
Abstract
Abstract
A mobile virtual reality system, equipped with built-in variables such as heart rate (HR), gaze-down data, and subjective fear rating, can allow individuals with a fear of heights to overcome it by self-training. This study aimed to verify the efficacy and safety of the training program. Forty-eight volunteers completed the four-session self-training program over 2 weeks. They were allocated into either low- or high-fear group by the Acrophobia Questionnaire (AQ)-anxiety scores, and then the changes of the built-in variables and AQ-anxiety scores were analyzed between the groups. The safety was assessed using the Simulator Sickness Questionnaire (SSQ). The AQ-anxiety scores were significantly decreased after self-training in both groups, and the degree of decrease was significantly greater in the high-fear group than in the low-fear group. Gaze-down percentage and subjective fear rating showed a significant group difference, but HR did not. The SSQ scores were within the acceptable level. These results suggest that the training effect was greater in the high-fear group than in the low-fear group. This mobile program may be safely applicable to self-training for individuals with high scores on the fear of heights by repeated exposure to virtual environments with the embedded feedback system.
Introduction
F
Virtual reality (VR) is one of the technologies enabling individuals to train something by themselves. The most typical training using VR is exposure therapy, which is a technique in behavior therapy used to reduce anxiety by the inhibitory learning process. 4 Three types of procedures, such as in vivo or real life, imaginal, and interoceptive, can be applied for exposure therapy. 5 VR technology is used when in vivo exposure is not practical. VR allows repeated exposures to multiple “real-like” contexts without space restriction, and provides a chance to treat a phobia in a safe, confidential, and cost-effective way.6,7 Due to these advantages, VR exposure therapy has been employed in treating phobias, including social phobia,8,9 agoraphobia, 10 arachnophobia, 11 and fear of flying.6,12,13 This therapy has also been demonstrated to be effective in overcoming the fear of heights.14–17 In the VR exposure therapy, immersion and presence provided by VR play an important role in the improvement of symptoms. 18
Treatments using VR have been available in a setting under the therapist's control so far; however, the development of a self-training VR program will be useful for individuals who tend to avoid visiting hospitals. In addition, this self-training program will also be helpful to clinicians that can use it as a therapeutic homework in their treatment sessions. The recent increase in the availability of mobile VR equipment and drastic decline of the cost provide a favorable environment for this self-training tool. With the pressing need for easily accessible options, we have developed a mobile-based VR self-training program that would allow individuals to virtually experience the heights in realistic and filmed scenes. For self-training, this program reaps the benefits of VR, allowing immediate performance recordings and supplying physiological feedback.19,20
Built-in variables of performance in our program include heart rate (HR) and gaze-down percentage, which are automatically measured while participants experience the virtual heights. HR is used as a parameter of the arousal level, whereas gaze-down percentage is counted to assess how well individuals look down from a high place despite the threat of heights. Exposure in the treatment of acrophobia leads to synchronous changes in psychophysiological arousal and subjective anxiety. 21 HR change has been confirmed in various VR environments, such as a social situation 22 and tunnel driving. 23 The virtual display of elevation has also induced physiological arousal comparable to that found in a real environment.24,25 Self-tracking or biofeedback of HR has acute effects on self-reported stress, 26 and provides an efficient way to reduce autonomic physiological reactions in response to negative stimuli. 27 It has been demonstrated that a set of brain regions, including the ventrolateral prefrontal cortex, pregenual anterior cingulate cortex, and insula supports volitional control of HR. 28 In addition, our built-in variables include subjective fear ratings, which are designed for individuals themselves to assess in the VR screen immediately after experiencing a scene for measuring how fearful it is. Recognizing one's own behavioral or emotional condition in VR treatment is useful for improving a self-regulatory ability in an anxious situation. 29 To apply to self-training for overcoming the fear of heights, contents of our program included four missions for allowing gradual exposures of the heights to participants, and also featured built-in behavioral and physiological variables that provided feedbacks on their level of fear and performance.
The current study aimed to verify the efficacy and safety of our mobile program on volunteers. We expected that subjective and physiological indicators reflecting fear reactions could be elicited through built-in variables and would be changed across repeated exposures, and that the more fear participants feel, the more effective outcome they would obtain after self-training. Based on these expectations, we examined the changes of built-in variables such as HR, gaze-down percentage, and subjective fear ratings during training, the level of acrophobia before and after training, and the severity of motion sickness after experiencing the virtual environments, and compared them between the low- and high-fear groups. The hypotheses of this study were that individuals with high fear would show greater changes in the built-in variables and level of acrophobia than individuals with low fear, and that the severity of motion sickness would be a level within a tolerable range.
