
Abstract
Abstract
Self-regulation strategies are helpful for increasing goal commitment and maintaining behavior change. Evidence suggests that the self-regulation strategy of mental contrasting with implementation intentions (MCII) shows promise in helping people increase their physical activity. The purpose of this research was to investigate whether these self-regulation strategies would increase physical activity, which would, in turn, improve well-being and mental health. In a quasi-experimental study, participants were randomized by school to an experimental group (n = 40) and control group (n = 45). The experimental group received self-regulation strategies, whereas the control group did not. Both groups were given a Fitbit and the goal of 10,000 steps per day. Participants' well-being and depressive, anxiety, and stress symptoms were measured at baseline and after the 3-week intervention. The experimental group's physical activity increased from 7,938 to 9,288 steps per day (p = 0.001), whereas that of the control group did not increase. In the experimental group, the findings suggested a significant increase for men, and a nonsignificant increasing trend for women. The study demonstrated the benefits of self-regulation strategies such as MCII on achieving physical activity goals. Findings also suggested that self-regulation strategies provided improvement beyond physical activity by decreasing the depressive symptoms of female participants in the experimental group. Given the small sample size, effects by gender have to be interpreted with caution. Limitations and suggestions for future research are discussed.
Introduction
U
Although studies have examined the impact of self-regulation strategies on physical activity,6,7 and have investigated the relationships between physical activity and well-being,8–10 there is little research examining the influence of self-regulation strategies on both physical activity and well-being. In this study, the combined effectiveness of two self-regulation strategies in increasing physical activity, well-being, and mental health was examined.
The first strategy involved regulating goal pursuit through mental contrasting with implementation intentions (MCII). During mental contrasting, individuals mentally elaborate a desired future (e.g., getting fit) and then identify and imagine obstacles of reality that prevent them from attaining the envisioned future (e.g., not being organized).11–13 Implementation intentions is a final step that involves developing an if–then plan to overcome the obstacle. 14 MCII has helped people with high expectations of success to achieve their goals across various interpersonal, achievement, and health domains by creating strong goal commitment with subsequent goal striving and goal achievement.15–17 MCII has also helped individuals with mild to moderate symptoms of depression to reach their activity-related goal. 13
The second strategy deployed was prompt self-monitoring, which involved daily reminders of goals. Michie et al. examined whether the following five techniques—prompt intention formation, prompt specific goal setting, provision of feedback on performance, prompt self-monitoring of behavior, and prompt review of behavioral goals—were more effective than other techniques in improving physical activity and healthy eating. 4 They found that interventions combining self-monitoring with at least one of the mentioned five techniques were significantly more effective than other interventions. In this study, we utilized one of the strategies mentioned—prompt self-monitoring of behavior. Hence, the first objective of this research was to investigate the effects of the combined self-regulation strategies of MCII and self-monitoring on physical activity.
Researchers using the strength model of self-regulation demonstrated that self-regulation depends on a common resource, and that improvements in one area of self-regulation can bring improvements to other areas. 18 For example, researchers reported that participants who worked on adhering to a physical activity program found benefits in other areas of their life, including having a more healthy diet, reducing impulsive spending, and reducing perceived stress and emotional distress. 19 Johannessen et al. also found a transfer effect wherein mental contrasting of a dieting wish improved not only self-reported eating behavior but also self-reported physical activity. 11
In this study, another objective was to examine whether effects of the combined self-regulation strategies in enhancing physical activity would extend to well-being and mental health. Specifically, we tested the hypothesis that the combined self-regulation strategies would increase physical activity, which would, in turn, improve well-being and mental health.
Method
Study design and participants
Ethics approval was given by the IRB of Nanyang Technological University. Participants, who were students or staff, were recruited through advertisements on notice boards throughout the university campus. Eligibility criteria included age 18–50 years, not having any serious health conditions based on the Revised Physical Activity Readiness Questionnaire, 20 willing to carry the Fitbit every day for 5 weeks during waking hours, and currently exercising <5 hours/week. There were 135 participants from 14 schools within the university who signed up (two schools each with one participant were combined). A school at the university typically represents an academic domain.
