
Abstract
Abstract
Immersive virtual reality is thought to be advantageous by leading to higher levels of presence. However, and despite users getting actively involved in immersive three-dimensional virtual environments that incorporate sound and motion, there are individual factors, such as age, video game knowledge, and the predisposition to immersion, that may be associated with the quality of virtual reality experience. Moreover, one particular concern for users engaged in immersive virtual reality environments (VRE
Introduction
A
The rule is clear: The closer the system is to human perception, that is, the matching between multimodal information channels (e.g., visual, auditory, or tactile) to the user's head and body, the higher the immersive potential.10,11 However, immersion may not be only mediated by technological issues but by negative side effects and individual factors as well. 12 Immersive tendency, an individual's tendency to become immersed in VREs, is believed to be intimately associated with cybersickness. 13 This type of motion sickness is characterized by symptoms, such as sweating, drowsiness, disorientation, nausea, and vomiting, compromising the sense of presence and the whole VR experience. 14
Based on previous literature, an individual with a greater predisposition to become more immersed in VRE will tend to experience lesser cybersickness symptoms and vice versa.12,13 Moreover, and despite several studies have shown that immersion tendencies are positively correlated with presence, that is, an illusion state of “being there,”15–17 no studies have focused on the relationship between individual factors and user's immersive trait-like tendency. If there are endogenous factors, such as demographic characteristics, perceptual, cognitive, and motor abilities, or even personality that may impact on presence,18–21 it seems logical that the combination of individual characteristics may be also associated with a certain level of immersive tendency and, thus, may impact on cybersickness and subsequently the quality of the VR experience. 22
Since cybersickness impacts the dropout, it would be helpful to clarify the relationship between the trait-like tendency to immersion, cybersickness, and which individual characteristics that are linked to both. To date and to the best of our knowledge, no studies on immersion tendencies have presented a multidimensional approach that allows the analysis of relationships between the individual variables that might be associated with the user's immersive tendency and cybersickness and between different levels of those variables.
A multiple correspondence analysis (MCA) combined with a cluster analysis (CA) technique was performed to profile the best-suited user for VRE, that is, the user profile associated with lower levels of cybersickness, that is, an indicator of better quality experience in VRE. An evident advantage of this combined statistical technique over other multivariate approaches yielding joint graphical displays, is that it facilitates the analysis and detection of the relationships between variables. 23 This technique enabled us, in contrast to previous studies, to better understand the association patterns across a large set of individual determinants of cybersickness in a multidimensional space, allowing the creation of typologies of VRE users.
Methods
Participants
Seventy-one undergraduate and master's students from the Lusophone University of Humanities and Technologies in Lisbon were enrolled in this study. Regarding gender, 33.8% were males (n = 24) and 66.2% were females (n = 47), with mean ages of 24.69 years (SD = 7.67) and 23.10 years (SD = 7.01), respectively.
Measures
In terms of sociodemographic factors, only age was considered in our analysis. The exclusion of gender from analysis is based on current evidences that game experience explains better the variability in immersion and cybersickness. 24 We also considered the gaming lifestyle of the user, which was assessed through eight items. Four items related to “computer experience,” “experience with IMAX,” “experience with VR,” and “gaming frequency” were taken from the ITC-Sense of Presence Inventory (ITC-SOPI). 25
The items “experience with IMAX” and “experience with VR” were measured through a dichotomous response (yes/no), whereas the item “computer experience” was evaluated through a 4-point Likert scale (1 = none to 4 = expert), and the item “gaming frequency” was measured by a 5-point Likert scale (1 = never to 5 = every day).
Four more items related to game experience were adapted from the Survey of Spatial Representation and Activities (SSRA), 26 such as “favorite platform for playing,” “number of video games bought per year,” “how does the user play,” and “game controller used for playing,” and were added to better profile video gamers. Regarding the item “favorite platform for playing,” it was measured through a dichotomous response (PC/console), as well as the item “how does the user play” (alone/accompanied) and the item “favorite platform for playing” (keyboard or mouse/joystick or game pad). The item “number of video games bought per year” was measured as an interval variable.
The predisposition to immersion was assessed through the Immersive Tendency Questionnaire (ITQ). 15 ITQ is composed of three subscales (Involvement, Focus, and Games) with 18 items to assess the capability to experience presence in an immersive virtual environment. The ITQ uses a seven-point scale format based on the semantic differential principle. 27 The internal consistency measure of reliability of ITQ was fair (Cronbach's α = 0.75). 15 In our study, similar internal consistency was found (Cronbach's α = 0.77).