Methods
Participants
Participants were recruited through a notice in a university's community Web site. From 71 applicants, we selected 50 individuals who had (a) no epilepsy and other neurological diseases, (b) no history of psychiatric illnesses and substance dependence, and (c) no cardiac or vestibular problem. Since 2 participants were dropped out of the training due to personal reasons, a total of 48 participants completed the training. This study followed ethical standards and was approved by the Institutional Review Board of Yonsei University Gangnam Severance Hospital.
Virtual task setting
Figure 1A shows the VR equipment. The virtual environment was displayed through the head-mounted display (HMD) latching a mobile phone (Galaxy S6 and Gear VR; Samsung Electronics). This system provided a 360° panoramic view with 96° field of view and allowed tracking of head movement as participants tilted their head to look around the environment. In-ear earphones were connected to the phone. Samsung Gear S2 smartwatch, worn on the wrist, was used to measure HR. Instructions were presented as text on the screen or by voice through the audio system.
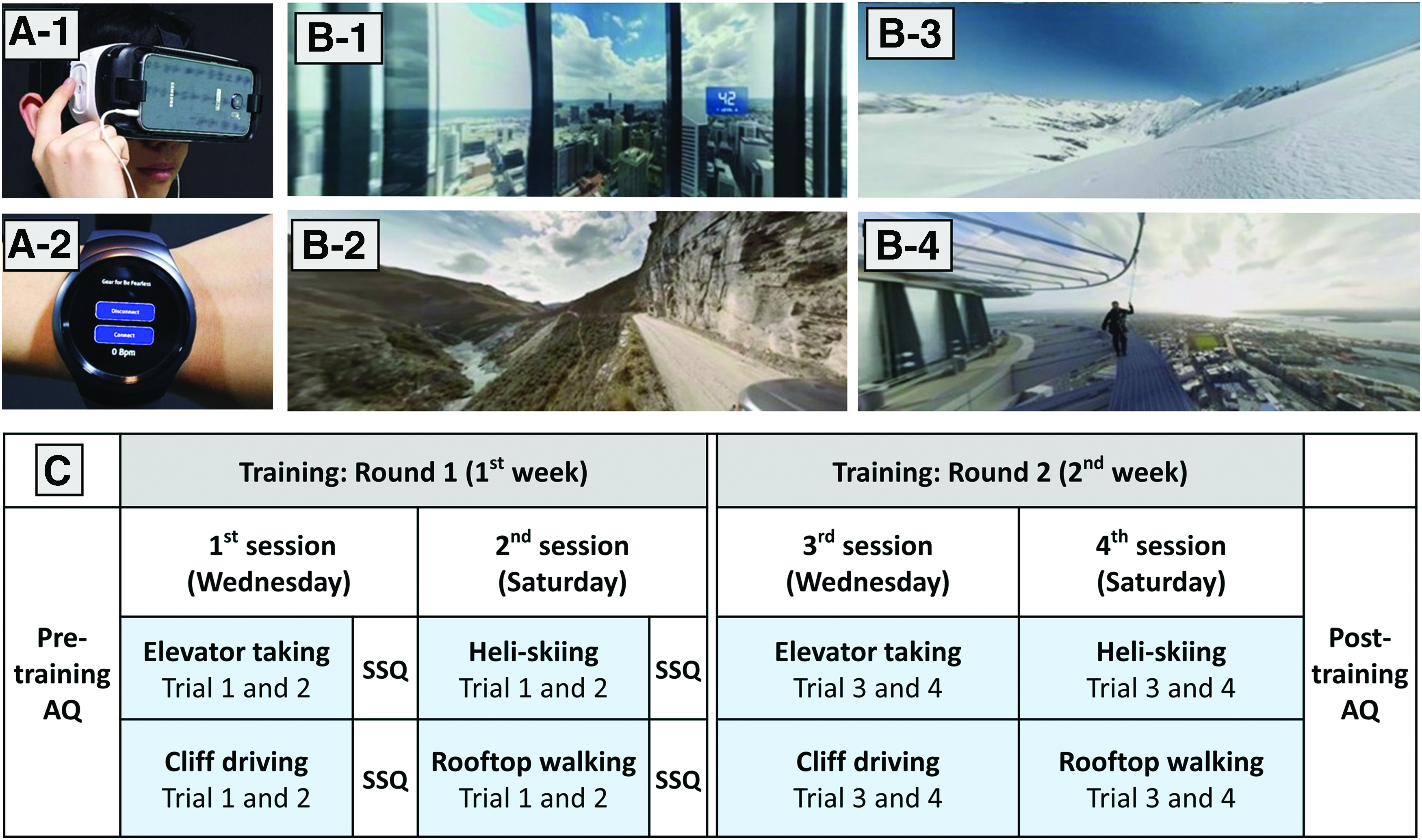
The devices and missions for the mobile virtual height task. The devices consisted of head gear with a touch pad, a smart phone latched onto the head gear
The task offered four different missions (Fig. 1B). For elevator taking, participants were placed in a glass elevator ascending from the 1st floor to the 45th floor with the background noise of the elevator operating. Cliff driving was to look outside in the back seat of a car running a road over a steep cliff. Heli-skiing was to look down from a helicopter flying over snow-covered mountains and then to jump and ski down a mountain slope at high speed. For rooftop walking, participants should take a stroll around the outer perimeter, encircling the top of a tall tower. When the mission system was developed, a task validation was preliminarily performed by measuring the level of scene-induced fear in five volunteers with mild height fears (five females, 27.0 ± 5.1 years of age), who rated on the subjective scale ranged from 0 (no fear) to 4 (extreme fear). The average scale scores 0.8 ± 0.8 in elevator taking, 2.2 ± 0.8 in cliff driving, 1.2 ± 1.1 in helicopter flying, and 3.4 ± 0.5 in rooftop walking.
Each mission lasted 5 minutes. To measure the baseline values, each mission started in a neutral situation for 10 seconds and then moved onto the height challenge. Built-in measures were made up of three different variables; (a) mean HR for 10 seconds during the neutral situation (baseline HR) and for early 10 seconds, middle 10 seconds, and late 10 seconds of each mission (challenge HR); (b) gaze-down percentage, the ratio spent watching under 10° from the horizontal line for the entire duration of each mission; and (c) subjective fear ratings, which were assessed in the VR screen immediately after the end of each mission using the touchpad and ranged from 0 (no fear) to 2 (severe fear). Participants could review each of the variables on the performance evaluation page. All data were instantly uploaded and made available on a cloud-based Web site.