Participants were randomly assigned to the experimental or control group by school (Fig. 1). Participants from the same school were assigned to the same condition to prevent possible contamination by discussion between the participants. A hundred participants showed up for the baseline assessment. Six participants could not or declined to participate based on the eligibility criteria described. The objective of the study was to conduct a randomized cluster trial with 43 participants from seven schools in the experimental group and 51 participants from seven schools in the control group.
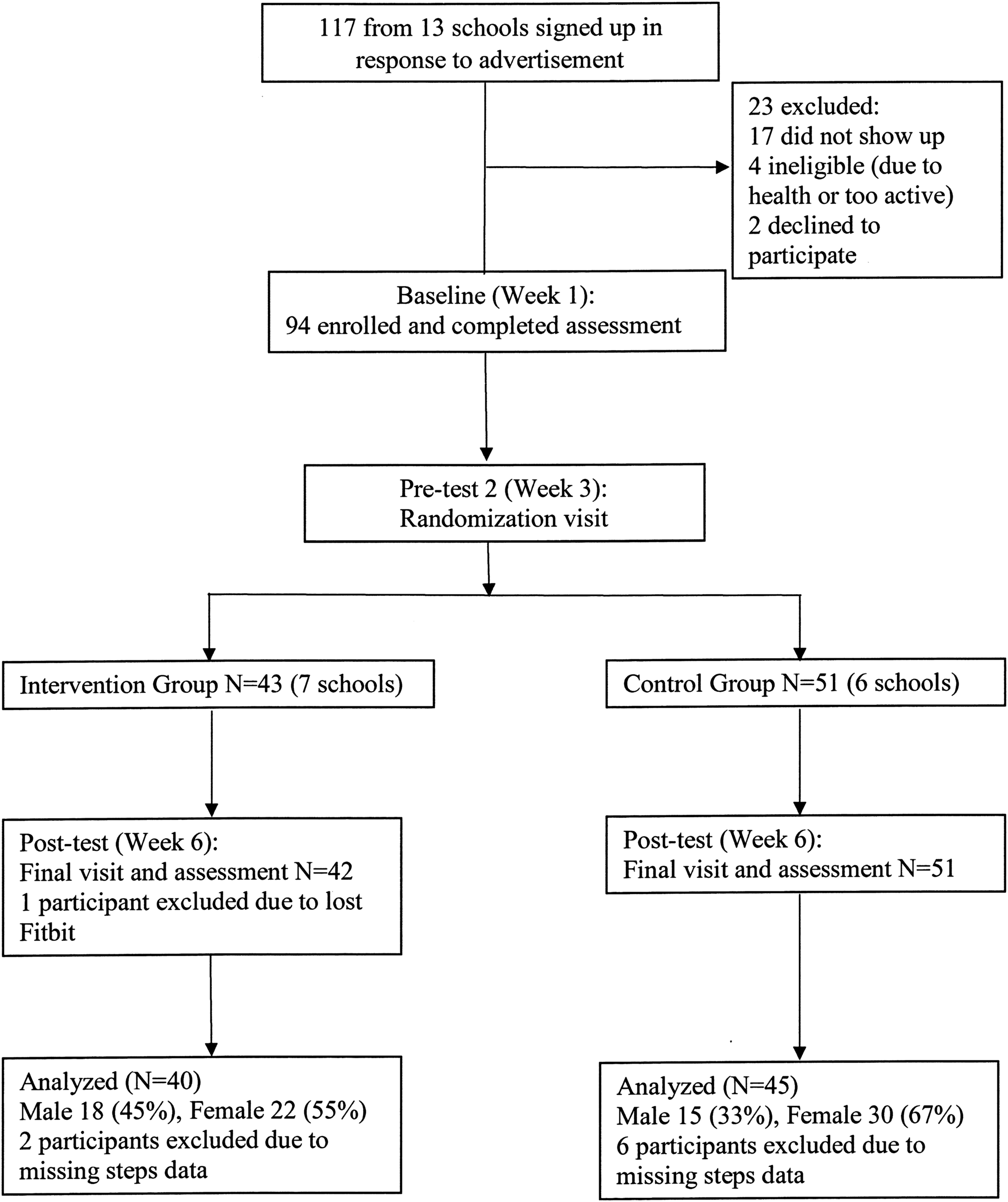
Study flowchart.