The Simulator Sickness Questionnaire (SSQ) 28 was used to assess cybersickness. The SSQ has a 4-point scale to rate 16 symptoms of simulator sickness, such as nausea, eye fatigue, and vertigo. The SSQ produces a total score and three subscale scores: Nausea, Ocular–Motor Problems, and Disorientation. In terms of internal consistency, the SSQ presented fair reliability (Cronbach's α = 0.71). 29 A good internal consistency was found for SSQ in the present study (Cronbach's α = 0.83).
Procedure and apparatus
Upon arriving to the experimental laboratory, the participants were explained the general purpose of the study. The whole procedure was described, and participants were asked to complete the informed consent form, being informed that they leave the experiment at any time they wanted to. A protocol consisting of a sociodemographic and gaming lifestyle questions and the ITQ were filled out before the experimental task.
The VRE, in the first-person perspective, was developed in Hammer (Valve™) and composed of a hazardous and puzzle-solving path to an airport. This VRE was part of a larger set of VREs developed by the Laboratory of Computational Psychology at the Lusophone University and was usually used as neutral or training VRE. All participants were instructed to find their way to the airport, resourcing objects placed in the VRE that would lead to an engaging nonlinear route to the airport. The most complex task of the scenario was presented to the participants in a room where they had to use some cement bricks to keep a swinging platform in the upright position, so that they could jump into the airport access, leading to the airport's street, where the objective was considered completed (Fig. 1).
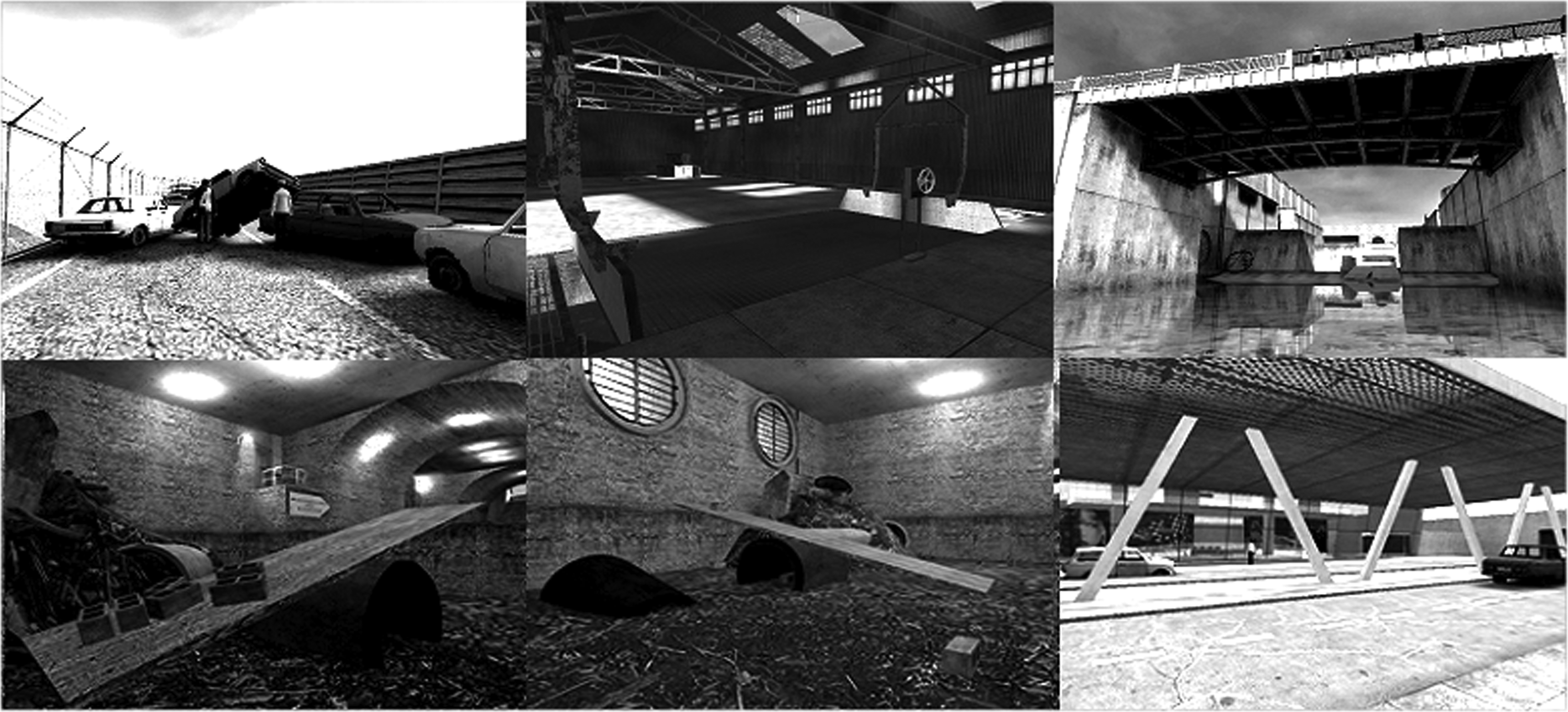
From top left to bottom right (clockwise) the several tasks needed to be completed to achieve the final goal: finding the airport (bottom right image).
