
Abstract
Abstract
Maintaining employment is difficult for patients with schizophrenia because of deterioration of psychosocial and cognitive functions. Such patients usually require vocational rehabilitation training, which is both demanding and costly. In this study, we developed a virtual reality-based vocational rehabilitation training program (VR-VRTP) for such patients and evaluated its feasibility as an alternative to traditional rehabilitation programs. We developed the VR-VRTP to include various situations commonly encountered in two types of occupations: convenience store employee and supermarket clerk. We developed practical situations, as well as a system for providing feedback, to ensure patients would not lose interest during training. Nine participants each performed the VR-VRTP repeatedly per week for a total of 8 weeks. At baseline and after training, all participants were evaluated using the following clinical and neuropsychological tests: Manchester Scale, Clinical Global Impression, Personal and Social Performance Scale (PSP), Hamilton Depression Rating Scale, Zung Depression Rating Scale, Beck Anxiety Inventory, Wisconsin Card Sorting Test, Stroop Test, Rey–Osterrieth Complex Figure Test (RCFT), and Auditory Verbal Learning Test (AVLT). After training, patient scores improved on the PSP, general symptoms on the Manchester Scale, AVLT, and delayed recall on the RCFT. The Manchester positive symptom score showed a trend of improvement. No significant changes were observed for other measures. The VR-VRTP may improve general psychosocial function and memory, potentially influencing real-world vocational performance. These findings provide preliminary evidence regarding the utility of the VR-VRTP in patients with schizophrenia.
Introduction
S
Virtual reality programs previously used in the treatment of various diseases10–12 may be considered as a cost-effective alternative to individual vocational rehabilitation training. Virtual reality-based programs have the advantage of being able to organize diverse program scenarios based on real-life situations, and the patient can experience multiple predictable situations and efficiently master appropriate methods of response. In other research, 10 virtual reality-based vocational training resulted in superior post-training cognitive function compared with vocational training conducted by a therapist.
Therefore, this study aimed to develop a virtual reality-based vocational rehabilitation training program (VR-VRTP), which patients with chronic schizophrenia can both understand and apply in real life, and to evaluate the feasibility of this program.
Methods
Participants
Participants were diagnosed with schizophrenia using the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition-text revision (DSM IV-TR). 11 All patients were recruited through the Outpatient clinic at the Psychiatric Department of the SMG-SNU Boramae Medical Center or the Dongjak District Community Mental Health Center. Inclusion criteria included the following: between the ages of 20 and 55; at least middle school education; desire for vocational rehabilitation training; and ability to give written informed consent. Those with physical disabilities that would make it difficult to engage in the program, those with a history of alcohol or other substance abuse disorders within the past month, and those with intellectual disabilities or other neurological or developmental disorders (other than chronic mental illness) were excluded. As a result, 10 patients were selected. Clinical evaluations performed by a psychiatrist before the VR-VRTP confirmed the diagnosis of schizophrenia, with eight patients having the paranoid subtype and two having the undifferentiated subtype. All participants provided their written informed consent. The Institutional Review Board of the SMG-SNU Boramae Medical Center approved this study protocol.
VR-VRTP
We composed virtual reality scenarios for both convenience store and market environments, in which schizophrenic patients are considered likely to be employed. Before entering a specific scenario, patients received training in presenting a good image, including training in greeting posture, smiling, and common verbal greetings. In the case of verbal greetings, patients spoke directly into a microphone, and their voices were recorded and played back so that the patients could hear their own voices to modify themselves. As the specific role of the scenario, participants selected solutions to problematic situations onscreen, after which they were given feedback. At the end of the training, final scores were displayed so that patients could feel a sense of accomplishment when their scores improved. The details of the scenarios are provided in Table 1. The convenience store scenario required ∼20 minutes to complete, while the market scenario required ∼15 minutes to complete, including the time required to give feedback during each scenario. Participants performed the VR-VRTP repeatedly per week for a total of 8 weeks with two scenarios. Screenshots from the virtual reality-based vocational rehabilitation training are provided in Figure 1.