Training procedure
All participants took part in four training sessions (Fig. 1C) over 2 weeks in the VR center. They were in a room alone with an assistant and were seated in a revolving chair. The assistant simply provided help to them in the operation of the VR devices. Participants executed the task by themselves based on to the built-in instructions. At each training session, they completed two missions. Each mission was repeatedly experienced for two times per session. Therefore, all four missions were experienced during the first week (“Round 1”). The same procedure was repeated during the second week (“Round 2”). Upon completing one mission and answering the built-in subjective question, they were instructed to see the performance report and go through each built-in variable.
Measurements of performance and safety
We used a Korean translation of the two self-report scales to measure performance and safety. Before the first session and after the final session, participants completed the anxiety subscale of the Acrophobia Questionnaire (AQ), 30 which included 20 items about fear of heights and a 7-point Likert scale using 0 (not at all anxious) to 6 (extremely anxious; possible score range 0–120; Cronbach's α 0.80). To assess the safety, participants repeatedly reported the severity of motion sickness after completing each mission on the first week of training using the Simulator Sickness Questionnaire (SSQ), 31 which consisted of 16 items with 4-point scales using 0 (none) to 3 (severe). This questionnaire yielded three subscores, such as nausea, oculomotor, and disorientation, which were calculated by the sum of each item associated with each subscore and multiplication of the special coefficient (9.54, 7.58, and 13.92, respectively) to the sum. The adjusted total score was obtained from the sum of the three subscores and multiplication of the special coefficient (3.74) to the sum.22,31
Statistical analyses
For the built-in variables, average scores from the repeated experiences in each session were used, and whole-period HR (the mean of baseline HR and challenge HR) and HR change {100 × [(challenge − baseline)/baseline]} were used as an additional variable. Before the analysis, normal distribution of outcome variables was inspected with Shapiro–Wilk tests. To find out the difference in the training effect, we divided the participants into two groups based on the pretraining AQ-anxiety scores. As the AQ-anxiety scores did not deviate from normality assumption (Shapiro–Wilk normality test, p = 0.041), median split (AQ-anxiety score = 41) was used for grouping them. In addition, based on the cutoff point of 45.45 on the AQ-anxiety score for high height fear in the previous report, 32 the number of individuals with high height fear before and after training was counted.