However, there were two participants assigned to the control group who mistakenly ended up in the experimental group, and two participants assigned to the experimental group who mistakenly ended up in the control group. The baseline briefings were held at different venues, and it was likely that participants showed up at the wrong venue despite the instructions. Consequently, there were 43 participants from nine schools in the experimental group, and 51 participants from nine schools in the control group.
Eight participants were excluded as they did not meet the criterion of having daily step data for at least half the period; data for the third week were imputed for one participant by carrying forward baseline values as the participant still met the criterion. Baseline weights were imputed for two participants using post-test weight data. The final sample size of this quasi-experimental study was 85 participants from 14 schools; the number of participants from each school ranged from 1 to 19.
Measures
The Fitbit Zip tracker was used to measure participants' physical activity in terms of their daily number of steps. Height and weight were measured using standard procedures. Participants' well-being was measured by the Expanded Satisfaction with Life Scale. 21 Their mental health was measured by the Depression Anxiety Stress Scale-21, 22 which assessed participants' depressive, anxiety, and stress symptoms. Cronbach's alphas for all scales had acceptable internal consistency at each point of data collection (0.675–0.897).
Intervention
As the first objective of the study was to examine the combined effectiveness of two self-regulation strategies—MCII and self-monitoring—the study compared (a) the use of these strategies (experimental group) with the (b) provision of a Fitbit tracker only (control group). Both groups were given a Fitbit, and the goal of 10,000 steps per day. The self-regulation strategies completed by the experimental group but not the control group were MCII and self-monitoring (see Appendix for instructions).
Procedure
Participants attended three sessions: baseline, pretest, and post-test. The purpose of the baseline session was to obtain informed consent, provide the Fitbit devices to the participants, and administer baseline assessments. The baseline was held in lecture theaters or classrooms. The purpose of the pretest, held in computer laboratories 2 weeks later, was to assign participants to the experimental or control group. Both groups were given the following instruction, “your goal for the next three weeks is 10,000 steps per day,” and responded to instruments related to goals; these measures were not analyzed in the study. The session then ended for the control group, whereas the experimental group completed the MCII.
A week later, participants in the experimental group were reminded through e-mail about their 10,000 steps per day goal, asked to complete the MCII again to reinforce the strategy, and given instructions to submit their daily number of steps, as described in the Appendix. Three weeks after the pretest, participants returned for a post-test in computer laboratories; participants returned their Fitbit, completed the assessments as described in the Measures section, and received a $20 voucher for study completion.
Statistical analyses and data management
Baseline characteristics were compared using two-way analysis of variance (ANOVA) to examine any differences between groups and gender. Gender effects were explored as prior research has indicated possible gender effects in pedometer-based interventions. 23 Repeated-measures ANOVA (time × group × gender) were conducted to examine the effects of the intervention on physical activity and psychological outcomes; time consisted of two data points: baseline and post-test. Two-way (group × time) followup ANOVA were conducted to explore significant three-way interactions, and post hoc paired t tests were conducted to examine changes within each group and gender.
The SPSS Macro PROCESS 24 was used to test a mediation model with gender as a covariate and the intervention as the independent variable. The mediator was change in physical activity, which involved subtracting the average daily steps during baseline from the average daily steps during the intervention. The dependent variable used in PROCESS was one of the well-being or mental health measures, that is, change in well-being, or change in depressive, anxiety, or stress symptoms. Data were analyzed from 2015 to 2017.
Results
Baseline characteristics
Participants (N = 85) had a mean age of 23.34 (SD = 5.49; range = 18–44) years with a mean baseline body mass index (BMI) of 22.14 kg/m 2 (SD = 3.81), and groups were not significantly different on key characteristics at baseline. There was a marginally significant group × gender interaction for baseline physical activity (p = 0.074); post hoc analyses indicated no significant differences within each group by gender, and no significant differences within each gender by group.
Controlling for gender, there was a marginally significant difference in pretest depressive symptoms (p = 0.078) with the experimental group (M = 0.69; SD = 0.64) being marginally higher than the control (M = 0.48; SD = 0.38). Controlling for group, there was a marginally significant gender difference on pretest BMI (p = 0.067), with male participants (M = 23.15; SD = 4.29) being marginally higher than females participants (M = 21.50; SD = 3.35). Although not significant, baseline differences suggest that regression to the mean may be a threat to the internal validity of the study.
