
Abstract
Abstract
The use of virtual reality (VR) in psychological treatment is expected to increase. Cybersickness (CS) is a negative side effect of VR exposure and is associated with treatment dropout. This study aimed to investigate the following: (a) if gender differences in CS can be replicated, (b) if differences in anxiety and CS symptoms between patients and controls can be replicated, and (c) whether the relationship between exposure to VR and CS symptoms is mediated by anxiety. A sample (N = 170) of participants with different levels of psychosis liability was exposed to VR environments. CS and anxiety were assessed with self-report measures before and after the VR experiment. This study replicated gender differences in CS symptoms, most of which were present before exposure to VR. It also replicated findings that a significant correlation between anxiety and CS can be found in healthy individuals, but not in patients. In a VR environment, anxiety partially mediated CS symptoms, specifically nausea and disorientation. A partial explanation for the differences found between patients and controls may lie in a ceiling effect for the symptoms of CS. A second explanation may be the partial overlap between CS symptoms and physiological anxiety responses. CS symptoms reported at baseline cannot be explained by exposure to VR, but are related to anxiety. Caution is required when interpreting studies on both CS and anxiety, until the specificity in measurements has been improved. Since anxiety mediated the CS symptoms, CS is expected to decline during treatment together with the reduction of anxiety.
Introduction
T
An important factor contributing to the effect of VR treatment is immersion, that is, the sense of being present in the virtual environment. 12 However, a common drawback of using head-mounted displays as a medium for immersive VR environments is the experience of cybersickness (CS), 13 also known as simulator sickness. CS is the occurrence of motion sickness-like symptoms when using VR and is related to increased treatment dropout. 1 As CS symptoms occur in 60 to 70 percent of participants, 14 this has a negative impact on treatment effects. CS is an unintended negative side effect and efforts should be made to limit negative effects while preserving the therapeutic effect of VR. 15
Four factors are reported to influence the occurrence of CS: (1) hardware and software choices for the VR system, (2) design of the virtual environment, (3) task characteristics, and (4) user characteristics.15,16 Examples of hardware and software characteristics influencing CS are visual surround of the display 17 and navigation (e.g., a mouse, joystick or treadmill). 18 The design of the virtual environment can influence CS by using dynamic auditory stimulation 19 and allowed movement (active vs. passive). 15 Task characteristics known to influence CS are duration of exposure to the virtual environment 20 and training. 21
User characteristics that can influence CS include gender, affective symptoms, and mental health. Susceptibility to CS is increased for women and varies over the menstrual cycle due to hormonal variation; however, explanations for this gender difference are incomplete. 22 Affective symptoms (e.g., feeling stressed or anxious) may increase the experience of CS23,24 but the nature of this relationship remains unclear.
VR treatment is used to expose patients to a virtual representation of their feared stimuli. During VR treatment patients will therefore experience high levels of anxiety. Physiological symptoms of anxiety and CS overlap and may confound both scientific research 24 and clinical practice. Anxiety disorders are much more prevalent in women, 25 making gender-specific relationships between CS, anxiety, and VR used in psychological treatment, an area of interest. It is also unclear why different findings emerge in healthy individuals and patients. For example, significant correlations between levels of experienced anxiety and CS were found in healthy controls, 26 but not in patients diagnosed with persecutory delusions exposed to a neutral VR environment. 27
High levels of CS symptoms were found in patients with an anxiety disorder even before immersion in VR. 28 Correlations were found between some CS symptoms and reported anxiety in a sample with both healthy controls and patients with an anxiety disorder. 29 Some CS symptoms may reflect anxiety more than side effects. 30 Thus, more clarity is required as to which user characteristics influence CS.
The present study aimed to investigate the following: (a) if gender differences in CS can be replicated, (b) if differences in anxiety and CS symptoms between patients and controls can be replicated, and (c) whether the relationship between exposure to VR and CS symptoms is mediated by anxiety (Fig. 1).