Since all built-in variables did not violate the normality, they were analyzed using repeated-measures analysis of variance (ANOVA), considering the time effect (baseline vs. challenge or Round 1 vs. Round 2) and group effect. Training and group effects of the AQ-anxiety scores were also analyzed using repeated-measures ANOVA. Post hoc examinations were performed using paired t tests. The SSQ scores were analyzed only for the group comparison using the Mann–Whitney U test because of the significant violation of the normality assumptions. To find associations among the built-in variables and SSQ scores, we calculated Pearson's correlations between mean values of whole-period HR, subjective fear rating, gaze-down percentage, and SSQ scores during all four missions.
Results
Demography
The pretraining AQ-anxiety scores were significantly different between the low- and high-fear groups (t = −12.21, p < 0.001). However, the two groups did not significantly differ in age, sex ratio, and education (Table 1).
AQ, Acrophobia Questionnaire—anxiety; SD, standard deviation.
Built-in variables during training
The comparisons between baseline HR and challenge HR and between groups in each round are presented in Table 2. In Round 1, the time effect in rooftop walking was the only significant result [F(1, 46) = 9.43, p = 0.004]. Significant results in Round 2 were the time effects in cliff driving [F(1, 44) = 6.25, p = 0.016], heli-skiing [F(1, 46) = 14.61, p < 0.001], and rooftop walking [F(1, 46) = 9.11, p = 0.004]. Table 3 presents the comparisons between rounds and between groups. Significant results for whole-period HR were the round effects in elevator taking [F(1, 44) = 5.44, p = 0.024], cliff driving [F(1, 44) = 19.52, p < 0.001], and heli-skiing [F(1, 46) = 4.59, p = 0.037]. There was the round effect of the HR change from baseline to challenge in heli-skiing [F(1, 46) = 5.17, p = 0.028] and the group effect in elevator taking [F(1, 44) = 4.52, p = 0.039]. Gaze-down yielded the group effect in heli-skiing [F(1, 46) = 4.94, p = 0.031] and rooftop walking [F(1, 46) = 11.94, p = 0.001].
Data: mean and SD.
Round 1, two sessions for first-week training; Round 2, two sessions for second-week training; Baseline, the mean of HRs during 10 seconds of the neutral situation; Challenge, the mean of HRs during 30 seconds of the height experience.
p < 0.05 (two-tailed); **p < 0.01 (two-tailed).
ANOVA, analysis of variance; HRs, heart rates.
Data: mean and SD.
Round 1, two sessions for first-week training; Round 2, two sessions for second-week training; Baseline, the mean of HRs during 10 seconds of the neutral situation; Challenge, the mean of HRs during 30 seconds of the height experience
p < 0.05 (two-tailed); **p < 0.01 (two-tailed).
In subjective fear ratings, elevator taking showed the group effect [F(1, 46) = 7.24, p = 0.010] and round × group interaction [F(1, 46) = 7.43, p = 0.009]. Cliff driving showed the round effect [F(1, 46) = 19.85, p < 0.001] and group effect [F(1, 46) = 18.76, p < 0.001], as well as round × group interaction [F(1, 46) = 5.45, p = 0.024]. In post hoc analysis, only the high-fear group showed significant decreases in both elevator taking (t = 2.70, p = 0.013) and cliff driving (t = 4.29, p < 0.001). In heli-skiing, the only significant result was the group effect [F(1, 46) = 12.02, p < 0.001]. In rooftop walking, there were the round effect [F(1, 46) = 30.78, p < 0.001] and group effect [F(1, 46) = 52.54, p < 0.001], as well as round × group interaction [F(1, 46) = 5.96, p = 0.019]. In post hoc test, both the low- and high-fear groups showed significant decrease (t = 3.08, p = 0.005; t = 4.63, p < 0.001, respectively).