Mean ages for the experimental and control groups were 22.33 (SD = 3.72) and 24.24 (SD = 6.59) years, respectively. The racial composition for the experimental group was 80 percent Chinese, 5 percent Malay, 2.5 percent Indian, and 2.5 percent Eurasian, whereas that for the control group was 82.2 percent Chinese and 8.9 percent Indian. Eight participants did not indicate their ethnicity in the experimental (n = 4; 10 percent) and control (n = 4; 8.9 percent) groups.
Effects of the intervention on physical activity
Measurement of physical activity
For physical activity, the baseline was the mean number of steps per day for the first 2-week period, and was calculated for each of the 3 weeks of the intervention (Fig. 2).The post-test measure used in the subsequent analyses was an average of all the 3 weeks' data, and is indicated as physical activity–overall (PA-O). To provide a more detailed perspective, physical activity analyses based on the average of the final third week of the intervention have been provided, and are indicated as physical activity–final week (PA-F).
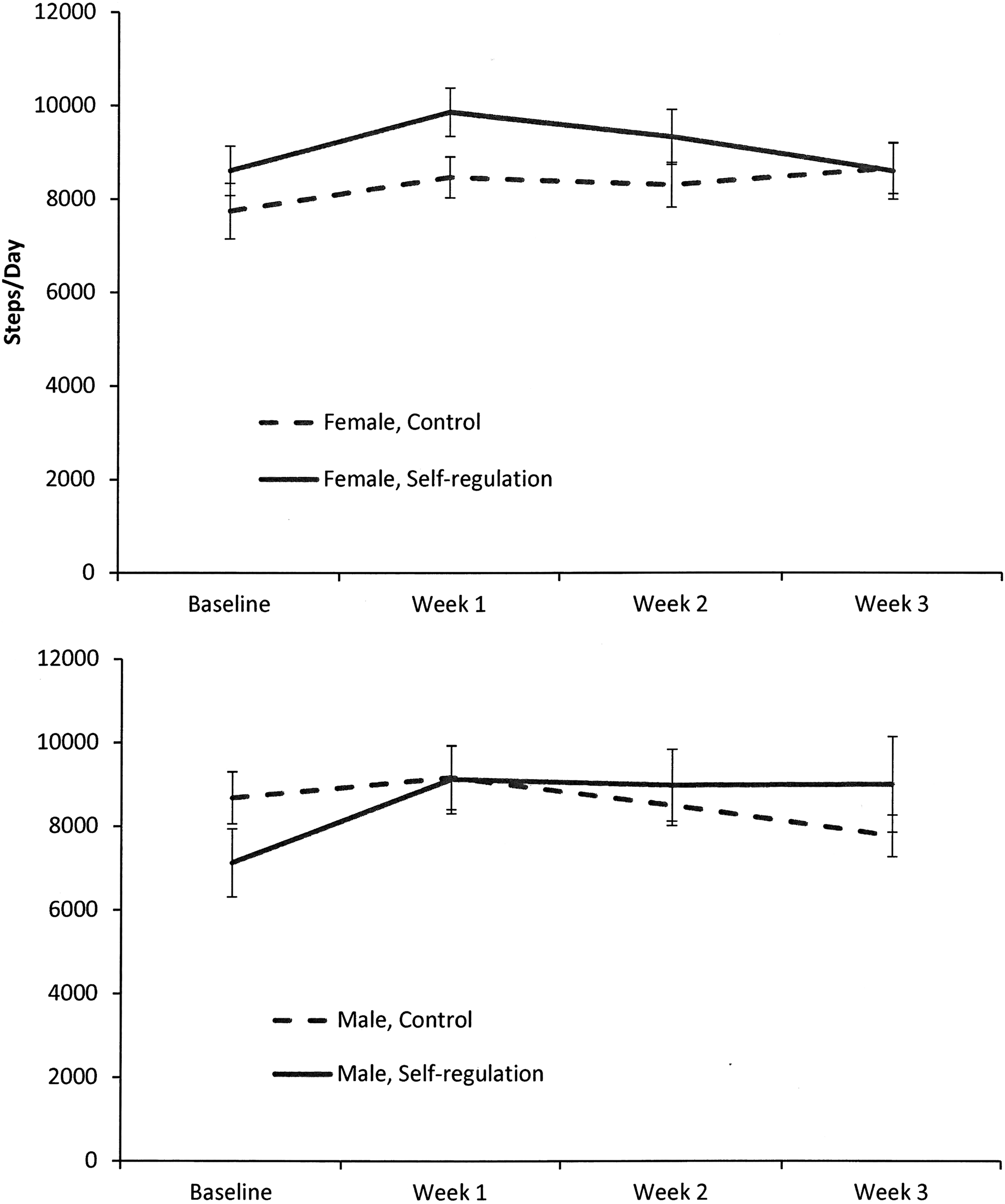
Steps per day for the experimental and control groups by gender at baseline and during 3 weeks of the intervention.
