
Abstract
Abstract
Problematic video game use (PVGU), or addiction-like use of video games, is associated with physical and mental health problems and problems in social and occupational functioning. Possible correlates of PVGU include frequency of play, cigarette smoking, and attention deficit hyperactivity disorder (ADHD). The aim of the current study was to explore simultaneously the relationships among these variables as well as test whether two separate measures of PVGU measure the same construct, using a structural modeling approach. Secondary data analysis was conducted on 2,801 video game users (Mage = 22.43 years, standard deviation [SD]age = 4.7; 93 percent male) who completed an online survey. The full model fit the data well: χ2 (2) = 2.017, p > 0.05; root mean square error of approximation (RMSEA) = 0.002 (90% CI [0.000–0.038]); comparative fit index (CFI) = 1.000; standardized root mean square residual (SRMR) = 0.004; and all standardized residuals <|0.1|. All freely estimated paths were statistically significant. ADHD symptomatology, smoking behavior, and hours of video game use explained 41.8 percent of variance in PVGU. Tracking these variables may be useful for PVGU prevention and assessment. Young's Internet Addiction Scale, adapted for video game use, and the Problem Videogame Playing Scale both loaded strongly onto a PVGU factor, suggesting that they measure the same construct, that studies using either measure may be compared to each other, and that both measures may be used as a screener of PVGU.
Introduction
T
Addiction has traditionally been studied with respect to substance use, but uncontrollable video game use that yields significant negative consequences may also be considered a form of addiction. While video game addiction is not a formal diagnosis in the Diagnostic and Statistical Manual of Mental Disorders–5th edition (DSM-5), Internet Gaming Disorder is listed under the section “Conditions for Further Study,” encouraging research in this area. 8 Studies show that the biological mechanisms for behavioral addictions such as Gambling Disorder and Internet Gaming Disorder are similar to the biological mechanisms of substance addictions. 9 Addiction-like video game use is characterized by an overall reward deficiency and, similar to substance dependence, cue-induced craving is present. In addition, research suggests that problematic video game use (PVGU) is associated with a number of negative consequences such as general health and mental problems, and difficulties in school, work, and interpersonal relationships.6,10–12
There is some variability in how video game addiction is defined and measured. Some studies use diagnostic criteria for pathological gambling from the DSM–4th edition (DSM-IV), adapted for video game use.6,13–16 Others study PVGU, which is a more general term that may refer to a large number of hours of video game use per day, 10 or to high scores on questionnaires designed to measure addiction-like use of video games.11,15,17 More recently, but subsequent to data collection for the current study, a measure based on DSM-5 criteria for Internet Gaming Disorder was developed. 18 Because the discussion on video game addiction is still in progress, this article will mainly use the term PVGU to refer to addiction-like or problematic use of video games.
Due to the problems associated with problematic play, it is important to identify correlates of PVGU, such as the amount of video game and tobacco use. Individuals who play video games most often tend to play the longest sessions, the majority of those who play over 4 hours per session tend to play video games daily, 19 and the number of days spent playing video games in the last 30 days is positively associated with PVGU. 15 Similarly, individuals with PVGU tend to spend more time on video games compared with individuals without PVGU. 14 Tobacco use is also correlated with PVGU.11,15,17,20 Desai et al. 20 found that among adolescents, when adjusting for race and gender, the odds of reporting PVGU were 112 percent greater for video game players who reported smoking regularly compared with video game players who reported never having smoked (p < 0.007). In addition, Van Rooij et al. 11 found that boys who used cigarettes were twice as likely to score high on PVGU.
