
Abstract
Abstract
Internet gaming disorder (IGD) is characterized by addiction to online gaming and reduced executive control, particularly when individuals are exposed to gaming-related cues. Executive control can be measured as vagally mediated heart rate variability (HRV), which corresponds to variability in the time interval between heart beats. In this study, we investigated whether individuals with IGD have altered HRV while playing online games. We hypothesized that while gaming, individuals with IGD would exhibit phasic suppression of vagally mediated HRV, which would reflect executive control dysfunction during game play. To test this, we measured the changes of HRV when young males with IGD were engaged in real-time online gaming. The changes of HRV were associated with the severity of IGD assessed by self-reports and prefrontal gray matter volume (GMV) calculated by voxel-based morphometry. We included 23 IGD subjects and 18 controls in our analyses. Changes in HRV were not statistically different between IGD subjects and controls. Within the IGD group, however, subjects showed significant decreases in high-frequency (HF) HRV during gaming. Furthermore, the degree of decrease correlated with IGD severity and prefrontal GMV. Importantly, this phasic suppression of HF-HRV in response to gaming did not occur in control subjects. In conclusion, young males with IGD showed an altered HRV response while playing an online game, reflecting their difficulties in executive control over gaming. The dynamics between executive control and reward seeking may be out of balance during game play in IGD.
Introduction
I
Recent comparative studies of recreational Internet game users showed that individuals with IGD have difficulty exerting executive control.3,4 Executive control is the ability to perform goal-directed behavior and self-regulation using higher order cognitive functions. 5 In the context of IGD, executive control dysfunction would prevent individuals from efficiently controlling the urge to play and adjusting their behavior appropriately to a long-term goal. The executive control dysfunction of individuals with IGD is consistent with previous studies that reported decision-making deficits, 6 impaired response inhibition, 7 and prominent impulsivity 8 in IGD. A number of neuroimaging studies have also provided strong support for the involvement of executive control-related brain regions in IGD. 9 In particular, it has been found that the prefrontal cortex, which plays a key role in executive control, 10 is involved in the pathophysiology of IGD.11,12
Although studies have indicated executive control deficits in IGD, the results of the behavioral tasks measuring executive control were not consistent. 13 Some studies showed that behavioral performance in decision-making tasks and inhibitory control tasks did not differ between IGD subjects and controls.14,15 We speculate that these findings may be due to the lack of gaming-specific cues in the course of performing the tasks. Recent studies have suggested that not only impaired executive control but also enhanced reward seeking triggered by cue reactivity plays important roles in the loss of control over online gaming.16,17 The disease model of IGD proposed that a dysfunctional interaction between executive control and reward seeking as a response to gaming-related cues may underlie excessive Internet gaming. 18 Consistent with this view, individuals with IGD appear to be more severely affected by executive control dysfunction when they are confronted with gaming-related cues. In gaming cue-specific versions of tasks, individuals with IGD exhibited cognitive inflexibility, 19 reduced inhibitory control, 15 and impaired working memory. 20 Thus, we inferred that the executive control dysfunction of individuals with IGD would become more apparent while playing online games.
The neurovisceral integration model proposed that neural networks related to autonomic and cognitive self-regulation were implicated in the control of cardiac vagal functions. 21 Heart rate variability (HRV), which is a physiological phenomenon of variations in the time interval between heart rates, has been suggested to index not only autonomic functions but also the capacity of cognitive self-regulation. 22 HRV under resting state and during mental loads has been associated with self-regulatory efforts.23,24 In particular, several lines of evidence have indicated that vagally mediated HRV (i.e., high-frequency [HF] HRV) may be closely associated with prefrontal neural functions and executive control. 25 The resting levels of vagally mediated HRV predict the individual differences in executive functioning.26,27 In addition, a greater reduction in vagally mediated HRV during mental tasks has been linked to inefficient prefrontal control over cognitive performances. 28 Given these relationships between vagally mediated HRV and executive control, measuring the vagally mediated HRV while playing online game might be highly informative to evaluate the difficulties for executive control during game play.
The aim of this study was to assess HRV changes in individuals with IGD while playing online games. We speculated that phasic suppression of vagally mediated HRV during a specific behavior would reflect impaired executive control over the behavior. We also speculated that individuals with IGD may show difficulties for executive control, in particular, when they are engaged in real-time online gaming. Thus, we hypothesized that vagally mediated HRV would be highly suppressed in IGD subjects, especially during game play. In addition, we hypothesized that this phasic HRV suppression may be associated with the severity of IGD and the gray matter volumes (GMVs) of the prefrontal cortex.
