
Abstract
Abstract
With this article, we aim to increase our understanding of how mobile virtual reality exposure therapy (VRET) can help reduce speaking anxiety. Using the results of a longitudinal study, we examined the effect of a new VRET strategy (Public Speech Trainer, PST), that incorporates 360° live recorded VR environments, on the reduction of public speaking anxiety. The PST was developed as a 360° smartphone application for a VR head-mounted device that participants could use at home. Realistic anxiety experiences were created by means of live 360° video recordings of a lecture hall containing three training sessions based on graded exposure framework; empty classroom (a) and with a small (b) and large audience (c). Thirty-five students participated in all sessions using PST. Anxiety levels were measured before and after each session over a period of 4 weeks. As expected, speaking anxiety significantly decreased after the completion of all PST sessions, and the decrement was the strongest in participants with initially high speaking anxiety baseline levels. Results also revealed that participants with moderate and high speaking anxiety baseline level differ in the anxiety state pattern over time. Conclusively and in line with habituation theory, the results supported the notion that VRET is more effective when aimed at reducing high-state anxiety levels. Further implications for future research and improvement of current VRET strategies are discussed.
Introduction
P
Effects of VRET on public speaking anxiety
VRET is based on graded exposure framework where individuals are exposed to increasing level of frightening stimuli. 9 This allows them to become habituated to the feared situation, leading to decrement of anxious responses to dysfunctional thoughts and events.22,23 VRET treats successfully public speaking anxiety comparably to a traditional Cognitive Behavioral Therapy (CBT) and often with lower dropout rates.8–11,20 Interestingly, VRET leads to a higher decrement in public speaking anxiety in highly anxious participants compared with less anxious ones based on the principles of psychodynamic behavioral therapy where commonly patients with severe anxiety symptoms benefit the most from (graded) exposure compared with moderate (healthy) and control groups.24,25 Besides, the state anxiety was much higher after completion of VRET in highly anxious participants compared with less anxious ones. 26 This may be due to hypersensitivity among high-anxious people, which increases awareness of environment stimuli that form a potential threat.27,28 Previous findings also imply that phobic speakers show more anxiety when speaking to an (usually animated) audience, then when speaking within an empty room, while less or nonphobic speakers do not show different anxiety responses. 16 Hence, we speculate that changes in state anxiety over time and across different VR exposure conditions will show a different pattern for participants with high and moderate initial anxiety levels. More research is needed regarding the fluctuation of state anxiety over time during a VRET.
Realness of virtual audience in VRET for public speaking anxiety
To make exposures to frightful stimuli realistic, VRET incorporates highly immersive three-dimensional environments generated through a multisensory pc, console, or mobile phone, which can be experienced through a wide field of view head-mounted display (HMD). These VR technologies can make exposure experiences feel real. Previous research showed that anxiety symptoms experienced during VRET matched the actual symptoms of speaking anxiety. 29 As a consequence, patients often prefer VRET over live in vivo exposure therapy. 20 A popular technique to increase realism is the integration of real-world video footage in VR environments by means of 360° videos. 30 This technique is widely adopted and rising since 2015, 31 as it is often cheaper than the creation of animations. Incorporating live video footage within VRET may improve a realistic experience as animated avatars are usually not perceived as realistic. 5 In addition it can increase the accessibility of VRET, as many smartphones support 360° video. 5 Nevertheless, only one study 8 demonstrated reduction of public speaking anxiety due to a VRET that integrated a real live audience video, yet, as a part of a regular (non-mobile) treatment setting.
The current study
Participants followed three mobile phone PST sessions based on CBT-graded exposure principles,7,32 by means of virtual presence in an empty hall (session 1), in front of a small audience (session 2), and large audience (session 3). Participants used the PST in their home environment, their own presentation material and their private smartphones.10,16,17 Within the aforementioned framework, we investigated the following hypotheses:
In addition, we explored changes in state anxiety over time and across different PST sessions to identify differences in anxiety change patterns for participants with a high and moderate initial anxiety level.