Attention deficit hyperactivity disorder (ADHD) may also be linked to developing PVGU. Most studies of the relationship between ADHD symptoms and PVGU have been conducted in children, and show that ADHD symptoms are predictors of increased video game use,21,22 and more severe symptoms are associated with PVGU.16,23 Children with ADHD have significantly higher PVGU scores than those without ADHD, 24 and children with ADHD are less likely to stop playing video games on their own and when asked by their parents to stop. 24 The few studies on ADHD and PVGU among adults also show that ADHD symptoms are associated with problematic play. Adults with video game addiction report more severe ADHD symptoms than matched controls without video game addiction. 12 Also, while ADHD symptoms in general are correlated with PVGU, inattention symptoms may be more strongly related to problematic play. 25 ADHD may also influence PVGU indirectly through its relationship with smoking. Adolescents and young adults with ADHD have a significantly greater chance of smoking compared with those without ADHD. 26 A recent meta-analysis showed that smokers with a childhood history of ADHD begin to smoke regularly earlier than smokers without a childhood history of ADHD. 27 Matthies et al. 28 found that adults with ADHD started smoking earlier compared with individuals without ADHD, and Laucht et al. 29 found that adolescents with ADHD have higher smoking rates than adolescents without ADHD.
Identifying the relationships among correlates of PVGU is critical for the development of appropriate treatment plans specific to PVGU, as well as to help assess risk and develop targeted prevention programs. Currently, studies on PVGU are few in number and the variability in defining and measuring PVGU makes it difficult to compare the results of existing studies and to make prevention and treatment recommendations, even though problematic play is associated with negative life consequences.30–32 Current treatment recommendations for PVGU, such as cognitive-behavioral therapy 33 and family therapy, 34 are therefore based on limited information, and actual treatment studies are few in number.33,35 Research to date suggests that ADHD, nicotine use, and number of hours spent on video games are all independently associated with video game addiction. However, no study has examined all of these variables simultaneously. Investigating such relationships may enhance understanding of the mechanisms, by which these potential risk factors may lead to video game addiction, and thus inform treatment recommendations. Therefore, the aim of the current study is to explore relationships among these potential correlates of video game addiction. In addition, limitations in the current literature regarding variability in the measurement of PVGU will be addressed by including and assessing two commonly used measures for PVGU, using structural equation modeling (SEM).
Materials and Methods
Participants
Participants included 2,801 video game users who responded to online advertisements on multigenre video game forums for an online survey. All individuals were adults between the ages of 18 and 57 (M = 22.43, standard deviation [SD] = 4.70; 93 percent male). See Table 1 for additional demographic information.
GED, General Education Diploma.
Materials
Problematic video game use
Young's Internet Addiction Scale (YIAS) 36 is a 20-item scale that assesses Internet addiction among adults. It adapts DSM-IV criteria for pathological gambling to Internet addiction. All items are rated on a six-point Likert scale (0 = not at all to 5 = always). Total summed scores range between 0 and 100, with scores between 0 and 30 indicating a normal level of Internet use, 31 and 49 indicating a mild level of Internet addition, 50 and 79 indicating a moderate level of Internet addiction, and 80 and 100 indicating a severe level of Internet addiction. For this study, all uses of the word “Internet” were replaced with “video game(s)” to adapt the questionnaire for measuring video game addiction. Example items include, “How often do you prefer the excitement of video games to intimacy with your partner?” and “How often does your job performance or productivity suffer because of playing video games?” This scale demonstrates good reliability 21 (α = 0.89 in the current study).
The Problem Videogame Playing (PVP) 37 Scale is a nine-item scale that assesses symptoms of video game addiction. It is based on DSM-IV criteria for substance dependence and pathological gambling. The items are dichotomous, with yes or no answers; higher total scores indicate higher levels of PVGU. Example items include, “I spend an increasing amount of time playing video games” and “When I lose in a game or I have not obtained the desired results, I need to play again to achieve my target.” For this study, an eight-item version of the original scale was used. One item was excluded from the scale due to user error (“Because of the video game playing I have reduced my homework, or schoolwork, or I have not eaten, or I have gone to bed late, or I spent less time with my friends and family.”), and no data were collected for this item. Reliability for the PVP typically ranges from poor to adequate, but the scale demonstrates good construct validity. 37 Cronbach's alpha for the current study was 0.53.