In this study, young males with IGD underwent an HRV recording while they were performing a continuous performance task and playing an online game. The continuous performance task is a neuropsychological test that has been used to measure general executive functions such as sustained attention and response inhibition. 29 For HRV data during game play, we focused on the early time in the game (for 5 minutes), because this period is less affected by the real-time state of gaming such as the outcome of the battle. To test our hypotheses, we compared the longitudinal changes of HRV between IGD subjects and controls. Because we were particularly interested in phasic HRV changes in IGD subjects, we also analyzed HRV changes within discrete time periods (resting state, during the continuous performance task, and during game play) for each group, respectively. Then, we tested correlations between phasic HRV changes and the severity of IGD and the GMVs of the prefrontal cortex.
Materials and Methods
Subjects
This study was conducted from June 2016 to August 2017. Institutional review board approval (HYI-16–044) was obtained for this study, and each subject provided written informed consent before participation. Subjects were recruited via online advertisements, flyers, and word of mouth. Forty-one young males participated in the study, all right handed, and aged between 16 and 27 years (mean age: 23.1 ± 2.6 years). All subjects were evaluated for sociodemographic characteristics and Internet use patterns.
The presence of online game-related problems was screened by using the Internet Addiction Test (IAT). 30 IGD subjects were classified as individuals who primarily used the Internet for online gaming and scored over 50 on the IAT31,32 (n = 23; age, 22.7 ± 2.8 years). All IGD subjects had been playing the online game “League of Legends (LOL)” (Riot Games, 2009) as their primary online gaming activity. To ensure reliable diagnoses of IGD, a board-certified psychiatrist conducted clinician-administered interviews using diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) classification for IGD. 33 In particular, all IGD subjects satisfied the criterion that they continued gaming despite social problems, which is considered a valid and accurate diagnostic for IGD. 34 Subjects who scored below 50 on the IAT were assigned to the control group (n = 18; age, 23.5 ± 2.3 years). The 40-item Korea Internet Addiction Scale (K-scale) was used adjunctly to the IAT to assess the severity of online game-related problems. 35
All subjects undertook the structured clinical interview from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (SCID) 36 to test for the presence of other psychiatric disorders, and the Korean version of the Wechsler Adult Intelligence Scale IV (WAIS-IV) 37 to estimate intelligence quotient (IQ). The exclusion criteria in this study were the following: having significant psychiatric symptoms other than IGD-related symptoms (e.g., depression, anxiety), neurological disorder or medical illness that affected the HRV (e.g., cardiac disease or endocrine disease), having low intelligence or difficulty in comprehending the questionnaires, and taking medications that affected the HRV (e.g., beta blockers or anticholinergics). All subjects in this study were psychiatric medication naive at the time of evaluation.
Procedure
After a rest period of at least 10 minutes, the resting-state electrocardiogram (ECG) recording was conducted for 10 minutes while in a comfortable sitting position (baseline HRV). Afterward, the Conners' continuous performance task (CPT; length, approximately 14 minutes)
38
was performed and an ECG recording was taken during the CPT (during the CPT HRV). Detailed procedures for the CPT are presented in the Supplementary Data section (Supplementary Data are available online at
After the HRV recording ended, each participant completed several self-report questionnaires to assess comorbid psychiatric symptoms of IGD. 39 All subjects completed the Beck Depression Inventory (BDI) 40 to test for depression, the Beck Anxiety Inventory (BAI) 41 to test for anxiety, the Alcohol Use Disorders Identification Test (AUDIT) 42 to identify alcohol-related problems, the Wender Utah Rating Scale (WURS) test to evaluate for childhood symptoms of attention-deficit/hyperactivity disorder (ADHD), 43 and the Barratt Impulsiveness Scale, version 11 (BIS-11) 44 to evaluate for impulsivity.
After the experiments with HRV monitoring and self-reports, participants underwent structural magnetic resonance imaging (MRI) analyses within a week. Detailed procedures for the MRI analysis are presented in the Supplementary Data section.
