
Abstract
Abstract
Although cognitive behavioral therapy (CBT) has been demonstrated to be the most effective approach for the treatment of bulimia nervosa (BN), there is lack of studies showing whether a combination with a serious video game (SVG) might be useful to enhance patients' emotional regulation capacities and general outcome. The aims of this study were (a) to analyze whether outpatient CBT + SVG, when compared with outpatient CBT − SVG, shows better short-term outcome; (b) to examine whether the CBT + SVG group is more effective in reducing emotional expression and levels of anxiety than CBT − SVG. Thirty-eight patients diagnosed as having BN according to DSM-5 criteria were consecutively assigned to two outpatient group therapy conditions (that lasted for 16 weekly sessions): 20 CBT + SVG versus 18 CBT − SVG. Patients were assessed before and after treatment using not only a food and binging/purging diary and clinical questionnaires in the field of eating disorders but also additional indexes for measuring anger expression and anxiety. Regarding the post-treatment psychometric measures, most of the mean differences (Eating Disorder Inventory-2, Symptom Checklist-Revised, State-Trait Anxiety Index, and partially State-Trait Anger Expression Inventory) achieved moderate to high effect size (d > 0.5), in the sense that CBT + SVG obtained the best results compared with the CBT − SVG group. Regarding therapy outcome (dropout, partial remission, and total remission), CBT + SVG showed better results and a moderate effect size emerged for the comparison of the risk of dropout during the treatment, being higher for CBT − SVG compared with CBT + SVG (44.1 percent versus 20.0 percent, d = 0.54). Although the sample size in our study was low, and consequently results should be considered with caution, we have obtained promising findings suggesting that in the short-term CBT + SVG might be a good option not only for improving emotional dysregulation and approaching the current limitations of CBT − SVG in BN but also for enhancing the therapy adherence of patients.
Introduction
C
In recent years, to enhance the current effect of CBT in ED, there has been a significant expansion in complementary new technological approaches for addressing and promoting self-control strategies,8,24 compliance, and adherence to therapy25,26 as relapse prevention strategies 27 and for increasing accessibility of nontreatment-seeking patients.28,29 The approaches explored are ranging from web-based interventions,30–33 text messaging, 25 smartphone applications,8,34 and virtual reality35,36 with promising results. Serious video games (SVGs) have been shown to be useful as complementary tools in the clinical field. These video games are designed with a specific purpose that goes beyond purely entertainment. SVGs can be applied, for example, to improve the individual's skills, attitudes, and knowledge.37,38 In healthcare, SVGs have been applied with different clinical goals such as obesity prevention and intervention, 39 behavioral improvements in adolescents and young adults with cancer, 40 the prevention of alcohol and drug use in adolescents, 41 and the rehabilitation of people with mild cognitive impairment, Alzheimer's disease, and related disorders. 42 SVGs and some brain therapies have also been found to have potential positive effects for managing emotional regulation in other conditions and disorders43–46 and even in some series of treated ED cases.47,48 However, there is a lack of controlled studies where this type of approach was analyzed.
The specific aims of the present study are twofold: (a) to analyze the short-term effectiveness of using a combined outpatient treatment (CBT with SVG: CBT + SVG) in BN when compared with a traditional outpatient therapy (CBT without SVG: CBT − SVG); (b) to examine whether the CBT + SVG group is more effective in reducing short-term impulsivity, emotional expression, and levels of anxiety than the CBT − SVG group.
We hypothesized that the finding of approaching impulsivity and coping with emotional distress, by means of CBT + SVG, may help ED patients improve not only these traits but also general psychopathology. Therefore, we expect the CBT + SVG group to exhibit more clinical improvement than the CBT − SVG group. Likewise, we expect to find a higher risk of dropout in the CBT − SVG condition.