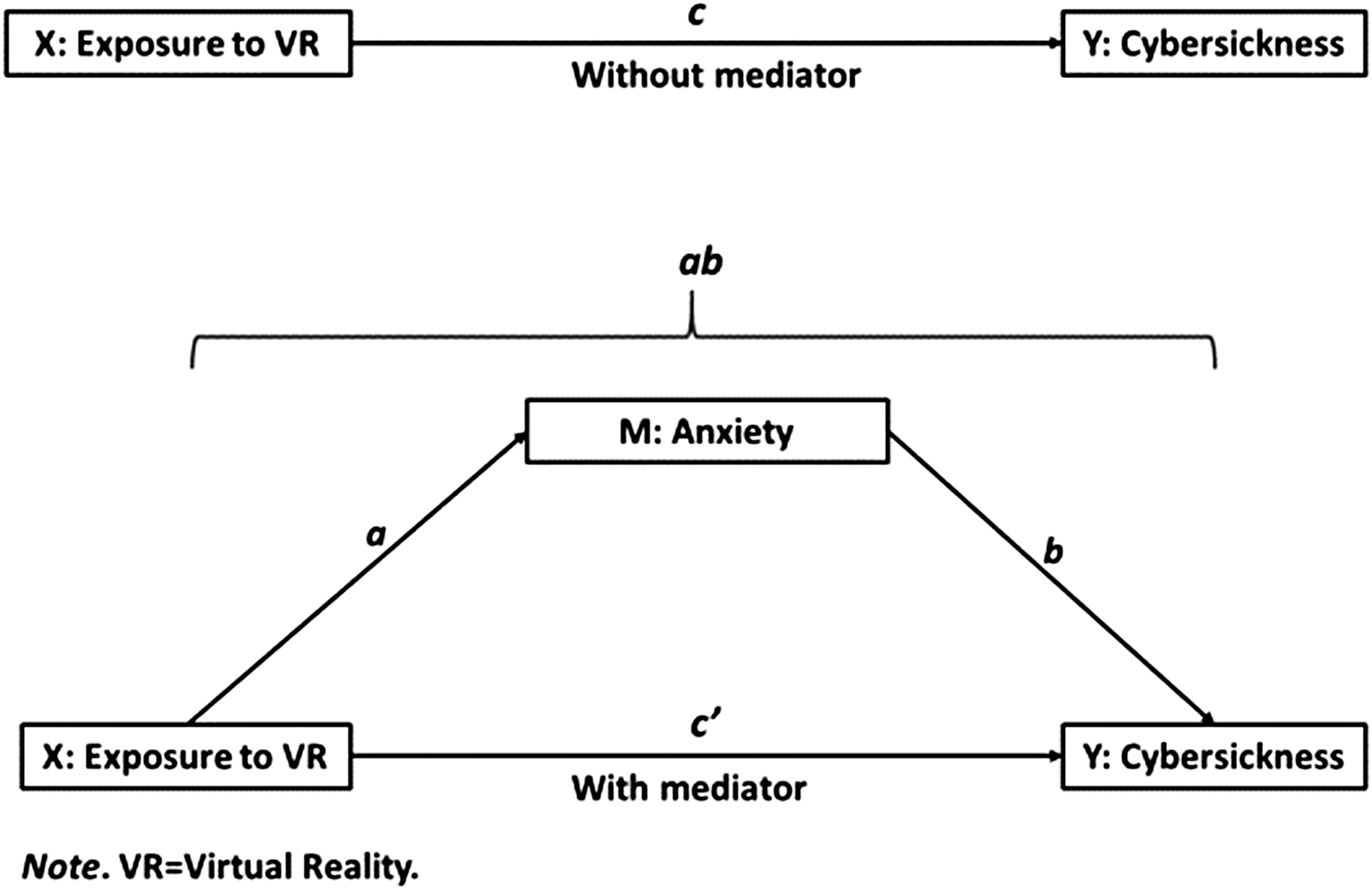
Hypothesis related to mediation. VR, virtual reality.