HRV data acquisition and processing
ECG signals were collected using a standard 3-channel ECG instrument and monitoring system (MP150 BIOPAC Systems, Santa Barbara, CA). The Ag-AgCl electrodes were attached in accordance with the Einthoven triangle superimposed on a human thorax. 45 Specifically, the positive electrode was attached to the left lower abdomen, the negative electrode to the right shoulder, and the ground electrode to the left shoulder, respectively. 46 After the ECG signals were acquired, data were preprocessed to remove noise from subjects' movement, breathing, and muscle electrical activity. Third-order Butterworth high-pass filtering with a 0.1 Hz cutoff frequency was performed to remove baseline wander, and a sixth-order Butterworth notch filter was applied to remove 60 Hz power line interference. 47 Third-order Butterworth low-pass filtering with a 15 Hz cutoff frequency was used to filter electromyogram artifacts from the ECG signals. 48 Then, all RR intervals on the ECG were detected using the Pan and Tompkins algorithm. 49 ECG signals were sampled at a frequency of 200 Hz. We removed the beat with a difference of consecutive RR intervals of more than 10%, and resampled at 10 Hz using cubic spline interpolation. 50
HRV data analysis
Among the time domain parameters of HRV, the square root of the mean of the sum of the squares of differences between consecutive RR intervals (RMSSD), the standard deviation of the RR interval (SDNN), and the percentages of adjacent RR intervals differing by >50 ms (pNN50) were obtained. While the SDNN represents overall HRV, the RMSSD and pNN50 are relatively sensitive to vagal tone. 51 We also acquired the power spectral density of HRVs by autoregressive spectral analyses. 52 We used a logarithmic transformation to control the skewed distributions of the HRV parameters. Among the frequency domain parameters of HRV, the high-frequency (HF-HRV: 0.15–0.40 Hz), low-frequency (LF-HRV: 0.04–0.15 Hz), and very low-frequency (VLF-HRV: 0.003–0.04 Hz) HRV were obtained. Although LF-HRV is influenced by both sympathetic and vagal activity, HF-HRV represents pure vagal activity. 53 Finally, VLF-HRV is associated with sympathovagal balance and is related to recovery from mental stress. 54
Statistical analyses
To compare demographic or psychometric characteristics, behavior results of CPT, and absolute values of HRV between IGD subjects and controls, we conducted independent t-tests and χ 2 tests. To test for differences in regional GMVs in the prefrontal cortex, the analysis of covariance (ANCOVA) with total intracranial volume (TICV) as covariate was performed. To test for group differences in longitudinal changes of HRV, mixed-model analysis of variance (ANOVA), using period (baseline, during the CPT, and during the game) as the within-subjects factor, and group (IGD subjects or controls) as the between-subjects factor, was performed. Subsequently, the two groups were further analyzed independently to examine for significant phasic changes in HRV within each group. For each HRV parameter in each group, three paired-samples t-tests with Bonferroni corrections (threshold with p < 0.05/3 or 0.0167) were conducted for comparisons between time periods (baseline vs. during the CPT, baseline vs. during the game, and during the CPT vs. during the game, respectively).
In cases where significant phasic HRV changes were found, Pearson correlation analyses were conducted to investigate the associations between the phasic HRV changes and the severity of IGD. To test for associations between phasic HRV changes and regional GMVs, partial correlation analyses controlling age and TICV were conducted.55,56 Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 24.0 K (SPSS, Inc., Chicago, IL). The level of statistical significance was set at p < 0.05.
Results
The demographics, clinical characteristics, and behavioral results of the subjects
Demographic variables (age, IQ, educational level, socioeconomic status, BMI, exercise level, and cigarette smoking status) were not significantly different between IGD subjects and controls (Table 1). IGD subjects spent significantly more time gaming weekly than did the healthy controls (t = 3.594, p = 0.001). IGD subjects scored significantly higher on the severity of online game-related problems (IAT: t = 9.799, p < 0.001; K-scale: t = 4.491, p < 0.001). K-scale results positively correlated with IAT scores (within all subjects: r = 0.560, p < 0.001; within IGD subjects: r = 0.594, p = 0.003). IGD subjects and controls did not significantly differ in self-reporting depression, anxiety, alcohol-related problems, and childhood ADHD symptoms. IGD subjects scored significantly higher on tests of impulsivity compared with controls (BIS: t = 3.299, p = 0.002). The behavioral results on the CPT (errors of omission, errors of commission, hit reaction time, and standard error of CPT hit reaction time) did not differ between IGD subjects and controls (Supplementary Table S1).
p < 0.05.