Methods
Research design and procedures
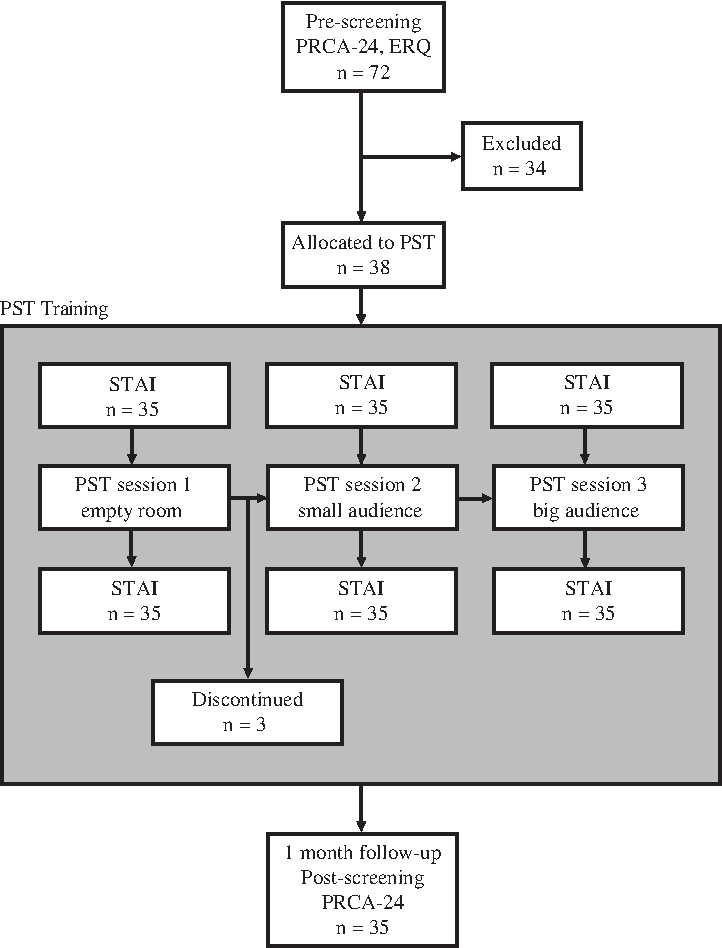
We used a longitudinal quasi-experimental design (Fig. 1). After prescreening (assessing public speaking anxiety and emotion regulation), an e-mail with protocol and consent form was sent to participants with a high to moderate public speaking anxiety level. A moderate or high anxiety level state meant a score 55 or higher on a scale from 1 to 120 (Personal Report of Communication Apprehension scale [PRCA-24] 33 ). All participants were given a pre-experimental task to adjust to habituate to the VR environment and prevent motion sickness. 34 It was highlighted that exposure therapy is most effective when a patient is at rest. 35 The participants who passed the task received a briefing and demonstration of the PST application as well as a VR HMD, so they could start using the PST at home. Participants received notifications via e-mail or WhatsApp about when they could start another video session or had missed a training session. Per PST session, a State Anxiety Inventory (STAI)-based pretest and posttest of S-anxiety was conducted. A month later participants filled in the PRCA-24 postscreening survey.
Participants and sampling
Seventy-two students from Dutch and International Universities in the Netherlands with moderate to high initial public speaking anxiety scores were recruited via posters, flyers, Facebook, lectures, and University newsletters. All of them completed the prescreening that consisted of the PRCA and the Emotion Regulation Questionnaire (ERQ). Seven participants were excluded due to low initial public speaking anxiety levels. Twenty-seven participants refused to participate in the training after they received the protocol and consent form. Primary reason, according to the participants, was a lack of time due to school or work. Three participants dropped out after the first session because of the same reason. As such, 35 participants, 25 females and 10 males, between 19 and 25 years old completed the training (Fig. 1). We looked if the dropout had biased the data; Little's Missing Completely At Random (MCAR 36 ) test showed that the data may be assumed to be MCAR test, χ2 = 46,316, df = 36, p = ns, and therefore missingness is assumed not to matter for the further analysis. 37
Material: PST
The PST (Figs. 2–5) was specifically designed for this experiment and developed for smartphones. Participants downloaded the application in the Google Play Store (android) or in Testflight (iOS). A 360° video was recorded using six GoPro cameras in a 360° rig (settings: 2.7K, 4:3, 30 fps) and stitched together in Autopano Video Pro. Recording took place in a lecture hall with roughly 100 students and 2 teachers and lasted 5 minutes. Audience size was manipulated using video software Adobe After Effects and creating three audience size based on training levels: (a) no audience, (b) small audience (12 people), and (c) big audience (Figs. 3–5). The videos could be replayed, paused, or stopped. To prevent participants from watching all sessions in a different sequence, training levels would unlock one by one after each week. The average amount of practice for video 1 was three times (M = 3.03, standard deviation [SD] = 1.04), for video 2 was four times (M = 4.00, SD = 0.87), and for video 3 was three times (M = 3.43, SD = 1.10).