Materials and Methods
Participants
A total of 170 participants aged 18–35 years were earlier recruited for a large VR study. 31
From these, we defined a high liability patient group based on phenotype, that is, the experience of (subclinical) psychotic symptoms. This group consisted of two categories:
- Fifty-five patients with a psychotic disorder according to the DSM-IV, with the exception of substance-induced psychotic disorder, and psychotic disorder due to a medical condition. These patients were recruited at five outpatient departments. - Twenty patients with an at-risk mental state (ARMS), recruited among patients seeking help for nonpsychotic psychiatric problems at two outpatient departments.
The low psychosis liability control group consisted of:
- Forty-two siblings of people diagnosed with a psychotic disorder who had no personal history of a psychotic disorder themselves. - Fifty-three control persons recruited from the general population; they had no history of psychotic disorder nor a first-degree relative with a psychotic disorder.
Our previous study in this cohort found no difference in reported symptoms between the siblings and healthy controls, 31 allowing to combine both groups for the analysis.
The exclusion criteria were poor command of the Dutch language, epilepsy, and intelligence quotient (IQ) ≤75.
Ethical approval
This study was approved by the Medical Ethics Committee of the Leiden University Medical Center (NL37356.058.12/P12.182). Written informed consent was obtained from all participants.
VR setting
The virtual environment used in this experiment was a café. Participants could navigate the virtual environment using a Logitech F310 Gamepad. The Sony HMZ-T1 head-mounted display used for VR display of the café had a high-density resolution of 1280 × 720 (per eye), with 51.6 diagonal field of view, and built-in headphones. A 3DOF tracker (UM7 Orientation Sensor; CH-Robotics) was added to the Sony HMZ-T1 for head rotation. The researcher controlled the VR system and actions in the virtual environment using a graphical user interface.
Detailed information on the conditions is already published. 31 The social stressors used in this virtual social environment (population density, ethnic density, and hostility) were found to elicit feelings of anxiety. 31 All participants participated in five conditions, each with different levels of social stress. Exposure to each condition lasted 4 min. The order of the five conditions was randomized to prevent a sequence effect.
Measurement instruments
Diagnostic instruments
The Comprehensive Assessment of At-Risk Mental States 32 was used to assess ARMS before participation. Psychotic disorder was diagnosed with either the Comprehensive Assessment of Symptoms and History 33 or the Schedules for Clinical Assessment in Neuropsychiatry. 34
Anxiety was assessed by self-rated momentary subjective fear in units on an analog scale (subjective unit of distress [SUD]), ranging from 0 (no distress at all) to 100 (worst possible distress). Anxiety was first assessed before the experiments. Participants also rated their maximum anxiety during VR immediately after each of the five experiments. The mean of these five maximum anxiety scores was calculated and used for the analyses.
The self-report Simulator Sickness Questionnaire (SSQ) 35 was administered before and after the VR experiments. The SSQ measure's three distinct symptom clusters were labeled as Oculomotor (eyestrain, difficulty focusing, blurred vision, headache), Disorientation (dizziness, vertigo), and Nausea (nausea, stomach awareness, increased salivation, burping). The SSQ was scored according to the procedures by Kennedy et al. 35
Analyses
Analyses were conducted with IBM SPSS version 23. For sociodemographic characteristics, differences in continuous variables between the groups were analyzed using t tests. If the distribution of a continuous variable was skewed a Wilcoxon rank-sum test was used. Group differences in categorical variables were tested using χ2 analysis. Pearson's correlation coefficient (two-tailed) was used for correlations.
We used the MEMORE method 36 for two-condition within-participant statistical mediation analysis. The single test path-analytic approach by MEMORE eliminates the need for multiple discrete hypothesis tests about components of the mediation model, as the previous dominant approach 37 requires. A single test decreases the probability of an error occurring. The conditions were no exposure (baseline) and exposure to VR. MEMORE can be used to estimate the total (c), direct (c'), and indirect (ab) effects of exposure to VR on CS and its subscales through anxiety in a two-condition repeated measures design. Bootstrapping (5,000 samples) was used. Fixed covariates such as gender (or other stable individual differences) are accounted for in the MEMORE model.
