
Abstract
Abstract
We explored the use of virtual reality distraction techniques for use as adjunctive therapy to treat chronic pain. Virtual environments were specifically created to provide pleasant and engaging experiences where patients navigated on their own through rich and varied simulated worlds. Real-time physiological monitoring was used as a guide to determine the effectiveness and sustainability of this intervention. Human factors studies showed that virtual navigation is a safe and effective method for use with chronic pain patients. Chronic pain patients demonstrated significant relief in subjective ratings of pain that corresponded to objective measurements in peripheral, noninvasive physiological measures.
Introduction
P
VR has also been found to be effective in reducing reported pain and distress in patients undergoing burn wound care, chemotherapy, dental procedures, venipuncture, and prolonged hospital visits.2–16 It appears that VR may change how the brain physically registers pain, not just the perception of pain stimuli. 2 An interesting study showed that 86% of patients undergoing wound care from a burn injury reported severe to excruciating pain even with therapeutic levels of opioids. 3 The challenges of treating severe pain confront clinicians daily. The search for adjunctive techniques has led to a number of studies where pharmacological agents are combined with behavioral modification approaches. More recently, distraction techniques have been used as an adjunct during unpleasant medical procedures. Examples of these techniques include deep breathing, viewing videotapes, listening to music, and playing video games.4–6 The success of these psychologically based techniques has led to the innovative use of VR as a distraction technique (see Table 1).
A study conducted by Sarig et al. explored the use of VR in managing chronic neck disability and pain. Twenty-five symptomatic and 42 asymptomatic individuals reported pain using conventional pain ratings as their cervical range of motion was measured. The goal of the study was to determine if range of motion correlates with pain management. Results indicated significant limitations in range of motion measurements, as they showed sensitivity but lacked specificity. 22 In 2013, Sarig et al. conducted a similar study to explore the issue further. Out of 25 patients, a comparison of self-reported outcomes and cervical range of motion showed correlations of 0.4–0.6 between the two measurements. This objective quotient indicates that subjective pain ratings can be supplemented with range of motion measurements and fear of motion reports to measure pain for physical rehabilitation studies. Moreover, VR was seen to not only reduce pain but objectively increase function. 16
A pilot study of VR to treat fibromyalgia in 2013 studied the long-term effects of VR therapy. The six women in the study who had undergone 10 sessions of therapy supported by adaptive virtual environments (VEs) were assessed at pretreatment, post-treatment, and at 6 months follow-up. Results show that both depression rates were significantly reduced and coping strategies reflected positive growth. 19 Another fibromyalgia study considered the use of noninvasive mirror visual feedback using VR to treat chronic pain of one fibromyalgia patient using ketamine as a pain reliever. On a 15 trial experiment, patient pain was shown to have decreased significantly, indicating the supplementary nature of VR with other medications. 20
In 2010, Patterson et al. combined VR with hypnosis. The randomized, controlled study of 21 trauma patients compared subjective pain ratings of patients that were induced under VRH (virtual reality hypnosis) and standard VR. Positive results of VRH therapy indicate a synergistic and additive effect of the analgesic efficacy of hypnosis and VR distraction techniques. 23
Other chronic conditions have been studied using VR as an adjunctive treatment. The first dermatological study of pruritus was conducted in 2009. Exposure to a computer-simulated game seemed to reduce the subjective pruritus intensity significantly among the 24 patients. Although pain and itching are activated under different internal brain mechanisms, a comparison of the commonalities of pain receptors, activations, and neural pathways can lead to insights on how to use these tools for the treatment of a variety of conditions such as chronic itching and chronic pain. 24
Methods
Participating in this study to investigate the efficacy of an interactive VE were 40 patients aged 22–68 years with average daily pain for at least 3 months and a daily average pain intensity score of ≥4 (0=no pain, 10=worst possible pain).
Results
Before we tested the pain distraction system on patients, we wanted to validate usability and safety in controls. To determine the human factors related to the use of our pain distraction system, we conducted an initial study with 15 controls. The subjects were enrolled as per the approved IRB protocol and signed the consent form. All participants went through a 15 minute VR exposure session while wearing a HMD. The VEs consisted of pleasant and relaxing scenes, including natural areas such as forests, beaches, and mountains. Relaxing music and soothing effects such as the branches swaying and tall grass moving were added. Tree branches for example moved six to eight times per minute to guide breathing regulation.