ADHD symptomatology
Conners' Adult ADHD Rating Scale-Self-Report: Short (CAARS-S:S) 38 is a 26-item scale that assesses adult ADHD symptomatology. Example items include, “It's hard for me to stay in one place very long” and “I intrude on others' activities.” Items are rated on a four-point Likert scale (0 = not at all to 3 = very much, very frequently) and summed to form a total score. A score greater than 65 reflects a clinically significant level of ADHD symptomatology. 39 The internal consistency and test–retest reliability of the CAARS-S:S range from good to excellent, and the scale demonstrates good convergent validity.40,41 The Cronbach's alpha for the current study was 0.89.
Smoking behavior and video game use
Participants reported the average number of cigarettes and the average number of hours they spent playing video games per week.
Procedure
This study was approved by Internal Review Board of Loma Linda University. Participants completed an online survey hosted by Qualtrics. Participants were recruited via advertisements posted on multigenre web forums such as
Statistical analysis
A partially latent SEM was used to test the relationships among ADHD, nicotine use, number of hours spent on video games, and PVGU. In the structural component of the model, ADHD, nicotine use, and number of hours spent on video games were tested as predictors of PVGU. In the measurement component of the model, PVGU was a latent variable, defined by the YIAS and the PVP scale. The YIAS, which has higher reliability than the PVGU, was used to set the metric.
The analysis was conducted using EQS Version 6.1 with full information maximum likelihood (FIML) estimation. Instead of the traditional approach to handling missing data in SEM, which involves deleting all cases with any missing information, FIML uses all available data, even if some data for a case are missing. 42 Model fit was assessed using model chi-square (χ2), root mean square error of approximation (RMSEA), comparative fit index (CFI), and standardized root mean square residual (SRMR). Good fit is indicated by a nonsignificant χ2, RMSEA <0.05 with the upper limit of the 90 percent CI <0.1, CFI >0.9, SRMR <0.1, and absolute values of standardized residuals <0.1. 43
Results