Interface of the PST application.

Empty room.

Small audience.

Big audience.
Measures
Speaking anxiety was assessed using PRCA-2433. The PRCA-24 consists of 24 anxiety items divided across four subscales: group discussion (6 items; “I dislike participating in group discussions”), meetings (6 items; “Generally I am nervous when I have to participate in a meeting”), interpersonal conversations (6 items; “While participating in a conversation with a new acquaintance, I feel very nervous”), and public speaking (6 items; “I have no fear of giving a speech”). A 5-point Likert-type scale was used (1 = strongly disagree to 5 = strongly agree). As such, sum scores per subscale can range from 6 to 30. A sum score above 18 indicates a degree of speaking anxiety, scores between 55 and 83 indicate a moderate speaking anxiety level, and scores between 83 and 120 indicate a high level of speaking anxiety. 33 Internal consistency was satisfactory in both, pre- and postassessment (0.81 < α < 0.92).
Anxiety state was measured using the S-Anxiety scale from the STAI 38 . This scale includes 20 items on a Likert-type scale (1 = not at all to 4 = very much so). An example of an item is: “I feel calm.” The range of total scores is 20–80, where a cutoff point of 39–40 is suggested to detect clinically symptoms for state anxiety. 38 Internal consistency was satisfactory during all six assessment moments (α-range: 0.89–0.93).
As emotion regulation can influence communication and stress levels, 39 it might be a relevant confounder. We measured emotion regulation during prescreening using the ERQ, 40 which includes 10 items on a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree) divided across two subscales, reappraisal (6 items; “When I want to feel more positive emotion such as joy or amusement, I change what I'm thinking about”) and suppression (4 items; “I keep my emotions to myself”). Internal consistency was satisfactory (reappraisal, α = 0.78; suppression, α = 0.76) and Principal Component Analysis (PCA) revealed a two-factor structure.
Results
Baseline characteristics of participants
Participants differed in baseline speaking anxiety total scores, t(35) = 10.347, p < 0.001, with 71.4 percent of the participants scoring moderate and 28.6 percent scoring high on this scale. Participants with initially high speaking anxiety scored higher on speaking anxiety total score and all speaking anxiety subscales (Table 1). Participants did not differ on baseline anxiety state measured before the first PST session [t(35) = 1.724, p = ns]. Within the moderate and high level of speaking anxiety subsamples, participants did not differ on baseline anxiety state, t(35) = −1.247, p = ns (Table 2). Regarding the emotion regulation strategies, the reappraisal baseline score was higher, t(35) = 6.400, p < 0.001, while the suppression baseline score was lower than the population average score, t(35) = −2.955, p < 0.01. At the moderate–high speaking anxiety subsample level, no differences in reappraisal t(35) = −0.064, p = ns, and suppression t(35) = −0.732, p = ns between the two subsamples were found.
Sum-scores with different subscripts are significantly different (t test).
p < 0.01; ***p < 0.001.
PRCA-24, the Personal Report of Communication Apprehension scale. 33
State anxiety measurement moments are chronologically presented with 1 = before training session 1, 2 = after session 1, 3 = before session 2, 4 = after session 2, 5 = before session 3, and 6 = after session 3. Sum-scores with different subscripts are significantly different (t test).
p < 0.01.
Speaking anxiety differences before and after the PST
Confirming H1, paired sample t tests revealed that participants scored lower on speaking anxiety total score after the PST was completed, t(35) = 3.216, p < 0.01 (Table 1 and Fig. 6). Anxiety during the context of public speaking, t(35) = 4.811, p < 0.001, and the context of interpersonal conversation, t(35) = 2.511, p < 0.05 contributed to this difference. No differences were found between pre-and posttest in other speaking anxiety subscales, anxiety during group discussions t(35) = 0.467, p = ns, and during meetings, t(35) = 0.529, p = ns.