Intelligence Quotient was assessed with the Wechsler Adult Intelligence Scale.
Wender Utah Rating Scale was performed to assess childhood ADHD symptoms.
HRV and structural MRI analyses
All HRV parameters (RMSSD, SDNN, pNN50, HF, LF, and VLF) at rest, during the CPT, and during the game are presented in Table 2. At every period, all HRV parameters did not significantly differ between IGD subjects and controls in independent t-tests. For all HRV parameters analyzed by mixed-model ANOVA, interactions between period and group and the main effect of group were not statistically significant (Supplementary Table S2). A main effect of period was statistically significant for the HF-HRV (F [2, 78] = 4.323, p = 0.017, partial eta-squared = 0.100) and the SDNN (F [2, 7] = 4.301, p = 0.017, partial eta-squared = 0.099). The main effects of period for other HRV parameters were not statistically significant.
The resting-state HRV recording was conducted for 10 minutes while in a comfortable sitting position.
The continuous performance task (CPT; length, approximately 14 minutes) was performed and HRV recording was taken.
Subjects underwent an HRV recording while they were playing the Internet game, “League of Legends (LOL).” HRV data for the early time in the game (5 minutes) were analyzed.
HF-HRV, high-frequency heart rate variability; LF-HRV, low-frequency heart rate variability; VLF-HRV, very low-frequency heart rate variability; RMSSD, root mean square of successive differences; SDNN, standard deviation of the normal-to-normal interval; pNN50, proportions of adjacent normal-to-normal intervals differing by >50 ms.
Analysis using a paired-samples t-test revealed that IGD subjects exhibited significant differences in the HF-HRV between the periods during the CPT and during the game (t = 2.796, p = 0.011; Table 3 and Fig. 1A). However, these parameters were not significantly different for control subjects (t = 1.256, p = 0.226; Fig. 1B). All other HRV, parameters were not statistically significant, as determined by paired-samples t-tests (Supplementary Tables S3–S7).
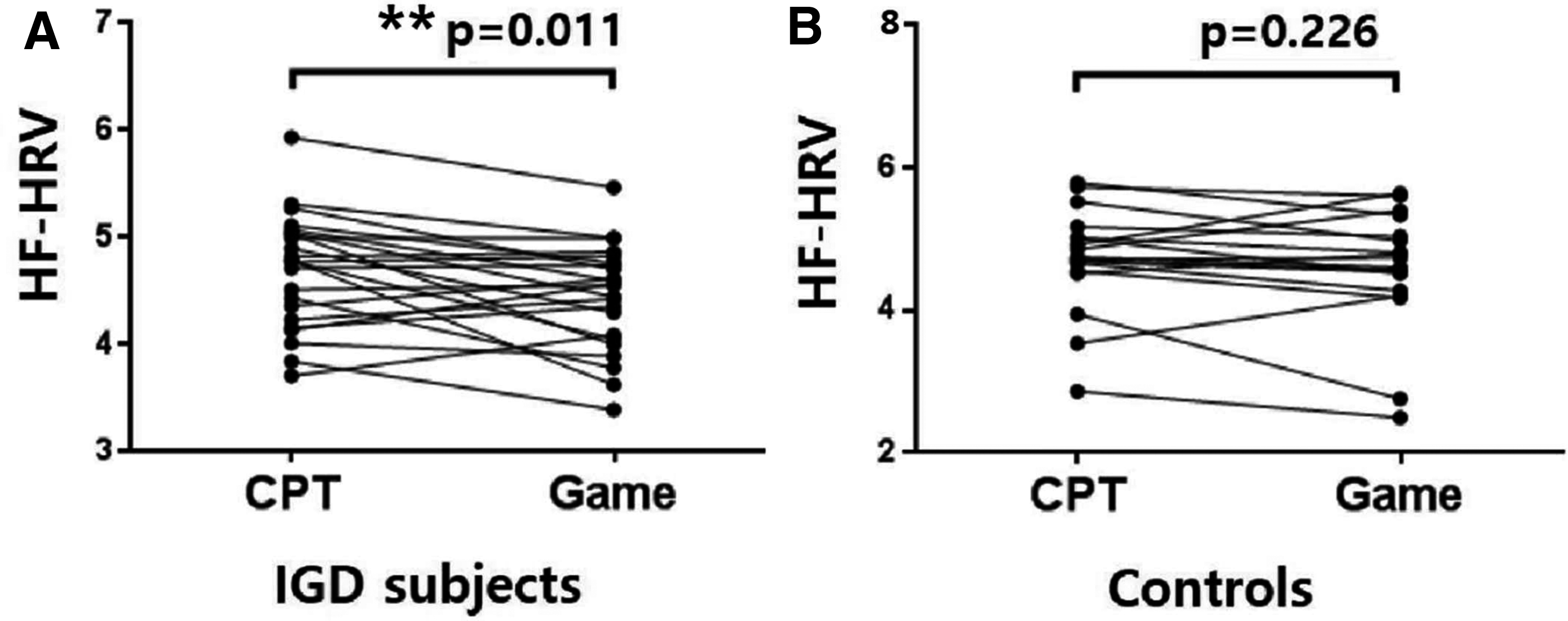
Paired-samples t-tests between during the CPT and during the game were used for HF-HRV.