Materials and Methods
Participants
The present quasi-experimental design study includes 38 female BN patients, who fulfilled the DSM-5 criteria 49 following a semistructured interview adapted from SCID-I interviews. 50 Participants were consecutive referrals for assessment and treatment at the Department of Psychiatry of the Bellvitge University Hospital in Barcelona (Spain). The average age of the initial sample was 29.5 years (SD = 9.9). The average duration of the disorder was 9.9 years (SD = 7.4) and the mean weekly binge and purging frequencies were 4.8 episodes (SD = 3.6) and 4.9 episodes (SD = 6.9), respectively. The mean body–mass index (BMI) of the total sample was 25.47 (SD = 5.89) and 21.2 percent of the sample was obese (i.e., BMI >30). The participants who fulfilled the inclusion criteria were consecutively assigned to either the CBT + SVG group or the CBT − SVG condition. Inclusion criteria were being females aged between 18 and 55. Exclusion criteria at intake were as follows: being male, having primary psychiatric or neurological disorders (e.g., psychotic disorders, bipolar disorder, substance abuse dependence, epilepsy) that may affect the game performance and the monitored physiological and emotional reactions, an active pharmacological therapy that may interfere with the game performance, and current diagnosis of Internet or video game addiction, measured by means of Young's diagnostic criteria for Internet addiction and a specific scale assessing video game addiction, which was developed in our service and is based on the DSM-IV criteria for pathological gambling and on the scale of Griffiths and Hunt to measure the level of video game dependence. Written informed consent was obtained from all participants and the Ethics Committee of the University Hospital of Bellvitge approved the study (Ref. PR112/08).
Assessment
For the assessment, commonly applied questionnaires in the field of ED comprising the Eating Disorder Inventory-2 (EDI-2), 51 the Symptom Checklist-Revised (SCL-90-R), 52 State-Trait Anxiety Index (STAI), 53 and State-Trait Anger Expression Inventory-2 (STAXI-2) 54 were employed. In addition, throughout the duration of the treatment, patients kept a daily food and purging diary. 55 Assessments were made pre- and postgroup therapy.
Eating Disorder Inventory-2
This is a reliable and valid 91-item multidimensional self-report questionnaire 51 that assesses different cognitive and behavioral characteristics, which are typical in ED. The EDI-2 retains the 64 items grouped into eight scales. All of these scales are answered on a six-point Likert scale and provide standardized subscale scores. In the current study, the total score was used as a measure of ED severity. When this instrument was validated in a Spanish population, 56 a mean internal consistency of 0.63 (coefficient alpha) was found.
Symptom Checklist-Revised
This test 52 contains 90 items and helps measure nine primary symptom dimensions and three global indices, which are a Global Severity Index, designed to measure overall psychological distress; a Positive Symptom Distress Index, designed to measure the intensity of symptoms; and a Positive Symptom Total (PST), which measures self-reported symptoms. All these three measures of global psychopathology were the scales of interest in our study. This scale has been validated in a Spanish population, 57 obtaining a mean internal consistency of 0.75 (coefficient alpha).
State-Trait Anxiety Index
This is a self-report questionnaire 53 that includes 40 items on a four-point rating scale, measuring state anxiety (20 items) and trait anxiety (20 items). Minimum and maximum scores range from 20 to 80 points. The set of questions value feelings of anxiety and depression in the areas of worry, tension, and apprehension. The STAI was validated in the Spanish population with Cronbach's alpha coefficients ranging between 0.90 and 0.94. 58
State-Trait Anger Expression Inventory-2
This test 54 contains 44 items that examine the experience and expression of anger. This instrument was validated in a Spanish population with Cronbach's alpha coefficients ranging between 0.63 and 0.95 and it comprises 49 items. 59 It entails three main global scales: State Anger; Trait Anger, and Anger Expression Index (AEI), which provides a general index of the expression of anger. Items are rated on four-point Likert scales assessing either the intensity of the angry feelings or the frequency with which anger is experienced, expressed, suppressed, or controlled. A higher score is always indicative of greater levels of the assessed anger construct.
Procedure
Following assessment and diagnosis conducted by experienced psychologists/psychiatrist, patients received one of the following treatment options: Option 1 (treatment as usual, namely CBT − SVG) and Option 2 (enhanced combined therapy: usual CBT + SVG).