Self-report questionnaires were completed by participants and scored on a scale of 1 to 7, where 1=“no effect” and 7=“highly effective.” Overall the pain distraction VE was found easy to use, had good stereo sound effects, and was immersive and interactive (see Figs. 1–3).
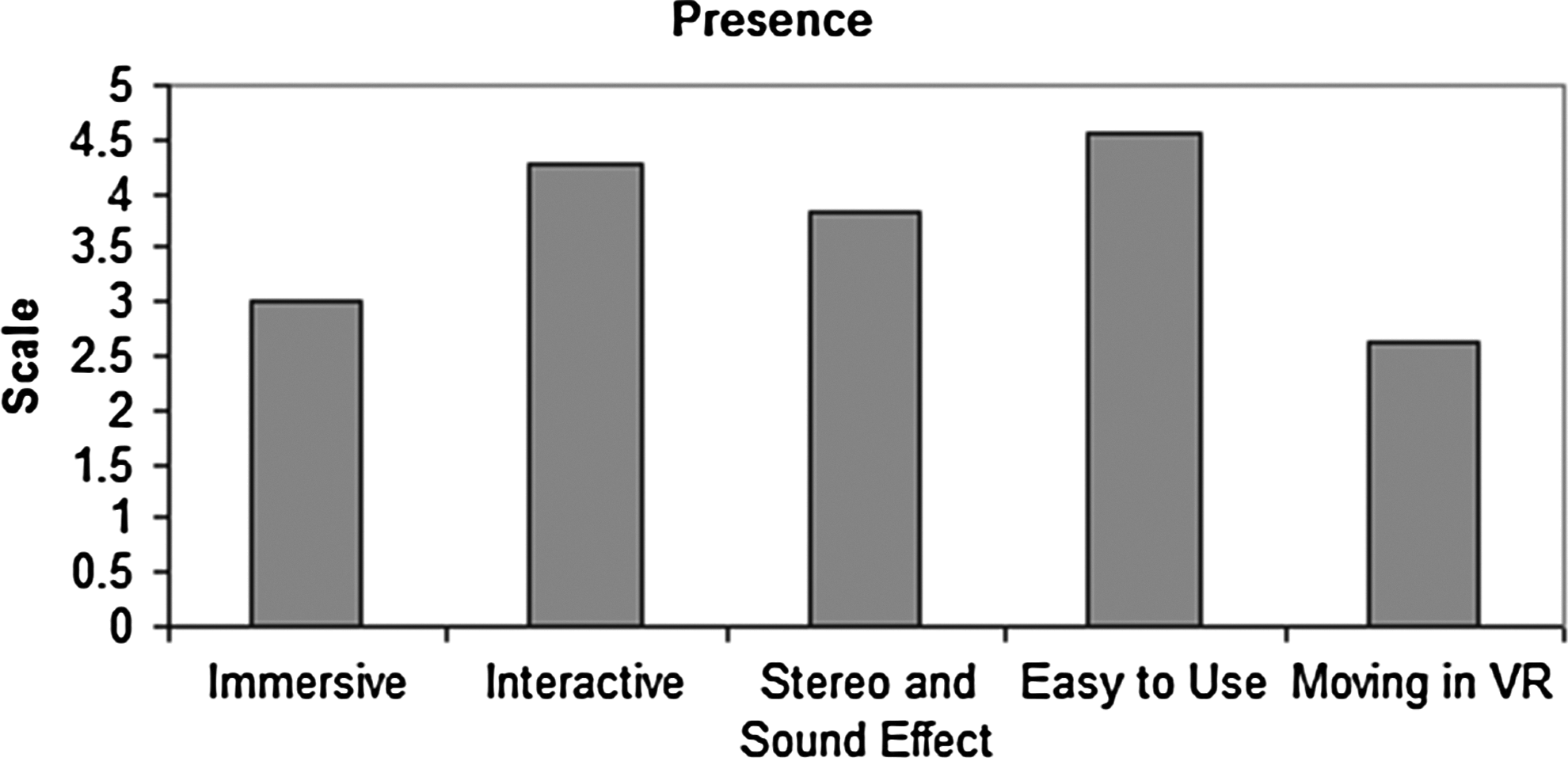
The scales of sense of being in the virtual reality (VR) simulated environment—Ease of use, Immersive, and Interactive effects on a scale from 1 to 7, where 7 represents the normal experience of being in a place. 1=“not at all,” 7=“very much.” VR environment was easy to use, interactive, immersive, and real.