p < 0.05/3 or 0.0167.
The resting-state HRV recording was conducted for 10 minutes while in a comfortable sitting position.
The continuous performance task (CPT; length, approximately 14 minutes) was performed and HRV recording was taken.
Subjects underwent an HRV recording while they were playing the Internet game, “League of Legends (LOL).” HRV data for the early time in the game (5 minutes) were analyzed.
Structural MRI data were analyzed, and TICV did not differ significantly between the IGD subjects and controls in independent t-tests (1702.60 ± 95.04 cm3 for IGD subjects; 1637.23 ± 112.98 cm3 for controls; t = 1.934, p = 0.061). The GMVs on both sides of the dorsolateral prefrontal cortex (DLPFC) and the ventrolateral prefrontal cortex (VLPFC) did not differ between the IGD subjects and controls in the ANCOVA, when controlling for TICV.
Correlation analyses
To represent the degree of phasic HF-HRV suppression in response to the game, ΔHF-HRV was calculated by subtracting HF-HRV during the game from HF-HRV during the CPT. Within IGD subjects, ΔHF-HRV was significantly correlated with the severity of online game-related problems (IAT: r = 0.431, p = 0.040; K-scale: r = 0.638, p = 0.001; Fig. 2A). ΔHF-HRV in the IGD subjects was also inversely correlated with regional GMVs in the left DLPFC and the right VLPFC (the left DLPFC: r = −0.455, p = 0.044; the right VLPFC: r = −0.481, p = 0.032; Fig. 2B). Correlation tests in controls did not reach statistical significance.
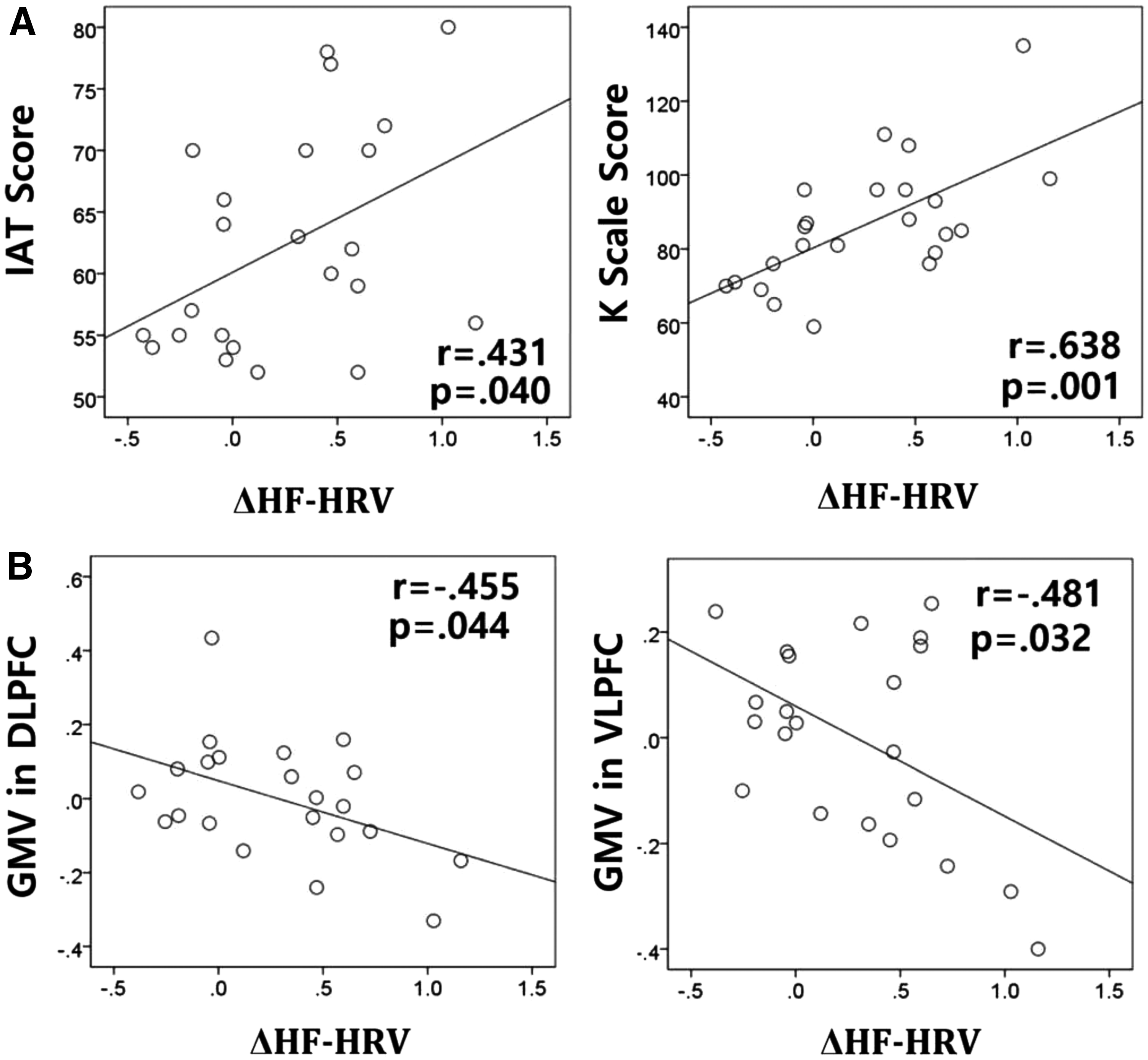
Correlation analysis within IGD subjects.
Discussion
We investigated altered patterns of HRV responses while playing online games in young males with IGD. During the experiment, IGD subjects and controls played an online game (“League of Legends”; LOL) followed by undergoing a neuropsychological test (the continuous performance task; CPT). We hypothesized that vagally mediated HRV would be suppressed in IGD subjects, especially during real-time online gaming. By contrast, our study revealed that group differences in HRV changes between IGD subjects and controls were not statistically significant. Within the IGD group, however, subjects had significantly lower HF-HRV during the game compared with during the CPT. Although not proven by comparison analyses with controls subjects, this decreased HF-HRV in IGD subjects during game play was consistent with our hypothesis that IGD subjects exhibit phasic suppression in vagally mediated HRV during game play.