Option 1: Usual therapy (CBT − SVG)
As described in previous studies, 11 our CBT outpatient treatment consisted of 16 outpatient 90-minute weekly sessions in a group therapy setting. The group was directed by a psychologist and a cotherapist. This program and accompanying program material have already been manualized and published in Spanish. 55
Option 2: Combined therapy (CBT ± SVG)
Each SVG session was carried out consecutively once a week, for 10–12 weeks, on the day of patients' usual CBT therapy. As described in previous studies,47,48 the SVG (PlayMancer) takes place in an island in which the subject must progress and move forward based on the achievement of a number of therapeutic targets (Fig. 1) developed along three minigames, where the final goal is to increase emotional self-control skills in patients and self-control over their general urgency to act. In this SVG, several components are integrated such as biosensors for monitoring physiological reactivity and a camera that continuously tracks the emotional state of the player. When negative emotions or hyperarousal physiological reactions are detected by the SVG, the game immediately directs the avatar to a relaxed area with the goal to calm down. During the whole game session, higher undesired emotional and/or physiological reactions are coupled with greater difficulty to reach the end goals of the video game (Fig. 2). Each session lasts 20 minutes and relaxing music is played for 3 minutes before and after the session starts.
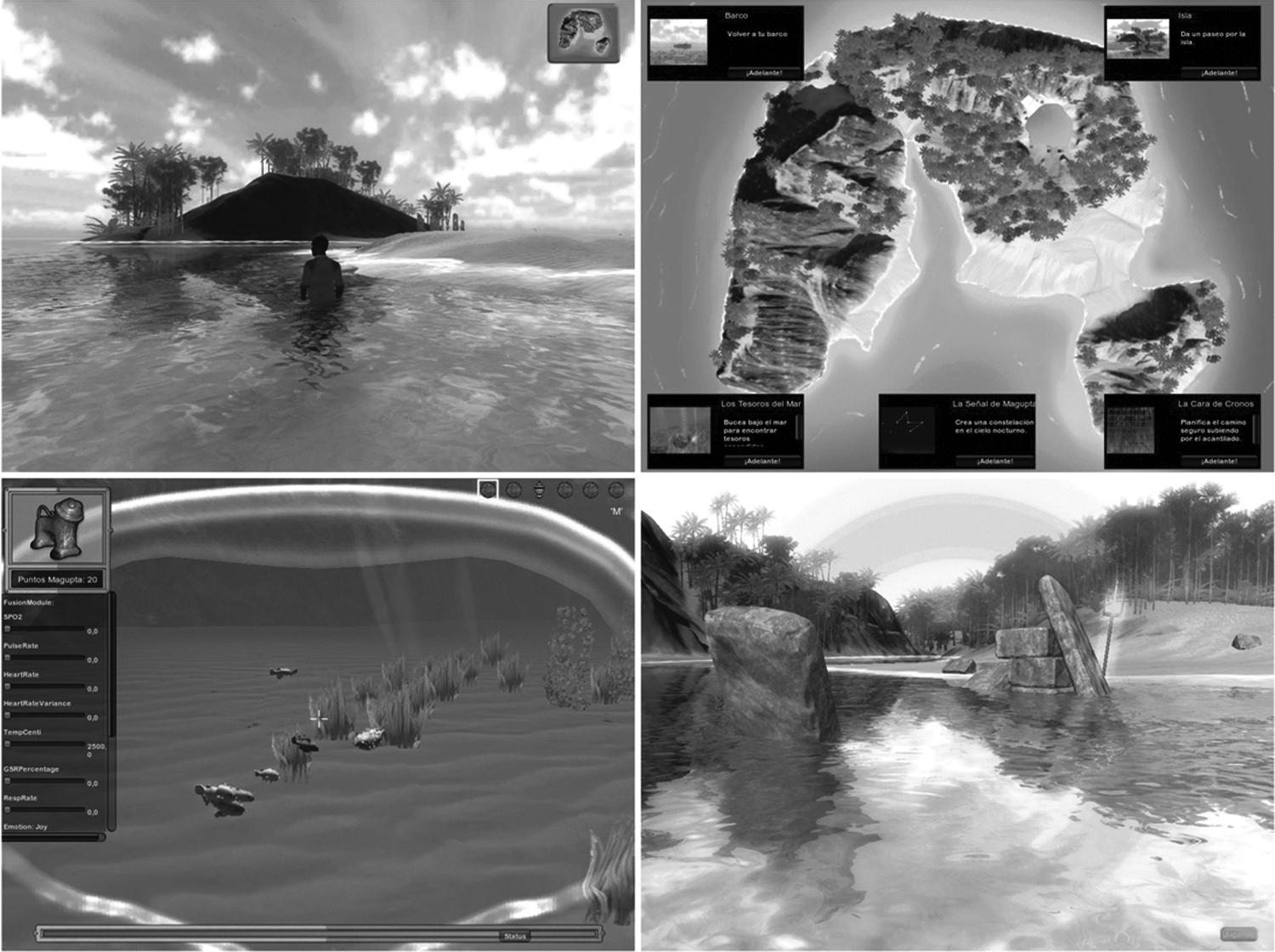
Examples of scenarios in this SVG: Islands. SVG, serious video game.