Repeated-measures ANOVA
For PA-O, the repeated-measures ANOVA indicated a main effect of time (p = 0.002), and a marginal time × group × gender interaction effect (p = 0.050). For PA-F, the repeated-measures ANOVA indicated a time × group × gender interaction (p = 0.004).
Two-way ANOVA and post hoc analyses
For PA-O, two-way (group × time) ANOVA indicated that for women, there was a main effect of time (p = 0.028); for men, there was a main effect of time (p = 0.025) and a time × group interaction effect (p = 0.015). Post hoc paired t tests indicated an increase in physical activity for the overall experimental group from M = 7,938.23 to 9,288.38 steps per day (p = 0.001), and the men of the experimental group indicated an increase in physical activity from M = 7,124.37 to 9,180.44 steps per day (p = 0.001; see Table 1), but no change for the control group.
P values in bold are <0.05.
BMI, body mass index; DA, anxiety symptoms; DD, depressive symptoms; DS, stress symptoms; PA-O, physical activity–overall; PA-F, physical activity–final week.
For PA-F, two-way (group × time) ANOVA indicated no significant effect for women, and a time × group interaction effect (p = 0.007) for men. Post hoc paired t tests indicated an increase in physical activity for men in the experimental group from M = 7,124.37 to 9,002.84 (p = 0.035), and a decrease for the men in the control group from M = 8,679.42 to 7,769.86 (p = 0.040; see Table 1).
Effects of intervention on well-being and mental health
For the well-being and mental health measures, there was a time × group interaction only for depressive symptoms (p = 0.048). Post hoc analyses indicated a decrease in depressive symptoms for women in the experimental group from M = 0.68 to 0.53 (p = 0.045), and an increase in depressive symptoms for men in the control group from M = 0.45 to 0.62 (p = 0.039). For life satisfaction, there was a time main effect (p = 0.019) and no time × group interaction; however, post hoc analyses indicated increases in life satisfaction for the overall experimental group from M = 4.53 to 4.76 (p = 0.014), and for the female experimental group indicated increases in life satisfaction from M = 4.67 to 4.98 (p = 0.024).
With regard to direct and indirect effects between the intervention and the dependent variables (change in the outcome variables), mediation analyses demonstrated there were no significant indirect effects. There was a marginally significant (p = 0.057) or significant direct effect (p = 0.047) on depressive symptoms based on whether the mediator was change in PA-O or PA-F, respectively.
Discussion
This study examined the effectiveness of self-regulation strategies for facilitating the achievement of a physical activity goal, and for increasing well-being and mental health. The intervention significantly increased the experimental group's physical activity. The increase was primarily due to the men in the experimental group, but there was a nonsignificant increasing trend for the women. Given the small sample size, the gender analyses should be interpreted with caution.
The intervention decreased the depressive symptoms of women but not of men in the experimental group; there was an increase in depressive symptoms of men in the control group. There was a suggestion that the intervention may have improved life satisfaction, especially for women. These gender differences are difficult to explain with the available data. Perhaps the explanation may lie within observed gender differences in how men and women respond to depression. As women are more likely to ruminate, and men are more likely to take action in response to depression, 25 we speculate that the active nature of this intervention may have had a greater impact on women because it activated a problem-solving response that countered their tendency to ruminate.