Importantly, HF-HRV is modulated by vagal (parasympathetic) activity and is a useful biomarker of executive control and prefrontal neural function. 28 Furthermore, we found that the degree of phasic decrease in HF-HRV during game play was significantly associated with the severity of online game-related problems. We also found that the changes in HF-HRV were negatively correlated with regional GMVs of the prefrontal cortex. These findings supported our hypothesis that phasic HRV changes while playing online games may be closely related with loss of control over gaming in individuals with IGD.
Unlike during game play, IGD subjects did not exhibit significant phasic HRV changes during the CPT (comparison between “baseline” and “during the CPT”). There were also no differences between IGD subjects and controls in behavioral performance of the CPT. However, IGD subjects showed significant phasic HF-HRV suppression when they were engaged in real-time online gaming (comparison between “during the CPT” and “during the game”) that reflected their executive control dysfunction. Our findings are in agreement with previous results that demonstrated more prominent executive control deficits under gaming-related conditions.15,19 The disease model of IGD suggested that a dysfunctional interaction between executive control and reward seeking underlies the loss of control over Internet gaming. 18 As a result of enhanced reward seeking triggered by gaming-related cues, the dynamics between executive control and reward seeking may be out of balance during game play. A shift in this balance may underlie the difficulty IGD subjects experience when exerting executive control over online gaming, leading to uncontrolled and excessive online gaming. Our findings of significant correlations between phasic HF-HRV suppression during game play and the severity of online game-related problems support this speculation.