Height fear before and after training
The mean AQ-anxiety scores before and after training were 22.71 and 17.29 in the low-fear group, and 63.71 and 48.04 in the high-fear group. There were the training effect [F(1, 46) = 46.96, p < 0.001], group effect [F(1, 46) = 98.50, p < 0.001], and training × group interaction [F(1, 46) = 11.10, p = 0.002]. As shown in Figure 2, post hoc t tests revealed that although the low- and high-fear groups showed significant decreases after training (t = 2.78, p = 0.011; t = 6.58, p < 0.001, respectively), the degree of decrease was significantly greater in the high-fear group than in the low-fear group (t = 3.33, p = 0.002). In addition, the number of individuals with the high AQ-anxiety score above 45.45 was 26 before training and was reduced to 13 after training.

Changes of the AQ scores in the low- and high-fear groups. Standard errors are represented as error bars. *p < 0.05 (two-tailed); **p < 0.01 (two-tailed).
Severity of motion sickness
Table 4 shows results of the three subscores and adjusted total scores of the SSQ. In the low-fear group, the adjusted total score was the lowest in elevator taking (median = 2.00, Q1 = 0.00, Q3 = 18.00) and the highest in rooftop walking (median = 7.00, Q1 = 0.00, Q3 = 26.00). In the high-fear group, it was the lowest in cliff driving (median = 43.00, Q1 = 31.00, Q3 = 101.00) and the highest in rooftop walking (median = 80.50, Q1 = 49.75, Q3 = 131.00). In all environments, the high-fear group showed significantly higher subscores and adjusted total score than the low-fear group (all: p ≤ 0.001).
Correlations
Table 5 shows correlations among mean values of the built-in variables and SSQ scores in each round for all participants. Correlation of subjective fear rating with whole-period HR was insignificant during Round 1, but significant during Round 2 (r = 0.42, p = 0.004). Correlation of subjective fear rating with gaze-down percentage was significant during Round 1 (r = −0.33, p = 0.023), but insignificant during Round 2. Correlation between whole-period HR and gaze-down percentage was also significant during Round 1 (r = 0.39, p = 0.007), but insignificant during Round 2. In correlations of the SSQ score with subjective fear rating and gaze-down percentage, significant results were seen in both Round 1 (r = 0.71, p < 0.001; r = −0.30, p = 0.037, respectively) and Round 2 (r = 0.43, p = 0.002; r = −0.29, p = 0.047, respectively). We additionally conducted correlation between whole-mission SSQ scores and AQ-anxiety change to explore the possible factors hindering the treatment efficacy. Among the four SSQ scores, the oculomotor score was negatively correlated with AQ-anxiety change (r = −0.31, p = 0.033).
p < 0.05 (two-tailed); **p < 0.01 (two-tailed).
SSQ, simulator sickness questionnaire.
Discussion
In the present study, the AQ-anxiety scores decreased after self-training in both the low- and high-fear groups, suggesting that our program may be effective in reducing scores on the fear of heights in most people. As expected, the reduction was significantly greater in the high-fear group than in the low-fear group. The AQ-anxiety scores before and after self-training were 63.71 and 48.04 in the high-fear group. This result is comparable with a previous study of the VR exposure therapy on patients suffering from acrophobia, 16 where the AQ-anxiety scores before and after the therapy were 57.12 and 36.12. The effect of self-training in the high-fear group was also gauged in the built-in subjective fear rating, which was significantly lower in the second round than in the first round.
Both groups showed increases of HR during challenge compared with baseline due to the fear of heights in most missions. Contrary to our expectation, however, there was no group difference in the HR change. This is consistent with a recent report that both patients with acrophobia and normal controls experienced a significant increase in HR and skin conductance during a virtual height challenge. 33 The concordant results of the two studies indicate that there may be discordance between subjective fear and physiological arousal. This discordance was confirmed by the round effect in the present study. During the second round, compared with the first round, whole-period HR was increased in most missions despite decreased subjective fear rating. Nonetheless, HR still reflects a fear response in that the subjective fear rating was positively correlated with whole-period HR in the second round, although not in the first round.