SVG used in the current study, where physiological and emotional recognition aspects were monitored.
Patients who completed the treatment were assessed at the end of CBT therapy and at 3 months followup and categorized in three groups: total remission, partial remission, and no remission (including those participants who dropped out), defined as per previous studies. 11 Primary outcome was based on the food and purge diary and the response of some clinical questionnaires in the field of ED. The working definition of a full remission outcome required the absence of binging and purging (laxatives and/or vomiting) behaviors for at least 4 (consecutive) weeks and psychological improvement measured by clinical questionnaires during the last 3 months after the end of therapy. Partial remission was defined as substantial symptomatic improvement, but still with the presence of symptoms according to previous criteria, and no remission was defined as no symptomatological improvement or dropout.
Statistical Analyses
Analyses were carried out with SPSS20 for Windows. t Test procedures compared the quantitative outcomes analyzed in this study between the two treatment conditions (CBT − SVG versus CBT + SVG), and χ2 tests compared the therapy outcome (grouped as dropout, partial remission, or total remission) between groups. The Kaplan–Meier method estimated the cumulative survival function for the event “dropout during the therapy.” Kaplan–Meier is a procedure included into the survival analyses methodology, which involves the modeling of time-to-event data, whereby death (or failure) is considered an event (in this study, the register of the dropout), allowing censored values (in this study, right censored data identified patients who did not dropout, that is, those who stayed for the entire treatment). A threshold level of p < 0.05 was fixed to consider significant results. However, since the low sample size in this study involves low statistical power, all the comparisons were accompanied with the Cohen's d coefficient, which is not related to sample size and gives the measure of the effect size between mean and proportional differences (moderate effect was considered for |d| >0.5 and high for |d| >0.8).
Results
Clinically relevant characteristics
No statistical differences were found between the two clinical groups for any clinically relevant variables (namely age of onset, duration of the disorder, average weekly frequency of binge/purging behaviors, and number of previous treatments) assessed (Supplementary Table S1; Supplementary Data are available online at
Bold: significant comparison (p < 0.05).
Moderate (|d| > 0.5) to high effect size (|d| > 0.8).
AEI, Anger Expression Index; CBT, cognitive behavioral therapy; EDI, Eating Disorders Inventory; GSI, Global Severity Index; PSDI, Positive Symptom Distress Index; PST, Positive Symptom Total; SCL, Symptom Checklist; STAI, State-Trait Anxiety Index; STAXI, State-Trait Anger Expression Inventory; SVG, serious video game.
Treatment outcome and dropout rates
As shown in Table 2, when comparing both groups on the therapy outcome (dropout, partial remission, and total remission), no statistical difference emerged in the global χ2 test (p = 0.22). However, a moderate effect size was found in the comparison of the risk of dropout during the treatment, being higher for CBT − SVG compared with CBT + SVG (44.1 percent versus 20.0 percent, |d| = 0.54).
Bold: Moderate (|d| > 0.5) to high effect size (|d| > 0.8).
Survival analyses showed that the rate of dropout during the therapy was higher for CBT − SVG compared with CBT + SVG (Fig. 3). Cumulative survival functions showed similar slopes–trends only between sessions 1 and 2 (around 5 percent of patients had dropped out by this time in both groups, cumulative survival around 95 percent). The remaining dropouts in the CBT + SVG group were registered at sessions 3 (cumulative survival equal to 85 percent at this time) and 7 (cumulative survival 80 percent). For the CBT − SVG group, dropouts after session 2 were registered at session 6 (cumulative survival 78 percent), 8 (cumulative survival 72 percent), 10 (cumulative survival 61 percent), and 11 (cumulative survival 56 percent).