The results are consistent with previous research that demonstrated the benefits of self-regulation strategies such as MCII4,15,16 and self-monitoring 26 on achieving physical activity goals. A significant contribution of this study shows that the self-regulation strategies provided improvement beyond physical activity by decreasing female participants' depressive symptoms and improving participants' life satisfaction, especially for women. As Johannessen et al. speculated, one possible reason for a transfer effect is that there may be a motivational “spill over” from one life domain to another. 11
Mediation analyses suggested that the intervention had a significant or marginally significant direct effect on changes in depressive symptoms, which was not mediated through changes in physical activity. Although this intervention is not equivalent to therapy, the direct effect may be comparable with the effects of goal-oriented therapeutic strategies such as behavioral activation 27 and solution-focused brief therapy. 28
Limitations include the lack of a true experimental design, the use of two self-regulation strategies, the small sample size, and the suggestion of a regression to mean explaining the results. As two self-regulation strategies were used, it cannot be ascertained as to which one was more effective in influencing physical activity and well-being, and future research can help to examine the specific mechanisms in such interventions. Interaction and mediation effects involving gender need to be interpreted with caution due to the small sample size.
Other limitations include a marginally significant trend in the baseline depressive symptoms being higher in the experimental group than in the control group; regression to the mean may have contributed to the findings for depressive symptoms. There was a nonsignificant trend in the baseline physical activity being higher for the experimental women than the men. This trend may have contributed to the nonsignificant increase for the experimental women. Nevertheless, research has suggested a more positive attitude and higher intention to engage in leisure time physical activity for men rather than women. 29 Strengths of the study include the use of Fitbit data to assess physical activity, examining the impact of self-regulation strategies, and the assessment of mental health variables.
“Mens sana in corpore sano” is a Latin phrase that translates to “a healthy mind in a healthy body.” Although studies have linked self-regulation strategies to physical activity, as well as linked physical activity to well-being and mental health, one of the strengths of this study is suggesting that an intervention of self-regulation strategies may benefit both physical activity and mental health.
This finding is consistent with numerous fields of research highlighting the importance of self-regulation. In the research on goal pursuit, studies have shown how MCII benefited a range of outcomes, including physical activity and depressive symptoms.13,17 In studies based on Baumeister's strength model of self-regulation, researchers have illustrated how improving self-regulation in one life domain may improve self-regulation in other life domains.18,19 Research in positive psychology has shown the importance of self-discipline and grit,30,31 whereas research in behavioral addiction has shown that changes in self-regulation are related to changes in pathological video game use.32 From an applied perspective, health researchers may consider that a self-regulation intervention focusing on physical activity may actually have well-being and mental health benefits.
Footnotes
Acknowledgments
The research was funded by the National Institute of Education Academic Research Fund, RI 05/13 AL. A part of the study was based on Li Shan Goh's master's dissertation submitted to the National Institute of Education, Nanyang Technological University, Singapore. Albert Liau and Pony Chew were at Nanyang Technological University during the study. We gratefully acknowledge the support of Maria Plengsangtip, Jie Xin Lim, Xuanyi Wei, and Khin Maung Aye.
Author Disclosure Statement
No competing financial interests exist.
Appendix
In this appendix, the two self-regulation strategies used in the intervention are described in detail. For the first self-regulation strategy, participants were engaged in the mental contrasting with implementation intentions, which involved answering questions where they imagined their wish, outcome, obstacle, and plan in relation to physical activity. The detailed instructions were as follows:
“In this section, you will be asked to write down your answers to the following four questions in the given boxes, respectively. Please be noted that there are no right or wrong answers. Just write down what you truly think. Any of your information filled out below is strictly kept confidential according to our principles of research ethics.
The if-then plan has the following format: ‘If (here you refer to the obstacle you specified), then I will (here you name the behavior to overcome the obstacle).’ Now please complete the if-then plan below by writing down your thoughts in the blanks:
If…
then I will…
Now say this plan slowly in your head one more time.”
The purpose of the second self-regulation strategy was to facilitate self-monitoring. A daily e-mail was sent that reminded participants of the 10,000-step goal, and asked them to submit their pedometer data every day through Google document for the first 7 days of the intervention. At the end of the 7 days, participants were sent a graph of their daily number of steps for this period. The instructions in the e-mail were as follows:
“Dear Participant,
Thank you for your participation. We appreciate it a great deal. We would like to remind you that your daily goal of physical activity is 10,000 steps a day.
As mentioned during the 2nd session before, for the next 7 nights, please submit your step count for today into the Daily Log Sheet. Please click on the below link in order to enter your Daily Log Sheet:
[weblink provided]
Please complete your Log Sheet by midnight, 11.59 pm today. Otherwise, your pedometer will reset to zero at midnight.
Thank you very much for your time and participation!”