Table 2 shows the correlations, means, and SDs of all variables. The full model (Fig. 1) fit the data well: χ2 (2) = 2.017, p > 0.05; RMSEA = 0.002 (90% CI [0.000–0.038]); CFI = 1.000; and SRMR = 0.004. Absolute values of all standardized residuals were less than 0.1.
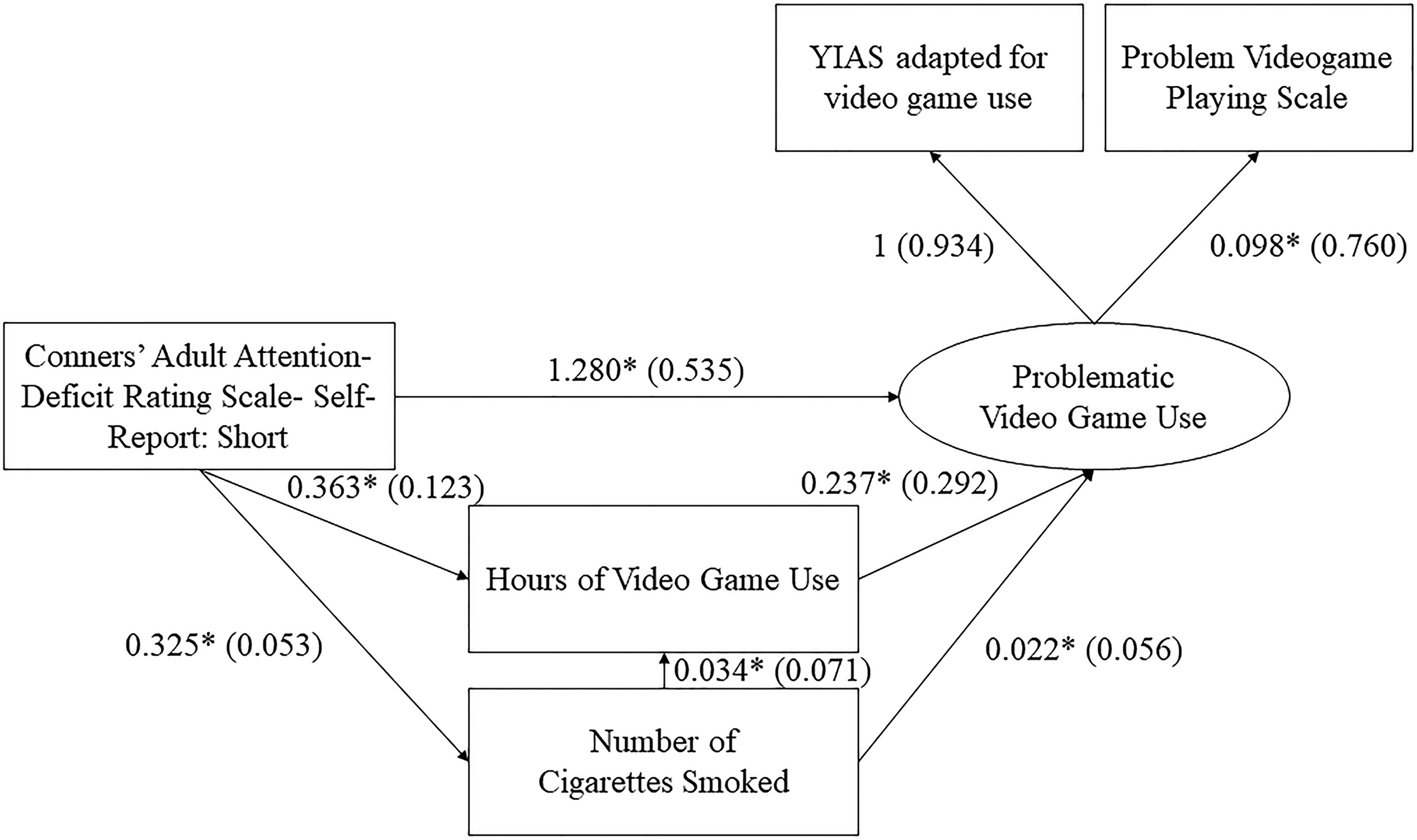
Full structural regression model predicting problematic video game use from Attention Deficit Hyperactivity Disorder symptomatology, hours of video game use, and smoking behavior. Standardized values are in parentheses. All freely estimated paths were significant. *p < 0.05. YIAS, Young's Internet Addiction Scale.
p < 0.01.
CAARS, Conners' Adult ADHD Rating Scale—Self-Report; PVP Scale, Problem Videogame Playing Scale; YIAS, Young's Internet Addiction Scale; SD, standard deviation.
As hypothesized, there were significant positive relationships among all variables in the model. For every one-point increase in ADHD symptomatology, participants reported smoking an additional one-third of a cigarette per week (b = 0.325, p < 0.05). For every one point increase in ADHD symptomatology, video game use increased by about 22 minutes per week (b = 0.363, p < 0.05) and PVGU increased by 1.280 points (p < 0.05). For every additional cigarette smoked, video game use increased by 2 minutes (b = 0.034, p < 0.05) and PVGU increased by 0.022 points (p < 0.05). Finally, for every additional hour of video game use, PVGU increased by 0.237 points (p < 0.05).
ADHD symptomatology explained 0.3 percent of variance in smoking behavior. ADHD symptomatology and smoking behavior together explained 2.1 percent of variance in video game use. ADHD symptomatology, smoking behavior, and video game use together explained 41.8 percent of variance in PVGU. In terms of the measurement model, the YIAS and PVP both loaded strongly and positively onto the PVGU factor; the standardized factor loadings were 0.934 and 0.760, respectively.
Discussion
The goal of the current study was to test relationships among potential correlates of PVGU. The proposed model fit the data well, and all hypothesized relationships were statistically significant. Results suggest that greater ADHD symptomatology, cigarette use, and video game use may all be associated with problematic use of video games. These findings are consistent with previous studies, which examined the independent effects of ADHD symptomatology,12,16,23–25 smoking,11,15,20 and video game use14,15,25 on PVGU.