Cumulative functions comparing the survival time to dropout by therapy. Y-axis represents the probability estimates and X-axis the number of the session.
Discussion
The main goal of this study was to examine the short-term effectiveness of enhanced CBT in BN when using complementary SVGs. The current study is a novel contribution to the literature on the usefulness of new technologies, specifically SVGs, for regulating emotions in ED and mental disorders.
The first main finding of the study is that adding the use of SVGs yielded better results for improving ED and general psychopathology than in the case of CBT − SVG. These results are in concordance with previous studies where a supportive therapy based on new technologies was applied to enhance CBT performance.7,33,35 Although both groups showed no statistically significant differences on general therapy outcome, the performance in the CBT + SVG group was better compared with the CBT − SVG group (50 percent vs. 28 percent, respectively) and even the rate of dropouts was lower in the former group. Although the sample size in our study was low and, consequently, the statistical power was poor, results should be considered with caution; in concordance with previous literature, 60 it showed that new technologies are a good option for enhancing usual CBT and increasing therapy adherence. The dropout rates were much lower than those described in the bulimic disorders literature11,61 that showed the range to be from 30 percent to 45 percent after an outpatient group therapy.
The second main finding was that when considering other noneating-related targets, such as anxiety and anger expression, the CBT + SVG group showed more improvement, namely in lower anxiety and higher capacity for expressing emotions, than the CBT − SVG group. Although there is a lack of study in the literature that analyzed the effects of SVGs in emotional regulation deficits of mental disorders,47,48,62 the few studies where these secondary targets were addressed, by means of additional emotional regulation tools for the therapy of ED, have also shown promising results.18–20 Our patients were able to improve emotional regulation capacities after the combined therapy. Whereas the CBT − SVG group still showed clinically relevant emotional dysregulation even after CBT (average score of AEI located in PC8059 when looking at normative data), the group of CBT + SVG reached normal emotional regulation levels (an average score of PC40). This result supports the finding of previous studies where the limited capacity of usual CBT for improving underlying personality and emotional traits 13 was evident. In this sense, new technology, namely SVG as used in this study, has shown its potential in modifying emotional dysregulation in ED. The underlying reasons behind positive effects of using SVGs were already described and contextualized in different studies,43–48 namely own internal positive features (intensiveness, isolation from outside world, immersive capacity, low resistance to be used) and their potential beneficial effects in brain activity.44,63–68
Due to its exploratory nature, there are several limitations of the present study that need to be considered: (a) although we have obtained some novel and relevant findings that suggest the potential of using SVGs, the small sample size of our groups limited the final statistical power of the analyses; (b) the short-term nature of the study does not allow to examine their middle long-term effect; (c) the design used, where no active control condition was used in the CBT − SVG group (e.g., a rehabilitation/relaxation standard VG), could introduce some procedural bias.
Finally, it can be concluded that adding SVGs may help enhance CBT effects not only in bulimic patients, namely in emotional dysregulation, eating severity, and psychopathology, but also in improving adherence to therapy. How far this finding is due to the properties of the SVG itself or to the fact that emotional dysregulation has directly been focused could not be demonstrated in the current study. In future studies, more controlled designs should be applied to control the procedure used (e.g., comparing with a control group where emotion-focused therapy, DBT, or active SVG approach is being used). From a clinical perspective, the main implications of our study are twofold: first, new technological approaches, namely SVGs, might be a good approach for enhancing CBT and for overcoming its current limitations; second, emotional dysregulation may need to be a specially focused target in therapy to be modified.
Footnotes
Acknowledgments
Partial financial support was received from FIS (PI11/00210; PI14/290), Fondo Europeo de Desarrollo Regional (FEDER), AGAUR (2014 SGR 1672), and PROMOSAM (PSI2014-56303-REDT). CIBER Fisiopatología de la Obesidad y Nutrición (CIBERObn) and CIBER Salud Mental (CIBERSam) are both initiatives of ISCIII. The authors would like to thank PlayMancer consortium for their contribution in developing this Platform and SVG. This work is part of the PhD thesis of Cristina Giner-Bartolome (supported by Ayudas Predoctorales de Formación en Investigación en Salud-PFIS: FI12/00470) at the University of Barcelona (School of Medicine).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.