Meanwhile, the high-fear group showed significantly greater subjective fear ratings in all missions than the low-fear group, suggesting that subjective fear can be effectively measured while performing the task. The gaze-down percentage was correlated negatively with the subjective fear rating and positively with whole-period HR, particularly in the first round. The high-fear group showed significantly less gaze-down percentage than the low-fear group, particularly in heli-skiing and rooftop walking. This is consistent with the recent finding that individuals with acrophobia exhibited restricted visual exploration and freezing gaze to the horizon. 34 Therefore, the gaze-down percentage seems to be opposite to a built-in variable because it effectively reflects an avoiding behavior. However, it was not proved to be an index of improvement of avoidance by training because there was no round effect in all missions.
In the evaluation of safety, simulator sickness was minimal in the low-fear group, but considerable in the high-fear group. The mean SSQ total scores in the high-fear group ranged from 43 to 80.05, and were similar to or higher than those of visually induced motion sickness in previous reports.35,36 The closed-type HMD is favorable to immersion, but results in increasing simulator sickness. 37 The group difference in the severity of simulator sickness was found in all SSQ subscores and all missions. The association of fear and simulator sickness was also confirmed in correlation analysis, which revealed a significant correlation of the SSQ scores with the subjective fear rating and gaze-down percentage. These are consistent with the previous report that simulator sickness is related to subjective judgment and eye gaze. 36 In our data, subjective fear and SSQ score were the largest during rooftop walking among the missions, further suggesting the close association between the two variables. This association may stem from the similarity of symptoms between fear response and simulator sickness. That is, some autonomic disturbances such as headache, sweating, nausea, and dizziness are induced by the simulator, but they are also the physical symptoms of anxiety.
The very low dropout rate of our sample suggests that simulator sickness was tolerable. Considering the frequency, however, individuals with a high fear of heights should be especially careful of simulator sickness. The VR users are recommended to rightly sit on a chair and briefly use the application with an interval of several days. 38 Although our study was performed following these recommendations, the oculomotor score was negatively correlated with the AQ-anxiety change, suggesting that eye strain can hinder the treatment efficacy. It has been demonstrated that simulator sickness can hinder perceived presence and consequently, impede the treatment efficiency. 39 Our program can be helped with an aid to mitigate simulator sickness, if it becomes available. Recently, several methods for alleviating simulator sickness, such as galvanic cutaneous stimulation 35 and the use of pleasant odors, 40 have been proposed.
The present study has some limitations. As most participants were in the mid-20s, the study did not account for age variation. Someone with very high AQ-anxiety scores could be a patient with acrophobia, but the exact diagnosis was not made. Because our groups were based on the AQ-anxiety scores rather than clinical diagnosis, the effectiveness in the high-fear group does not necessarily mean treatment outcome in the patients. It is also uncertain whether or not the effectiveness of the training can be generalized to real life because pre- and posttraining behavioral tests were not conducted to evaluate how well the fear of heights was overcome in real situations. Since the sense of presence or immersion was not evaluated, it was difficult to quantify how much participants felt the VR missions to be enough to immerse. Although acrophobic responses are different between standing and walking, 34 we gained the data only in the standing condition. In addition, a measure for safety was only the self-reporting SSQ and other objective measures were not applied in the study. Finally, although our mobile program was designed for self-training, data were obtained in a VR center to reliably monitor participants' performance. Further study is necessary to confirm whether the same results can be obtained by self-training at home.
In conclusion, the efficacy of our program was identified by the decrease of the AQ-anxiety scores after self-training in both the low- and high-fear groups. The superior effect of self-training in the high-fear group was proved by the greater decrease of the AQ-anxiety scores compared with the low-fear group. HR and gaze-down percentage were demonstrated to be a built-in variable as an index of arousal and an avoiding behavior, respectively. Simulator sickness induced by the program was tolerable to participants. This mobile program may be useful to self-training for individuals with high scores on the fear of heights by repeated exposure to virtual heights and feedback information.
Footnotes
Acknowledgments
This work was funded by Samsung Electronics Co. Ltd. Dr. J.-J.K. was contracted by Samsung Electronics Co. Ltd., to develop the program and collect participant data. The funding source provided the concept, and technical and visual support in developing the VR mobile application. However, it had no role in the conduct of the study; collection, management, analysis, interpretation of the data, as well as in the preparation, review, and decision to submit the article for publication.
Author Disclosure Statement
No competing financial interests exist.