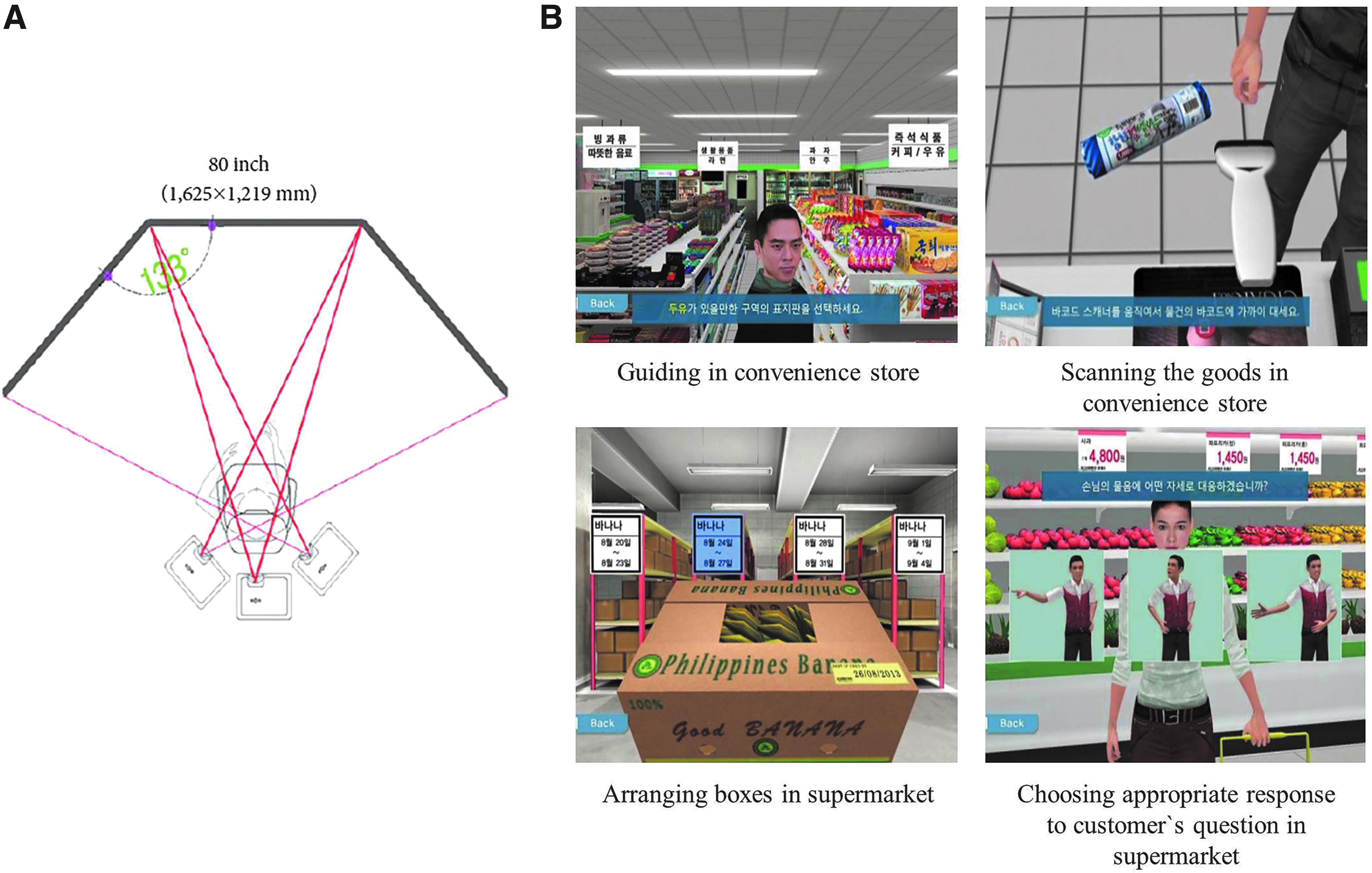
Illustration of projection wall system
A three-dimensional surround screen using three LX400 LCD digital projectors (Christie Digital Systems, Cypress, CA) was installed in the immersion room at the SMG-SNU Boramae Medical Center. Patients used a mouse to move and respond about the virtual space displayed on the screen (Fig. 1).