Numerous studies have indicated alterations of the prefrontal cortex in IGD. 11 Long-lasting excessive Internet gaming has been related with reduced GMV in the DLPFC 57 and the VLPFC. 58 Previous functional MRI studies have shown that individuals with IGD had altered prefrontal activation in response to gaming cues.59,60 In the current study, we found phasic HF-HRV suppression during game play in IGD subjects, and this phasic suppression of HF-HRV was correlated with GMVs in the left DLPFC and the right VLPFC. Given that brain structural properties affect functional neural activity, 61 our finding of an association between phasic HF-HRV changes and GMVs of the prefrontal cortex supports the proposed role of HRV in indexing prefrontal cortical activity. 25 The prefrontal cortex cooperates with other cortical and subcortical areas to modulate executive control function. 10 We speculate that the association between an altered autonomic response to gaming and loss of control over gaming in IGD is mediated by prefrontal dysfunctions.
Ultimately, this study suggests that individuals with IGD have a characteristic HRV response (phasic HF-HRV suppression) while playing online games. Our investigation of HRV changes in individuals with IGD has several clinical implications. HRV is a biomarker that can be monitored noninvasively and conveniently during a short-term period. Therefore, if the characteristics of HRV in IGD are verified, this can be useful for evaluating IGD symptoms and monitoring treatment efficacy. Furthermore, HRV biofeedback can be used as an interventional tool. Indeed, HRV biofeedback has been used previously to treat addiction 62 or develop behavioral control.63,64 Thus, efforts to enhance understanding of different aspects of the HRV response to gaming can provide new therapeutic possibilities for patients with IGD.
Limitations
There were several limitations to the present study. First, HRV changes during each period did not differ significantly between IGD subjects and controls in the mixed-model ANOVAs and independent t-tests. This is not surprising, as absolute values of HRV parameters can have wide interindividual variations due to the influence of various individual psychosocial factors and physical conditions. 65 Given the large variation in HRV, our small sample size likely limited the statistical power of our group comparisons. Altered HRV responses to gaming in individuals with IGD may be more clearly demonstrated by measuring changes in HRV while performing a variety of tasks on a larger number of subjects, and then comparing them with HRV changes during game play.
Second, this study did not include an analysis of behavioral performance that could reflect executive control dysfunction during game play. Although previous studies suggest that phasic suppression of HF-HRV reflects executive control dysfunction,22,25 this study lacks direct evidence of this phenomenon as we did not directly measure executive control. Furthermore, we only analyzed HRV data that were recorded early in game play, and the changes in HRV in response to specific game events were not evaluated in this study. Future studies, including an analysis of the behavioral characteristics of individuals with IGD during specific game events and their accompanying HRV responses, may expand on our current findings and support appropriate interpretations.
Third, because this study measured HRV during real-time online gaming, it is possible that there was noise in the HRV signal due to physical movements (i.e., neck motion, wrist movement). To control for this, we instructed subjects not to engage in activities not related to game play and used various filters to remove noise from the data in the analytic processes. However, future studies might collect and consider several biological signals that can reflect the subject's physical condition (i.e., electrooculogram and electromyogram), more accurately reflecting HRV during game play.
Finally, because a cross-sectional design was used in this study, it was difficult to determine whether executive control dysfunctions indexed by phasic HF-HRV suppression led to a vulnerability for IGD, or long-lasting excessive gaming distorts the patterns of HRV responses to gaming. A longitudinal design study of the HRV features in individuals with IGD will be needed to clarify the causal relationship between altered autonomic response to gaming and loss of control over gaming.
Conclusion
In conclusion, young males with IGD showed significant decreases in HF-HRV while playing online games, indicating diminished executive control over gaming. The degree of HF-HRV suppression correlated with severity of IGD and GMVs of the prefrontal cortex. These findings suggest that the balance between executive control and reward-seeking behavior is shifted during game play in individuals with IGD. In the future, HRV responses to gaming may be a useful therapeutic target for IGD.
Footnotes
Acknowledgments
This research was supported by the Original Technology Research Program for Brain Science through the National Research Foundation of Korea funded by the Ministry of Science, ICT & Future Planning (NRF-2015 M3C7A1064906).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.