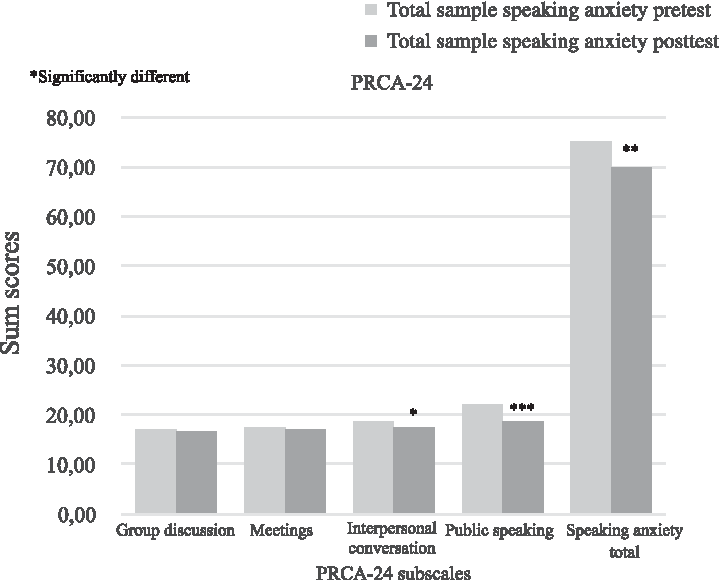
Differences in speaking anxiety scores before and after the PST. Pretest and posttest PRCA-24. *p < 0.05; **p < 0.01; ***p < 0.001.
The PST is more effective in participants with a high level of public speaking anxiety, confirming H2 (Table 1 and Fig. 7). For high speaking anxiety participants, the total speaking anxiety score, t(10) = 4.785, p < 0.01, as well those on three out of the four subscales scored lower after the PST was completed [for public speaking, t(10) = 6.708, p < 0.001, interpersonal conversation, t(10) = 4.000, p < 0.01, and group discussions t(10) = 2.653, p < 0.05] but not for subscale “during meetings” [t(10) = 1.843, p = ns]. For moderate speaking anxiety participants, only the subscale public speaking showed a decrement over time, t(25) = 3.129, p < 0.01.
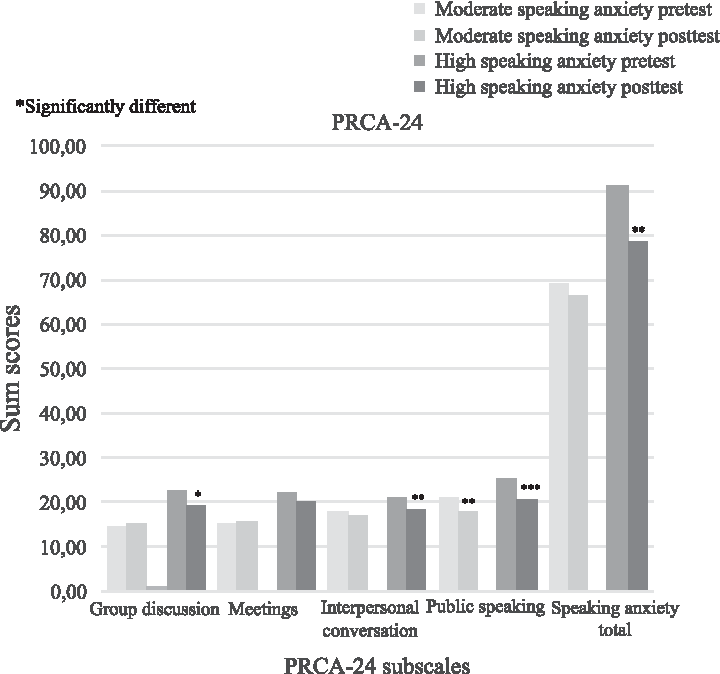
Differences in speaking anxiety scores before and after the PST in initially moderately and highly anxious participants. Pretest and posttest PRCA-24. *p < 0.05; **p < 0.01; ***p < 0.001.
