
Abstract
Abstract
Problematic video gaming (PVG) is a concern for psychologists attending children and adolescents. Uniform diagnostic criteria are lacking, and risk factors are poorly understood. Internet gaming disorder (IGD) was included in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), and scales derived from its diagnostic criteria may be helpful to assess PVG. A multicenter study was conducted in secondary schools using an IGD-derived scale (dichotomous Nine-Item Internet Gaming Disorder Scale [IGD-9]), analyzing PVG-related variables. Seven hundred eight students (55.8 percent male) with mean age 15.6 ± 2.7 years were included. Seventy-three percent were gamers and 22 percent heavy gamers (HGs). Forty-five percent reported online gaming and 6.6 percent massive multiplayer online role-playing games (MMORPGs). Fifty-nine students (8.3 percent) scored 5 or more in IGD-9 and were classified as IGD+. HG and IGD+ subjects were more frequently male and online and MMORPG gamers (p < 0.01). However, IGD+ subjects had significantly worse psychosocial scores than IGD− (p < 0.001), while HGs did not significantly differ from casual gamers (p > 0.01). The multivariate analysis showed that IGD+ scores were significantly associated with worse psychosocial health and adjustment (p < 0.001), while the other variables (male sex, online and MMORPG gaming, and HG) were not significantly associated (p > 0.01). The IGD-9 scale scored positive in 8.3 percent of our sample. Unlike gaming time, this scale was associated with psychosocial disturbances, making it potentially useful as a screening method to detect candidates for clinical intervention.
Introduction
I
However, many scholars are overtly against the definition of PVG as a mental disorder, at least the way IGD was defined. IGD criteria have been selected following substance abuse and gambling disorders, and consensus regarding the main symptoms and how to assess them is lacking. In addition, overdiagnosis may have negative medical, social, and scientific consequences and lead to video gamers' stigmatization. 5
The risk factors for PVG have been difficult to establish as most of the literature consists of transversal studies, and the diagnostic criteria for PVG are heterogeneous. Male sex, psychopathological conditions, impulsivity, gaming time, and certain online gaming subtypes are deemed possible candidates. 6 First, boys are more prone to engage in VG than girls (who tend to find social networking and chatting via technology products more attractive). 7 Males generally spend more time with VG and are at least three times more likely to engage in PVG (from 5 to 12 percent in males to 1 to 4.6 percent in females).8–10
Although the associations have been well established, it is controversial whether psychopathological conditions such as depression, social anxiety and isolation, and low self-esteem are causes or consequences of PVG.10–12 Online VG avatars may be seen by gamers as better adjusted, competent, and satisfactory than their real self and be used to relieve these negative feelings. 13 In a 2-year prospective study, impulsiveness and poor social competence were risk factors to engage in PVG, while depression, social phobia, and poor academic performance were consequences. 6
As for time devoted to gaming, it remains controversial whether gaming time may contribute per se to PVG. 14 The threshold for gaming time to be considered excessive has not been properly established, and long followup prospective studies are lacking. In a 2-year followup study, gaming time appeared as a risk factor for PVG. 6 However, in other studies, gaming time failed to remain significant in multivariate analyses (unlike impaired functioning as measured by sustainable development goals and the Weiss Functional Impairment Rating Scale Parent-Based), suggesting that PVG is not simply playing a lot.8,9,15 Although children with PVG do tend to increase their gaming time in a medium term,15,16 some authors consider that spending high amounts of time in VG is not exclusive of PVG, and this pattern may be consistently found in psychologically healthy gamers. 17
Online gaming is rapidly spreading, and online games, especially massive multiplayer online role-playing games (MMORPGs), have been consistently linked to addictive gaming. 18 The incidence of PVG among MMORPG gamers varies widely (3.6–44.5 percent) depending on the measurement method, and dramatic consequences such as poor academic performance and self-neglect have been reported.19,20 This led the DSM-5 to name the problem IGD, rather than simply gaming disorder. 21 Nine criteria covering the main features of an addiction disorder (salience, mood modification, tolerance, withdrawal symptoms, conflict, and relapse) are proposed. 22 Fulfilling five criteria within the past 1 year would be diagnostic. Since IGD was described, many authors in recent studies (2014–2016) have explored its prevalence mostly through DSM-5 criterion-derived scales. The results vary widely from 0.7 to 15.6 percent, depending on the measurement method, age, and geographical area. 23
In 2015, Lemmens et al. published the Nine-Item Internet Gaming Disorder Scale (IGD-9), demonstrating its good psychometric properties and association with poor psychosocial functioning in a large, representative nonclinical sample. 24 The questions proposed have a strong clinical sense and seem to be a feasible instrument for caring psychologists or school counselors to explore PVG symptoms.