Results
Demographics
A total of 170 participants were included: 95 controls in the low-liability group and 75 patients in the high-liability group. Sociodemographic characteristics of the participants as well as anxiety and CS scores are presented in Table 1. Controls had a higher level of education and a lower use of psychiatric medication. There was a trend of more female participants in the control group.
Note: Values are presented as mean (standard deviation) or n (%). CS was measured by the self-report SSQ. Anxiety was assessed by self-rated momentary subjective fear (SUD 0-100). Group differences between controls and patients of continuous variables were analyzed using a t test, or Wilcoxon's rank sum if skewed. Group differences of categorical variables were analyzed with χ2.
p < 0.05; **p < 0.01.
CS, cybersickness; SSQ, Simulator Sickness Questionnaire; SUD, subjective unit of distress; VR, virtual reality.
Gender
At baseline, 90 percent of women and 86 percent of men reported at least one symptom of CS. Women reported more CS symptoms than men, both overall and for each CS subscale. These differences were present both before and after exposure to VR.
No significant gender difference was found in the increase in total CS symptoms when exposed to VR (rank sum Z = 1.19; p = 0.24), or for oculomotor and disorientation separately. Women reported a stronger increase in nausea than men (rank sum Z = 2.31; p = 0.02) when exposed to VR. Results for both overall CS and for each of the three symptom categories separately are presented in Figure 2. No differences were found between men and women in reported anxiety, either before or during exposure to VR.