State anxiety difference over time
A repeated measures analysis of covariance, with the high versus moderate speaking anxiety baseline variable as a covariate, showed a small effect of the PST sessions on state anxiety over time, F(5, 165) = 2.902, p < 0.05, ηp2 = 0.08. Contrasts revealed that compared with the state after first session, state anxiety increased after the first training, F(1, 33) = 8.300, p < 0.01, ηp2 = 0.20 and before the second training, F(1, 33) = 9.556, p < 0.01, ηp2 = 0.23, but decreased after the second training session, F(1, 33) = 7.518, p < 0.05, ηp2 = 0.19. However, state anxiety increased before the third session compared with after the second session, F(1, 33) = 5.167, p < 0.05, ηp2 = 0.23. No difference was found on state anxiety before and after the third training session (Fig. 8).
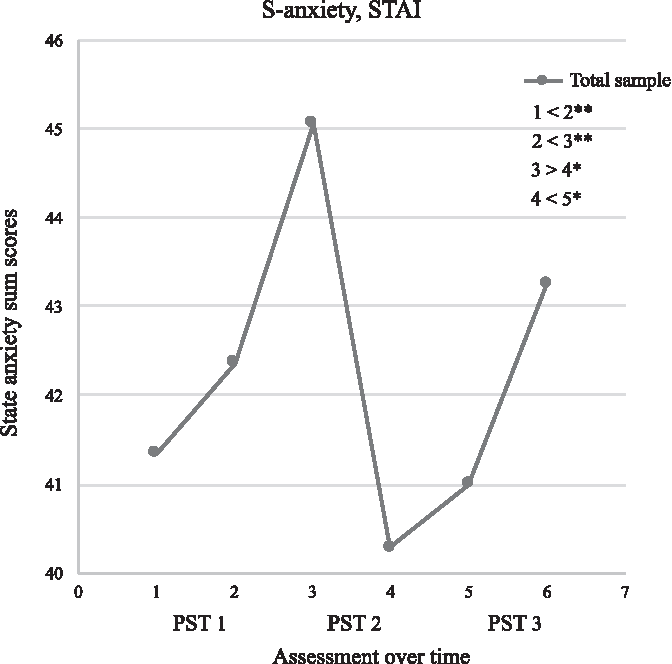
Fluctuation of state anxiety scores over time (before, during and after the PST). PST 1, Training session 1; PST 2, Training session 2; PST 3, Training session 3. *p < 0.05; **p < 0.01.
Results revealed an interaction effect of speaking anxiety on state anxiety, F(5, 165) = 2.820, p < 0.05, ηp2 = 0.08. Contrasts revealed interactions when comparing participants with moderate and high speaking anxiety on state anxiety before and after the first training session, F(1, 33) = 11.253, p < 0.01, ηp2 = 0.25, after the first and before the second session, F(1, 33) = 7.430, p < 0.05, ηp2 = 0.18, and after the second and before the third session, F(1, 33) = 4.868, p < 0.05, ηp2 = 0.13. State anxiety shows different patterns for participants with moderate and high speaking anxiety (Fig. 9). While state anxiety significantly increases after the first training in high speaking anxiety group, it decreases in the moderate speaking anxiety group. State anxiety decreases between the second and third training session in high speaking anxiety group, while it increases for the moderate speaking anxiety group. Also, a different pattern is revealed for state anxiety after the second and before the third session (a decrement for the high speaking and an increment for the moderate speaking anxiety group). Table 2 shows an overview of state anxiety (sub)scales sum-scores.
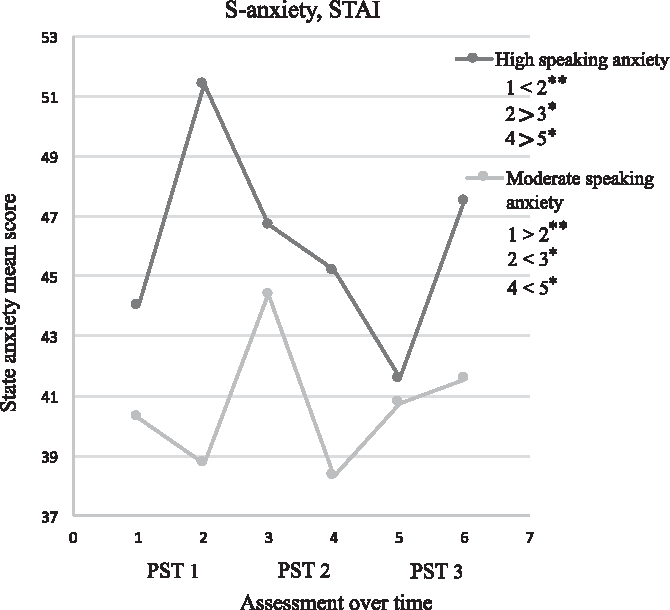
Differences between initially moderate and high anxious participants in state anxiety scores over time (before, during and after the PST). PST 1, Training session 1; PST 2, Training session 2; PST 3, Training session 3. *p < 0.05; **p < 0.01.