The computer used was a high-performance custom-built desktop coupled with an optic mouse and a keyboard. To enhance higher levels of immersion, the VRE was displayed through an HMD (eMagin Z800 with tracking system) with an 800 × 600 resolution. Participants with ophthalmologic conditions wore their prescribed glasses for the experiment. Sounds were played through desktop speakers in front of the participant. The researcher left the experimental room when the experiment started. The experimental task was monitored from a researcher/control room through a window and a TFT monitor on which the VRE was also displayed. After task completion, SSQ was administered. After that, participants were thanked and dismissed. The whole experiment, involving the completion of questionnaires and the VRE, was carried out in an isolated, soundproof, and dimly lighted room and took, on average, around 40 minutes for each participant.
Data Preparation
All data were inserted and coded in Excel 2010 and then finally imported and analyzed in IBM-SPSS 20 (Statistical Package for the Social Sciences) for Windows.
Gaming lifestyle indicators
In MCA approach, it is essential to identify multiple indicators considered relevant to capture the structure of the phenomenon under study. Table 1 presents gaming lifestyle indicators, its respective categories, frequencies, percentages, and nonresponses.
NR, nonresponse.
Regarding representativeness of variables' categories, all presented similar proportions, except for the item “experience with IMAX.” The item “the favorite platform for playing” presented the highest percentage of nonresponses (36.6%, n = 26), whereas the items “computer experience,” “frequency of gaming,” and “how do you play” presented no nonresponses.
Supplementary variables
Age, immersion tendency, and cybersickness level were treated as supplementary variables, that is, zero-weight variables without interfering with the estimation of the principal factors (principal axes). 30 Concerning age, participants showed a mean age of 23.54 years (SD = 7.01). Age was discretized into three age groups (adolescents, young adults, and adults) as suggested in the literature. 31
In relation to immersion tendencies, participants showed a mean of 69.54 (SD = 12.55), and for cybersickness, they showed a mean of 379.57 (SD = 347.90). Discretization was performed based on quartile values: immersion tendencies (low/low to moderate/high to moderate/high) and cybersickness (low/low to moderate/high to moderate/high). Table 2 presents the supplementary variables (age and quality of VRE experience), its respective categories, frequencies, percentages, and nonresponses.
NR, nonresponse.
No nonresponses were encountered for the supplementary variables, except for cybersickness (n = 6; 8.5%). These nonresponses were linked to the occurrence of missing or invalid responses to at least to one SSQ item and were discarded from the analysis.
Results
The relationships between variables were examined through MCA.a This method is a multivariate approach used to explore the relationship between categorical variables. 32 The first step in MCA was to set the maximum number of dimensions through the following expression:
Rmax = min {(n – 1); (p – max (m1;1))},
where:
n: number of individuals
p: number of categories (active)
m1: number of variables (active) with nonresponses.
From the initial 14 dimensions (maximum number), only 2 were retained. The first dimension explained 33.7% of variance, and the second dimension explained 26.2%, as is depicted in Figure 2.

Representativeness of the initial dimensions based on inertia values.
The MCA was performed once again but only with two predefined dimensions.
Furthermore, the variables “experience with IMAX” and “experience with VR” revealed inappropriate discrimination values and were removed from the analysis. Table 3 describes the discrimination values for the gaming lifestyle indicators.
The first dimension was thought as gaming practices that differentiate gaming frequency, favorite gaming platform, type of interface, and how participants play. The second dimension was thought as computer/game knowledge. This dimension is associated with computer experience and with the purchase of games per year. Subsequently, a topological schema for the gaming lifestyle was performed. The results pointed out three clearly different types of gaming lifestyle (Fig. 3).

Multidimensional space between scores for gaming lifestyle indicators and supplementary variables.