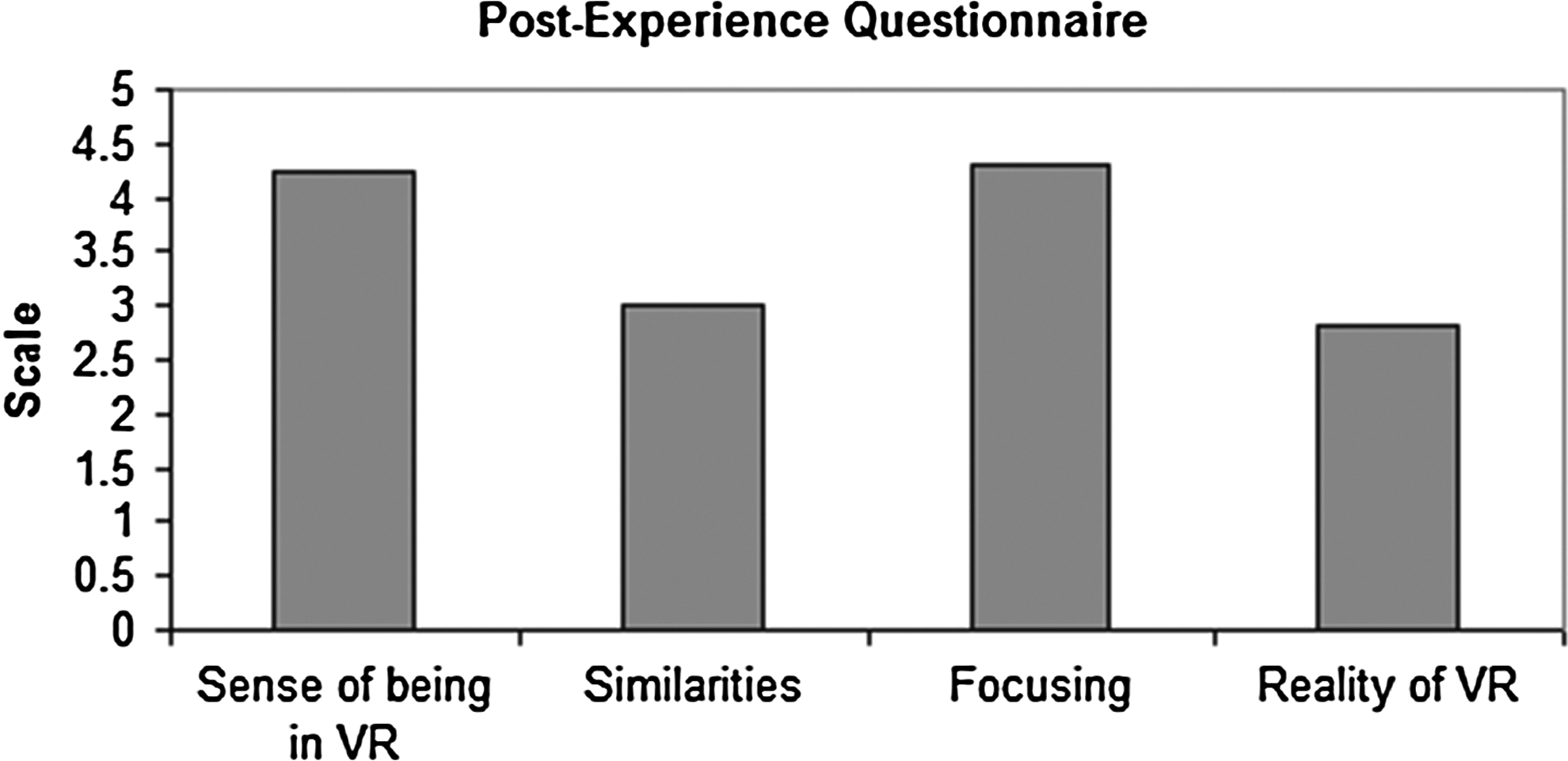
The scales of sense of being in the VR—how real was VR versus the simulated environment, similarities between the simulated environment and the actual places patients visited, how focused on the tasks patients were during the simulated environment, on a scale from 1 to 7, where 7 represents the normal experience of being in a place. 1=“not at all,” 7=“very much.” VR was immersive and real.

