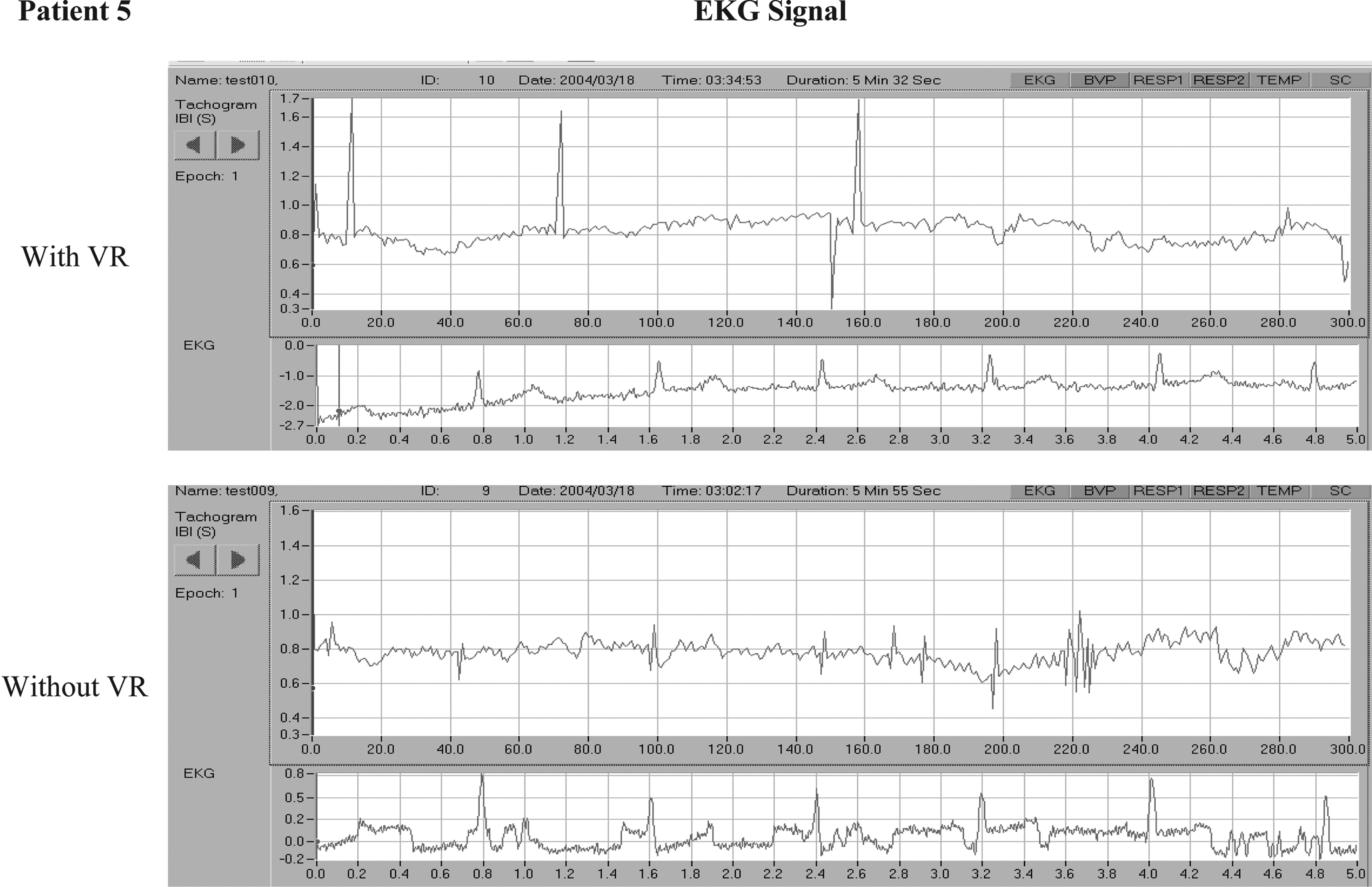
EKG of patient 5 with and without VR distraction.
Discussion
An inexpensive, commercially available VE could have a significant impact in reducing perceived pain involved in a variety of medical procedures.
The physiological results of this research suggest that the use of the VR distraction system may be a beneficial option for patients with mild to moderate fear and anxiety associated with dental treatments. This system may be a useful adjunct in dental offices to help reduce anxiety, discomfort, boredom, and the time required to perform routine dental procedures. It allows them to relax by allowing them to navigate to another location while still physically remaining in the dental office.
Additional research exploring the mechanism by which VR distraction is achieved will be needed. There is much room for improving “presence and realism” in future VR applications specifically designed for treating pain. New virtual worlds, custom built to be more immersive, could produce even larger reductions in pain. Such new worlds can take advantage of the versatility of VR software. On a clinical level, several observations were noted by the clinical staff and from the survey results to improve on existing problems with the design of the study (see Table 7).
The cost of an immersive VR system has dropped dramatically since the mid-1990s, and additional price reductions are inevitable. At the same time, the quality and portability of VR has increased dramatically, benefiting from the enormous improvements in more conventional computer technology (e.g., cheaper memory, cheap and fast graphics accelerators, higher information processing capabilities of the hardware, and a dramatic maturation in the quality of VR world building software commercially available).
To summarize, the present study provides encouraging initial support for the use of VR as a technique for controlling fear and anxiety during dental procedures. Additional empirical research will be needed to determine whether VR can become a viable form of fear and anxiety control during dental treatments. Techniques that prove effective for treating dental pain will likely prove effective for other painful procedures.
Footnotes
Acknowledgments
We thank the National Institute on Drug Abuse, National Institutes of Health for partial funding of this project. We also thank the participants who were willing to spend time with our clinical team.
Author Disclosure Statement
No competing financial interests exist.