Measures
We measured participants' clinical conditions and cognitive functions at baseline and after the 8-week training period. For clinical condition, Manchester Scale, 12 Clinical Global Impression-Severity (CGI-S), 13 Clinical Global Impression-Improvement (CGI-I), 13 Personal and Social Performance Scale (PSP), 14 and Hamilton Depression Rating Scale (HAM-D)15,16 were used by a psychiatrist, and self-ratings were obtained using Zung Depression Rating Scale (ZDRS) 17 and Beck Anxiety Inventory (BAI).18,19 For cognitive function, Wisconsin Card Sorting Test (WCST) 20 and Stroop Test for executive function,21,22 Rey–Osterrieth Complex Figure Test (RCFT) for visual memory,23,24 and the Korean Version of the Auditory Verbal Learning Test (K-AVLT) for verbal memory23,25 were administered by a psychologist.
Statistical analysis
The Wilcoxon signed-rank test was used to compare changes in clinical condition and cognitive function between pre- and posttest measurements. p Values less than 0.05 were considered significant. Among the factors considered for neurocognitive evaluation, the t-score signifies a converted score appropriate to age with an average of 10 and a standard deviation (SD) of 3, and percent refers to the age-equivalent percentage. Age equivalent t-scores or percent were obtained for the Stroop Test, RCFT, and K-AVLT measures. However, as there are no data for the Korean equivalent of the WCST, raw scores were used. The data analysis was performed using SPSS version 20.0 (SPSS, Inc., Chicago, IL).
Results
Ten subjects were registered according to the recruitment standards presented in the Methods section; however, one female with paranoid subtype (no occupation) declined to participate and a total of nine patients participated in the study to completion. The average age of the participants was 36.65 (SD = 5.41) years, with an average educational attendance of 12.11 (SD = 2.62) years. All nine participants (four female, five male) were unmarried. One male was employed as an unskilled laborer, while the remaining participants were unemployed.
At baseline, the average PSP score of participants was 60.56, while the average CGI-S score was 3.11, suggesting that the participants had mild stable symptoms of schizophrenia. Significant pre- to postprogram changes were observed on both the general symptoms score of the Manchester Scale (p = 0.025) and the PSP score (p = 0.046). No significant differences were observed in scores on the HAM-D, CGI-S, ZDRS, and BAI (Table 2). The positive symptom score of the Manchester Scale showed a trend of statistical improvement (p = 0.059, Table 2). The average CGI-I score was 3.56.
Values are mean (standard deviation). p Value (two tailed) of z-score on the Wilcoxon signed-rank test.
p < 0.05.
BAI, Beck Anxiety Inventory; CC, category complete; CGI-I, Clinical Global Impression-Improvement; CGI-S, Clinical Global Impression-Severity; D recall, delayed recall; HAM-D, Hamilton Depression Rating Scale; I recall, immediate recall; K-AVLT, The Korean version of Auditory Verbal Learning Test; PSP, Personal and Social Performance Scale; raw, raw score; RCFT, Rey–Osterrieth Complex Figure Test; t, t-score; WCST, Wisconsin Card Sorting Test; ZDRS, Zung Depression Rating Scale.
The pre- and postprogram evaluations of neurocognitive function were conducted using the WCST, Stroop Test, RCFT, and K-AVLT. Patients did not demonstrate a statistically significant change of WCST and Stroop Test scores. However, the memory scores on both the immediate recall (p = 0.037) and delayed recall (p = 0.026) portions of the RCFT and on the first (p = 0.007) and fifth (p = 0.012) attempts of the K-AVLT increased significantly (Table 2).