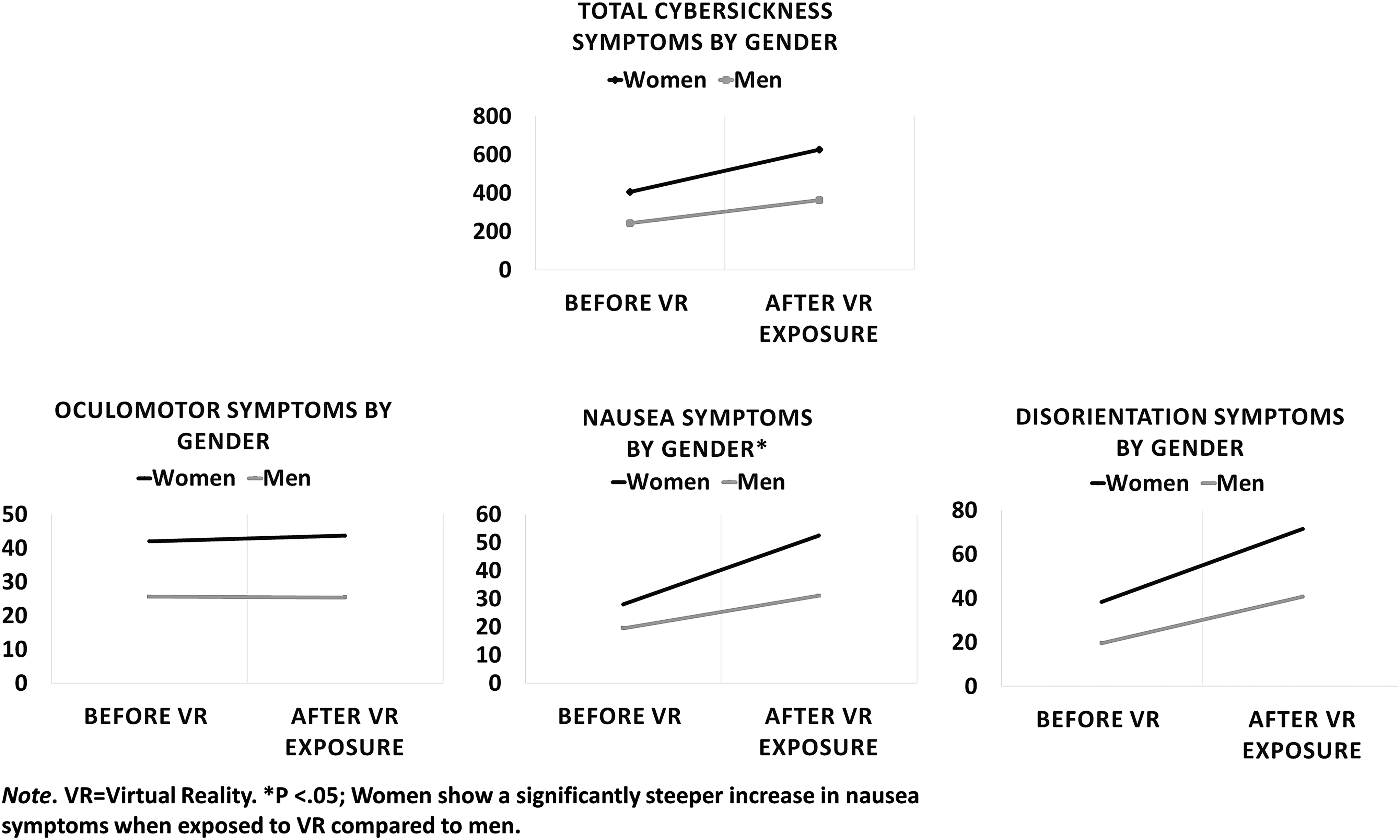
By gender, CS symptoms before and after exposure to VR. *p < 0.05; Women show a significantly steeper increase in nausea symptoms when exposed to VR compared with men. CS, cybersickness.
Patients and controls
At baseline, 81 percent of the controls and 96 percent of the patients reported at least one symptom of CS. Patients reported significantly more symptoms of CS at baseline than the controls. After exposure to VR, there was no significant difference in nausea and disorientation between the two groups. Results for both overall CS and for each of the three symptom categories separately are presented in Figure 3.
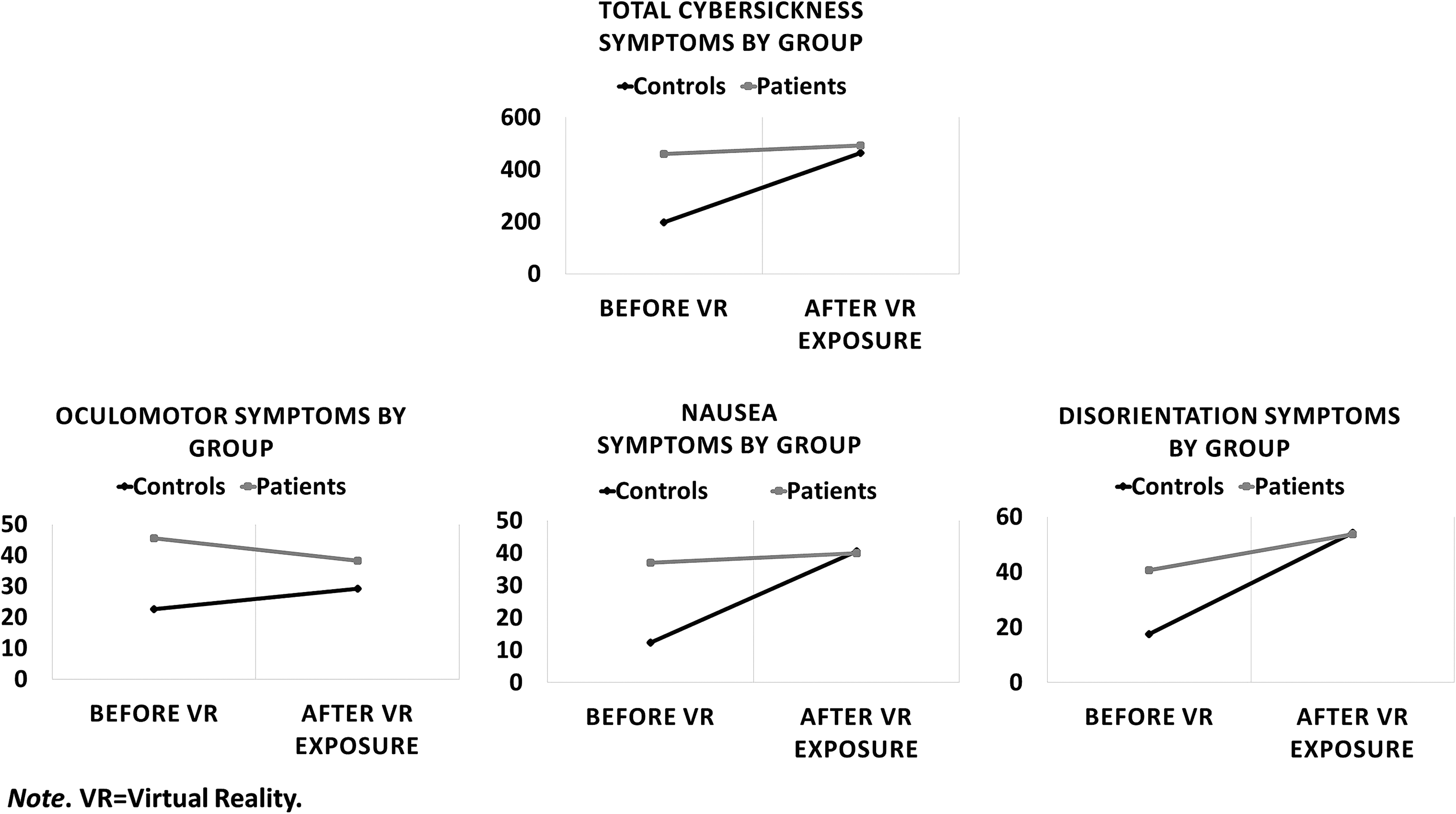
By group, CS symptoms before and after exposure to VR.
At baseline, there was a significant correlation between anxiety and CS for patients (r = 0.33, p < 0.01), whereas this was not found for the controls (r = −0.03, p = 0.74). In contrast, after exposure to VR, patients no longer showed a significant correlation between anxiety and CS (r = 0.19, p = 0.11), whereas the controls did (r = 0.53, p < 0.01).
Anxiety as mediator variable
For all 170 participants, a significant correlation was found between anxiety and CS at baseline (r = 0.33, p < 0.01) and after exposure to VR (r = 0.34, p < 0.01).
Mediation results are presented in Table 2.
Sobel test was used to estimate p value of indirect effects. CS was measured by the self-report SSQ. Anxiety was assessed by self-rated momentary subjective fear (SUD). MEMORE was used for two-condition within-participant statistical mediation analysis. The conditions were no exposure (baseline) and exposure to virtual reality. Fixed covariates, such as gender, are accounted for in the MEMORE model.
<0.05; ** <0.01.
SD, standard deviation.
Anxiety mediated the relationship between exposure to a VR environment and the experience of CS. The direct effect (c') remained significant, implying that the mediation effect of anxiety on CS was partial. Examination of the CS subscales revealed that the relationship between exposure to VR and nausea was partially mediated by anxiety. The relationship between exposure to VR and disorientation was also partially mediated by anxiety. Oculomotor symptoms had no direct relationship (c) with exposure to VR.
Discussion
In this VR study, the large majority of patients and controls reported at least one symptom of CS. We replicated both gender differences in CS and differences in CS between patients and controls. The relationship between exposure to VR and CS was partially mediated by anxiety. This implies that part of the relationship between exposure to VR and CS symptoms, more specifically nausea and disorientation, was explained by anxiety as an intermediary variable.
Women reported more CS symptoms than men, but most of these differences were already present at baseline. When exposed to VR, women had a steeper increase in nausea symptoms. The gender difference in severity of CS symptoms is in accordance with others. 22 However, gender differences in oculomotor and disorientation symptoms existed before VR exposure and cannot be explained by either exposure to VR or anxiety levels.