To confirm these topologies, object scores were saved, and a hierarchical clustering was performed. According to Reis, 33 when the division of a new group presents no significant changes in the fusion coefficient, it should be assumed that the partition is adequate. Under this view, three clusters were identified. In a second stage, a K-means clustering was conducted presenting the following partition (Table 4).
With the purpose of validating this classification, three clusters were projected in the multidimensional plan (Fig. 4).
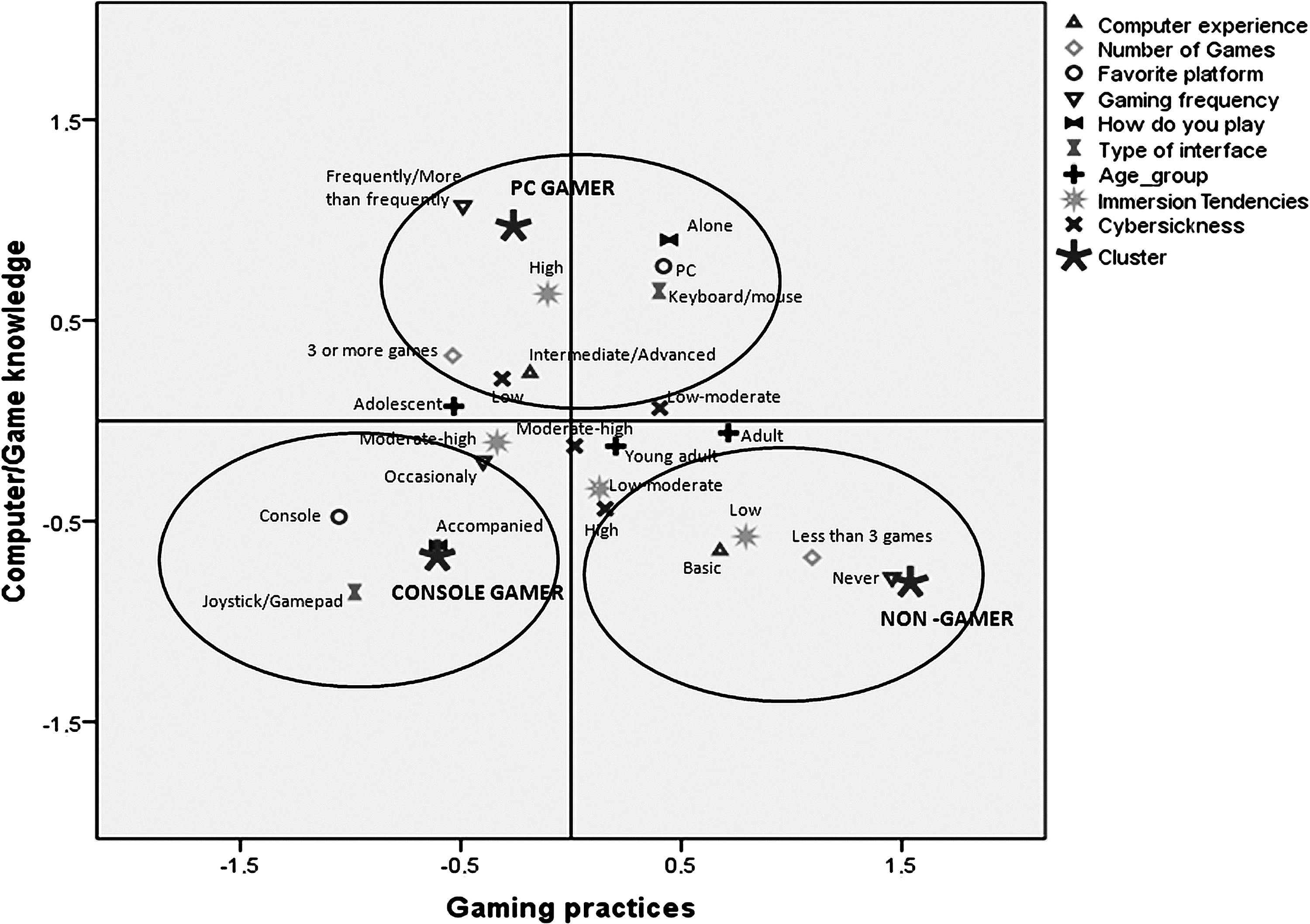
Multidimensional space between gamer profiles (clusters), scores for gaming lifestyle indicators, and supplementary variables.