Sickness exploration questionnaire scores in terms of general discomfort, fatigue, headache, eyestrain, and nausea, their mean scales are all <1.5, where the scales range from 0 to 3. 0=“Absent,” 3=“Severe.” No serious side effects were observed. It was determined that VR was indeed safe to use with this population.
Controls reported good levels of presence and immersion when using the environments. The system was easy to use and understand. Evaluation of post-experience questionnaires showed that the sense of being in the VEs was high. This sense of being in VR correlated well with levels of immersion and interactivity on the presence questionnaires. Because we were concerned with potential adverse effects in patients using the VR system, we administered the Simulator Sickness Questionnaire. This questionnaire showed very low levels of fatigue, headache, eyestrain, and nausea when using the VR system. These low numbers indicate the VR system is both safe and effective.
In our first pilot study, six chronic pain patients, ranging in age from 22 to 68 years, tested the VE with a head-mounted display and physiological sensors. All six participants reported a drop in pain while in the VE, and the magnitude of pain reduction from the VR compared to the pain focus condition was large (75.8%) and significant. A nonparametric Wilcoxon signed rank test indicated that the mean pain rating during the VR condition was significantly lower than the session with no distraction (n=6; p=0.028). Each of the six participants exhibited higher mean skin temperature when engaged in the VE than when in the pain focus condition. A paired t test also indicated that the overall mean temperature was significantly higher when participants were using VR (df=5; p=0.004). A higher average temperature in VR suggests a reduced level of discomfort and anxiety, substantiates the self-reported pain ratings, and suggests that VR is an effective method of reducing pain and anxiety (see Figs. 4 and 5).

Comparison of subjective pain ratings.
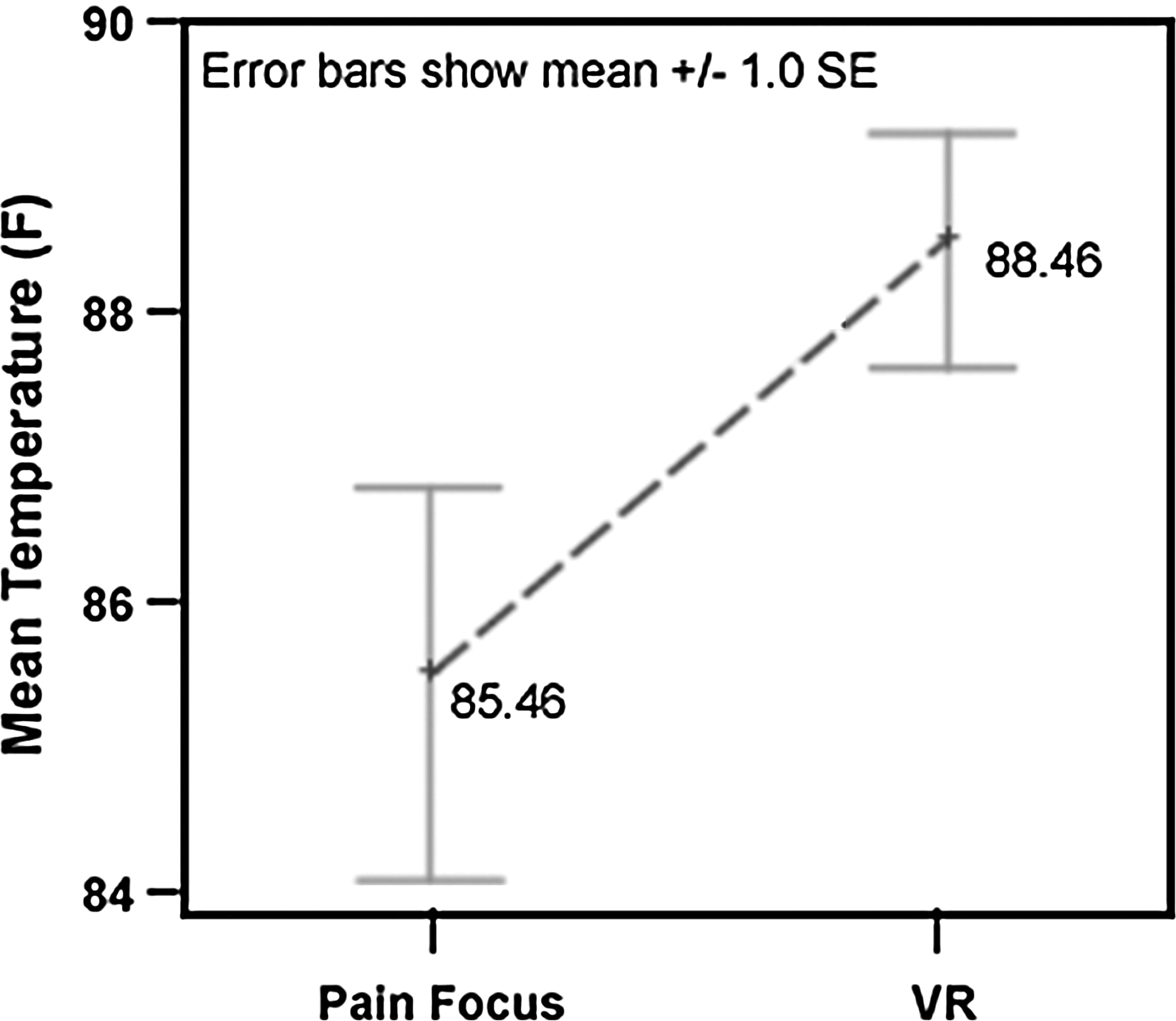
Comparison of objective pain ratings.