Our results replicate both findings about CS symptoms being present before exposure to VR in patients with an anxiety disorder, 28 and associations found between anxiety and CS symptoms.29,30 Our results replicate findings that significant correlations between anxiety and CS were found in controls 26 but not in patients.27,28 Our study indicates that a partial explanation may lie in a ceiling effect for CS symptoms, that is, CS symptoms were already high in patients before VR and remained high, whereas they were low in healthy controls before VR and increased during VR. A second explanation may be the partial overlap between CS symptoms and physiological anxiety responses.
CS symptoms reported at baseline cannot be explained by exposure to VR, but are related to anxiety. The present study found that anxiety was a mediating factor for nausea and disorientation symptoms of CS, but not oculomotor symptoms. This suggests that anxiety may impact some, but not all symptoms of CS. This is in line with studies showing five individual symptoms of CS (general discomfort, fatigue, headache, difficulty concentrating, and fullness of head) to correlate with reported anxiety.29,30 Especially two CS symptoms, general discomfort and difficulty concentrating, may reflect anxiety symptoms as they significantly load on the anxiety factor. 30 This is also in line with a study demonstrating that nausea symptoms are affected by reported anxiety. 24
We found no increase in oculomotor symptoms after exposure to VR; previous research on the profile of CS found that oculomotor symptoms are the least likely to occur, 38 which may have influenced the statistical power. It is also possible that oculomotor symptoms (e.g., eyestrain and blurred vision) are physiologically less related to anxiety symptoms. The fact that mediation by anxiety is partial and is consistent with the finding that multiple factors influence CS. 18
Strengths and limitations
The primary strength of the study is that the CS symptoms were measured before and after exposure to VR. Also, three different CS subscales were measured instead of only nausea, or using a single-sickness scale. Second strength is that the inclusion of both patients and controls allowed examining group differences. Thirdly, the MEMORE method simultaneously used the CS and anxiety scores before exposure to VR, as well as scores after exposure, to estimate mediation effects.
On the contrary, the statistical power of this study was limited, as many participants reported little CS and little or no anxiety symptoms; this impeded more detailed analysis of the subgroups. Four of the SSQ items load on two subscales instead of one, which inflate the contribution of these items on the total score. As two of these items, general discomfort and difficulty concentrating, are known to be correlated with anxiety, 30 this might have affected analysis.
Only two specific patient groups were included and all participants were relatively young; both these factors limit the generalizability of our findings. Also, this study examined state anxiety only, whereas additional affect states should be explored in future research. As a stable individual difference trait, anxiety is accounted for in the MEMORE model. However, as it can influence both the anxiety response and the CS symptoms, more research is required to clarify its potential role. Another limitation is that anxiety was measured with self-report. Finally, this study used the diagnostic criteria of the DSM-IV instead of the current DSM-V; however, as there are only marginal differences in the categories of psychotic disorders 39 the effect on the individual diagnosis of each patient in the present study can be considered negligible.
Clinical implications and future directions
This study indicates that caution is required when interpreting studies on both CS and anxiety, until the specificity in measurements has been improved. Gender differences in CS should also be taken into account. Findings on CS based on controls cannot be generalized to patients. Reported anxiety symptoms may partially reflect CS symptoms and vice versa. The relationship between VR exposure and CS symptoms is partially explained by anxiety as an intermediary variable. When VR therapy reduces anxiety, the nausea and disorientation symptoms are expected to decline. In addition, CS symptoms decrease after repetitive use of VR. 40 If a patient reports anxiety and CS during the first stages of VR treatment and can tolerate this, we recommend to continue with VR treatment.
Future research should include patients diagnosed with an anxiety disorder, and measure both state and trait anxiety. Replication with a larger sample size of a broad age range is necessary to be able to perform more detailed analysis of subgroups and further clarify mechanisms.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Declaration of Helsinki 1975, as revised in 2008.
Footnotes
Acknowledgments
This work was supported by the Netherlands Organization for Health Research and Development (Veni 916.12.013 to W.V.).
Author Disclosure Statement
No competing financial interests exist.