The result of the current study, which suggests a relationship between smoking and PVGU (along with other correlates), is consistent with previous literature suggesting neurological similarities between substance and behavioral addictions. 9 Di Chiara 44 describes a motivational learning hypothesis in the context of addiction: an addictive stimulus is addictive in that it causes repetitive release of dopamine in the mesolimbic system, leading to strengthening of the stimulus-reward learning process. PVGU may be explained by this hypothesis; functional magnetic resonance images obtained during video game play indicate activation in the mesocorticolimbic system. 45 Ultimately, there are long-term changes in the reward system for individuals with PVGU that are similar with individuals with substance addictions. 46 Studies indicate similar neurological dysfunctions in individuals with pathological gambling and individuals with substance use disorders when compared to healthy controls, such as low levels of serotonin metabolite 5-hydroxyindole acetic acid in cerebrospinal fluid, 47 and low levels of ventral striatal activations that inversely correlates to severity of the addictive behavior. 48
ADHD symptomatology explained 0.3 percent of variance in smoking behavior, and ADHD symptomatology and smoking behavior together explained 2.1 percent of variance in video game use. These effect sizes are small, suggesting weak clinical significance despite current evidence suggesting a significant level of comorbidity between ADHD and smoking26,29 and the tendency for individuals with history of ADHD to start smoking regularly earlier than individuals without history of ADHD.27,28 However, it is important to remember that these relationships are reported after controlling for all other variables in the model, whereas these relationships were typically studied individually in previous studies. It is also possible that another unmeasured variable influences both ADHD and smoking behavior. For example, studies suggest that there may be some genetic explanation for both high levels of ADHD and smoking. 49 Also, there may be other variables that better predict video game use, such as negative self-esteem, 17 lower social competence, 6 and reinforcement characteristics of the video game. 50
While the individual correlates of PVGU had small effect sizes, the effect of the combined predictors on PVGU was large (41.8 percent), suggesting that it may be useful to consider these variables in combination in the assessment and treatment of PVGU. For example, clinicians treating clients with PVGU may benefit from tracking not only the amount of video game use but also clients' smoking behavior and current ADHD symptomatology. In addition, clinicians whose clients show high levels of ADHD symptomatology, cigarette use, and video game use may consider also assessing for PVGU and providing psychoeducation.
The YIAS and PVP were also tested to determine whether they measure the same construct (problematic play), which is important when determining whether results from studies using only one of these measures are comparable. The factor loadings of these two scales were strong, suggesting that both scales are measuring PVGU, that either one may be used to assess PVGU, and that findings from existing studies using either of these instruments may be more readily compared to each other. The shorter PVP may be useful when a quick screening instrument is needed, while the longer YIAS may be more helpful in capturing a wider range of PVGU severity in situations where time is less limited.
The current study has a number of strengths, including the large international sample and a more thorough assessment of PVGU than in previous research. However, the results should be interpreted in light of several limitations such as the use of an eight-item version of the PVP scale. While it is uncertain how the fit of the model would change if the full nine-item scale were used, the eight-item version shared a significant amount of common variance with our other measure of PVGU (the YIAS), suggesting that its performance may be roughly equivalent to the nine-item version. Nonetheless, comparison studies of the two versions are required before stronger conclusions about measurement equivalence can be drawn. Only 5.6 percent of our sample met criteria for clinically significant ADHD symptomatology (T ≥ 65). However, there was still a significant relationship between ADHD symptomatology and PVGU, suggesting that even subclinical levels of ADHD symptomatology may be associated with PVGU.
Another limitation is that the sample was predominantly male and Caucasian, making it difficult to generalize our findings to females and individuals of other racial and ethnic backgrounds. In addition, the data are cross-sectional; therefore, we cannot infer causal relationships among the variables. The data were also collected via self-report. Respondents may have poor insight about their behavior or may minimize problems with addiction-like behavior.
Conclusions and Implications
Together, ADHD symptomatology, smoking behavior, and the amount of video game use appear to have a significant impact on PVGU. Tracking these variables may be helpful for clinicians treating clients with or at risk for PVGU. In addition, results indicate that the YIAS and PVP measure the same construct, suggesting that either scale may be used as a screening instrument for PVGU, and that results from studies using either of these scales may be compared with each other. Future studies may benefit from examining additional variables that may explain PVGU, such as cognitive and affective variables that may contribute to PVGU directly or indirectly through ADHD, smoking, or amount of video game use.
Footnotes
Author Disclosure Statement
No competing financial interests exist.