As in the previous study, we compared a pain focus condition to a VE exploration condition in 34 additional chronic pain patients. Data on heart rate and skin temperature were collected, as well as pain intensity ratings obtained from self-report questionnaires. All patients reported a decrease in pain while in the VE, with significance ranging from p<0.05 to p<0.001, depending upon which of the three pain rating scales were used (see Fig. 6). The significant decrease in heart rate (p<0.05) while the patients were in the VE indicates a reduced level of pain and anxiety, and suggests that VR is an effective method of reducing this distress (see Fig. 7).

Comparison of reported pain intensity.

Comparison of heart rate.
Discussion
Overall, the results of this study show VR is effective at reducing pain. Within the subjective outcomes, patients reported significantly lower pain ratings while exploring the VE than during the pain focus session. Several patients reported encouraging feedback as well, such as “this is the first pain relief I have had in 3 years,” “I was so busy playing the game, I forgot about my pain,” and “even though the procedure was finished, I wanted to keep playing.” This shows that this technology is significant not only in reducing pain but also in eliminating the interruptive nature of chronic pain.
Moreover, objective measures further supported the reduction of pain with use of the VR system. Skin temperature was significantly higher and heart rate was lower during the VR session, which indicates greater relaxation.
In virtual technologies, a necessary factor to consider is the presence felt by the user. In a study conducted by Hoffman et al., the distractive properties of a virtual program were greatly enhanced with higher immersion and presence of the VE used to reduce pain and anxiety of burn patients. 26 Similarly, a comprehensive review of immersiveness on physiology reported that greater immersion has relaxing effects on physiological factors such as heart rate, respiration rate, skin temperature, and skin resistance. 27 Due to the high presence and realism scores of the self-report surveys, the virtual program used in this study can be considered as effective in engaging patients, and thus distracting from pain.
Additional studies can further determine the correlation between presence and pain management, as well as the association of pain distracting qualities of VR and various types of pain.
Footnotes
Acknowledgments
We thank the National Institute on Drug Abuse, National Institutes of Health for partial funding of this project. We also thank the participants who were willing to spend time with our clinical team.
Author Disclosure Statement
No competing financial interests exist.