The figure leads to the conclusion that clusters are consistent with the mentioned profiles. Console gamers are represented in cluster 1, whereas PC gamers correspond to cluster 2, and nongamers match cluster 3. The PC gamer profile is linked to “intermediate/advanced experience in computers,” the use of “PC as favorite gaming platform,” as well as “plays frequently alone,” “the keyboard or mouse is the interface used to play,” and “purchasing three or more games per year.” The console gamers' profile joins the “use of console” to the use of the “joystick or game pad to play.” These gamers play “occasionally” with “someone else.” The nongamers' profile is associated to “basic experience in computers,” “nonplaying,” and the “purchase of less than three games per year.”
Moreover, the projection of the supplementary variables showed that the adolescents are closer to the PC gamer profile. In turn, adults are closer to the nongamer profile. As expected, higher immersion tendencies and lower levels of cybersickness were linked to PC gamers' and console gamers' profiles, whereas low immersion tendencies and lower levels of cybersickness were linked to nongamers' profile.
Discussion
The present analysis sought to classify the users according to age, gaming lifestyles, predisposition to immersion, and cybersickness. The results indicated the existence of three different typologies when it comes to VR experience (level of cybersickness).
The PC gamers' profile showed that these participants play frequently alone with a keyboard/mouse. This profile is more associated with young ages (adolescence), being also associated with a higher predisposition to immersion and lower levels of cybersickness. In contrast, console gamers are teenagers and young adults, who play console occasionally with joystick/game pad and are more associated with a moderate degree to become immersed. The nongamers are usually adults who have basic computer experience and showed higher levels of cybersickness, subsequently displaying a lower quality VRE experience.
The present results corroborate previous evidence34–36 and suggest that VRE might work better with users with PC gaming experience, which is in consonance with the idea that a constant computer usage and gaming, probably, increase the predisposition to be immersed and, subsequently, to experience presence. As current research highlights that gaming platform and game controllers may influence immersion,37,38 assessing only individuals' immersive tendencies and motion sickness propensity might be a limited approach.
Adopting these user typologies will be possible to standardize the provision of technical resources for the psychotherapeutic process. Furthermore, as game controllers used in a specific virtual reality exposure therapy (VRET) may impact on immersion and cybersickness, patients with low computer skills, with no gaming expertise, and who are used to different game controllers should go through a familiarization stage before VRET to reduce cybersickness symptoms, dropouts, and subsequent treatment failure. 39 However, these results should be interpreted with precaution.
One of the main limitations of this study concerns the nature of sample selection and size. As our sample was composed only of university students, a wider spectrum sample is required to generalize our results. Besides, some individual factors (e.g., user's anxiety trait or level of fatigue) were not controlled and therefore might influence user's attention and how VRE was perceived.40–42
Future studies with the combined use of eye tracking and VRE might provide more information about this issue.43,44 Additionally, and given that keyboard and mouse were the game controllers used in this study, gamers who were proficient in playing with such controllers might have had less cybersickness symptoms due to an easier navigation in the VRE.
Accordingly, individual characteristics here analyzed cannot be seen as crystallized factors but that they have to do with previous user's experience and habits, supporting the idea that immersion tendency and cybersickness might be both trainable. It might also be possible that the combined use of HMD with keyboard/mouse controllers should be rethought in console gamers and nongamers, at least at first stages, as the wrong game controller, that is, a controller that the user is not used to deal with, might hinder the VR experience.
Therefore, and transposing these results to clinical practice, it should be possible to allow the user/patient to choose his/her preferred game controller. It would be also of interest in further research to examine the effect of the use of different game controllers in VREs (e.g., Move for PlayStation 4® or Kinect for Xbox One®) as a function of the game controller usually used by the user. Besides, measures of task performance should be implemented in future experiments to understand better the results of ITQ and SSQ measurements.
Conclusion
This study found relevant associations between variables related to the VR experience. Older users with a low tendency to immersion and high cybersickness symptoms are linked to console gamers and nongamers. Based on our findings, these typologies provide some guidelines to researchers and therapists as VRE effectiveness might be higher for certain types of users. However, the individual characteristics assessed in the present study cannot be seen as if they are stable traits associated with a stagnant technology.
To get the maximum of a VRE, users should be immersed and experience high levels of presence without any severe cybersickness symptoms. In the cases that patients show high resistance to computers and/or are nongamers, a pretraining phase in a neutral VRE or providing more suitable technical resources (e.g., the game controller he/she is used to) might better predispose users to become immersed in VREs.
Note
a. “This procedure was performed through SPSS, Optimal Scaling→ multiple correspondence analysis.”
Footnotes
Author Disclosure Statement
No competing financial interests exist.