Discussion
This study conducted preliminary research for the development of a VR-VRTP reflective of real-life situations and applicable to patients with schizophrenia. As a result of administering the VR-VRTP to patients with schizophrenia, we observed improvements in their clinical condition as measured using the PSP and the general symptom section of the Manchester Scale. Evaluation of their neurocognitive functions revealed additional improvements in visual and verbal memory capabilities.
Applications of the virtual reality technology have been expanding in the field of psychiatry as a means of dealing with training environments. Through this simulated reality, the program can recreate stimuli that are relatively difficult to provide directly in real life. In addition, the level of exposure can be controlled, and repeated training is simple. Moreover, when systematized programs with an instruction manual are administered, reliance on the competence of the therapist is diminished, and costs, including personnel expenses, can also be reduced. Given these advantages, these kinds of virtual reality-based programs have been applied in prior research for the treatment of phobias, 26 distorted body image, 27 childhood autism, 28 and in smoking cessation 29 and gambling addiction programs. 30 One of prior studies 31 administered a virtual reality program to schizophrenia patients to evaluate cognitive flexibility. The results were similar to prior observations that the patients with schizophrenia exhibit more concrete thinking than a control group. Other report 10 indicated that those who took part in the virtual reality-based vocational training for schizophrenia patients exhibited positive improvement in the WCST compared to either those in the traditional program with therapist or in the control group. Based on these results, we may anticipate that the virtual reality-based programs either do not show a significant difference in effectiveness compared to previous training programs or can be expected to be superior.
To date, researches have reported the link between performance in vocational activities to psychiatric symptoms and cognitive function.32,33 McGurk et al. 34 reported that lower levels of negative symptoms and higher scores on pre- and postemployment program measures of executive function and language learning ability were associated with greater numbers of hours worked and higher wages. Moreover, higher levels of positive symptoms resulted in the patients' receiving additional assistance, while great executive function, concentration, and psychomotor abilities allowed patients to receive less assistance during the program.
In the case of the VR-VRTP developed for this study, the patients' PSP scores and visual and verbal memory functions improved significantly and their positive symptoms showed a trend of statistical improvement. As such, we may predict that the effects of the program can be anticipated to translate to actual vocational activity. Moreover, while there was no statistically significant change in the HAM-D score, there was a significant change in the general symptoms score of the Manchester Scale indicating that a positive influence on the patients' subjective experience of depression or anxiety can be anticipated as a result of participation in the program. However, although there were no significant changes of scores for the WCST or Stroop Test compared to other studies, it is possible that the participants had mild level of schizophrenia or relatively short training period to improve executive function. In reviewing these results, we believe that the VR-VRTP may provide help in the improvement of overall function associated with the social rehabilitation of patients with schizophrenia.
The limitations of this study are as follows. This study involved the small number of patients, and relatively short program duration may have made it difficult to observe many significant effects and generalize the results of this study. There was no control group; the object comparison of the effects of VR-VRTP is difficult with vocational training using traditional program with therapist or program with other tools. For evaluating severities of the psychiatric symptoms of schizophrenia, more detailed scales are needed. Even though the participants had relatively mild and stable symptoms, medication changes were not directly controlled. In addition, while there were no significant changes in scores on WCST or Stroop Test, improvements in the recall scores in RCFT and K-AVLT may have been influenced by learning effect from the baseline trials. In future study, a randomized controlled study with more participants will be needed.
This study is a meaningful work that develops the VR-VRTP reflective of real-life situations in Korea and applies it toward the patients with schizophrenia. The VR-VRTP may become a new rehabilitation program in community mental health centers, hospitals, or other related facilities, particularly in understaffed locations. Future programs can be improved by including more realistic characters and places and training in more diverse jobs and experiences. Further modifications of the level of difficulty according to the subject's level of cognitive function and severity of clinical condition also should be developed.
Footnotes
Acknowledgments
This research was made possible by a research grant from the SK Telecom Research Fund (Grant No. 16-2013-91). Development of the VR-VRTP was assisted by FNI Co., Ltd. (Gyeonggi Province, Korea), to whom we express our thanks.
Author Disclosure Statement
No competing financial interests exist.