Discussion
We investigated the efficacy of the PST in students with high and moderate level of public speaking anxiety in the Netherlands. As expected, we found that public speaking anxiety decreases after the completion of the PST in participants with initially moderate and high level of public speaking anxiety.8–11,20 Our findings also confirmed that a PST is more effective for individuals with an initially high level of speaking anxiety compared with those with moderate anxiety.16,24,25,27,28
This study further contributes to the belief that state anxiety shows different patterns over time and across anxiety situations in participants with different initial speaking anxiety levels. For the low anxiety level simulations (e.g., an empty room) moderately anxious participants show an opposite pattern compared with anxious participants (revealing a decrement instead of an increase in state anxiety). This is not surprising due to their hypersensitivity to external stimuli.1,11,28 Healthier individuals show a typical habituation process followed by a decrement of anxiety in the same session, as they do not appraise the situation as being threatening.22,23 An alternative explanation is related to the concept of presence, feelings of “being there” related to the degree to which a medium can produce realistic representations of objects, events, and people. 41 One could argue that only highly anxious individuals perceive VR environments as being real enough as they also perceive a real situation very quickly as threatening even if the threat is nonrealistic. 42 However, previous research showed that high level of presence can be induced with a low level of representativeness of VR avatars. 16 This finding combined with the fact that we used live videos of real audiences makes us believe that the different patterns found to relate to environment sensitivity levels and not a difference in feelings of presence. Moreover, there is some evidence that intensity of (speaking) anxiety is not directly affected by the presence in VR. 26
We also discovered that after each PST session, only highly anxious participants always felt immediately less anxious, while for moderately anxious sample anxiety sometimes increased. We can only speculate that highly anxious individuals are much more relieved after being exposed to public speech situations as they normally are extremely aware of stimuli in VR environments during the sessions that could form a potential threat. 42 Stepping out of the threatening situation will automatically lead to decrement in the state anxiety. Nevertheless, the habituation also eventually occurred in moderately anxious individuals as the increment in state anxiety before each of PST sessions gradually decreased over time.
The current study has several limitations. The sample consisted of healthy (nondiagnosed) students. Applying the PST in patient population would probably increase its efficacy as the VRET used in our study was more effective for participants with an initial high level of public speaking anxiety. In addition, we need to be careful with the interpretation of the current results due to a small sample size as the generalizability to a broader population is low. Anxiety was assessed by self-reports and there was no control group included. To obtain more objective anxiety measurements during the therapy, future research should include biofeedback applications. Finally, VRET future studies could focus on how to make use of VR to motivate participants to reduce dropout rates. Higher motivation is achieved by including features in the VR environment such as rewards, personal presentation slides, speech/voice recognition, and positive and interactive feedback (e.g., relaxation when anxiety level is too high). Moreover, it is highly recommended to ask the research participants to give a speech in a real situation before and after the public speech training to ensure the efficacy of the training.
We conclude that the PST is effective in reduction of public speaking anxiety in students, although further research is needed to establish whether this type of mobile VRET can replace a VRET that is commonly guided by a therapist. Moreover, our data revealed differences in PST effects for high and moderate anxious individuals making an argument to adjust future PST devices based on those findings.
Footnotes
Acknowledgments
The authors are grateful for the patience and support of Oscar Bastiaens and Creative Lab (NHTV) experts in 360 videos, Dr. ir. Willem-Paul Brinkman (Technical University of Delft) for valuable advice at the start of this research, and Arnoud Versluis (NHTV) for helping us with sampling. A special thanks to Erwin Peters, a student from the International Game Architecture and Design at the NHTV, who codeveloped the virtual PST application. On a personal note, we acknowledge the support from Juul Ketelaars, Danae Arroyos Calveras, Barbara Meijkamp, Anneriek van Laarhoven, and Jeffrey van Herwijnen.
Author Disclosure Statement
No competing financial interests exist.