Given the PVG definition controversy, it is necessary to provide more data from diverse populations to help experts better describe and study this complex phenomenon. In this study, we aimed to estimate the frequency of IGD in a sample of Spanish students from several urban secondary schools. The measuring instrument was the IGD-9 scale, which requires a minimum of five affirmative answers to diagnose IGD, following DSM-5 criteria. Second, we aimed to analyze whether scoring positive in IGD-9 was associated with a poor psychosocial status. Finally, we analyzed whether variables linked with PVG in scientific literature (male sex, gaming time, and online/MMORPG gaming) were associated with IGD in our sample.
Methods
Our research team of the University of Málaga (UMA), with the institution's approval, designed an observational transversal study to analyze a sample of students aged between 12 and 18 years in the city of Málaga. Málaga is one of the biggest cities in the south of Spain, with a population of 569,000. Four public and publicly funded private schools from different socioeconomic areas of the city were selected. Subjects of interest were nonselected students from compulsory secondary education (Educación secundaria obligatoria, 12–16 years), baccalaureate (Bachillerato, the grade required to access university, 17–18 years), and vocational training (technical specialist certificates, 17–18 years).
Self-administered, confidential, and anonymous paper and pencil questionnaires were distributed by school counselors and completed voluntarily by students in class. Questionnaires included the IGD-9 scale, which is available in Appendix 1. Questionnaires included demographic data (gender, age) and the use of video games in any device (personal computer, cell phone, tablet, handheld console, or home console), as well as the use of online games and/or MMORPGs. Questions regarding gaming time (days of the week and hours a day) were included. In the absence of consensus criteria for heavy gaming, we defined the threshold on an empirical basis, derived from our experience as clinical psychologists. Whenever gaming time exceeded a mean of 2 hours a day at least 5 days a week or binge gaming (at least 5 hours of consecutive gaming) was reported, the student was classified as a heavy gamer (HG). Otherwise, students who played fewer hours were classified as casual gamers (CGs).
To assess problematic gaming features, we selected the IGD-9, developed by Lemmens et al., with proven psychometric properties (Cronbach's α 0.93). 24 It consists of nine dichotomous questions regarding gaming features in the previous year, and a score of 5 or more (affirmative answers) qualified a subject as IGD+. The Spanish version of this scale, previously published by Petry et al., 25 was elaborated following translations conducted using the World Health Organization's recommendations regarding the process of translation and adaptation of instruments. 24 Omega coefficient (ω) analysis was designed to assess reliability and validity of the scale in our sample.
Finally, psychosocial health and adjustment were explored by five different subscales, as reported previously, 24 assessing areas frequently related with addictive disorders. Self-esteem was measured with five items from the Self-Esteem Scale 26 ; satisfaction with life with the five-item Satisfaction with Life Scale 27 ; prosocial behavior with the five prosocial items from the Strengths and Difficulties Questionnaire 28 ; physical aggression with seven items from the Physical Aggression subscale from Buss and Perry's Aggression Questionnaire 29 ; and loneliness with 5 questions from the 20-item UCLA Loneliness Scale. 30 With the exception of satisfaction with life, all scales were shorter versions of the original scales. The items had been selected in the aforementioned work by measuring confirmatory factor analysis. 24 Questions in all scales were answered in a semiquantitative 5-item Likert-type scale: totally disagree (1) to totally agree (5). Items reflecting positive feelings were reverse coded. Total score and subscale scores were measured quantitatively, a higher score indicating poorer psychosocial health and adjustment.
Analysis strategy
The associations among main variables (IGD+ score, psychosocial health and adjustment, gaming time, and HG status) and secondary variables (gender, age, and online and MMORPG gaming) were analyzed with appropriate statistical tests (Student's T for quantitative variables and χ2 for qualitative variables) with a level of significance set at alpha = 0.01. This stricter level of significance was selected to reduce the likelihood of a type I error: since we applied an IGD scale conceived for a clinical setting (mental health services) in a nonclinical setting (school-based questionnaire), the positive predictive value diminishes, increasing the likelihood of observing false positive results. Multivariate analysis (logistic regression) was applied to rule out potential confounders among statistically significant variables. G-Stat 2.0 software and SPSS were used for statistical analysis.
Results
From December 2015 to February 2016, questionnaires were distributed with a response rate of nearly 100 percent (only two students refused to fill the questionnaire). Thus, 708 students (55.8 percent of them male) with a mean age of 15.6 ± 2.7 years were included. Demographic variables are detailed in Table 1. Gaming variables are detailed in Table 2. A majority (516, 72.8 percent) of the surveyed students were gamers (defined as VG at least once a week), and the remaining 192 (27.2 percent) were nongamers (Fig. 1). Students' gaming time is detailed in Table 3. Among gamers, 157 (22.2 percent) fulfilled the criteria for HGs, while 359 (77.8 percent) did not and were classified as CGs. Online gaming was also frequent (45.2 percent) in the sample, but only 6.6 percent of the students specifically played MMORPGs.
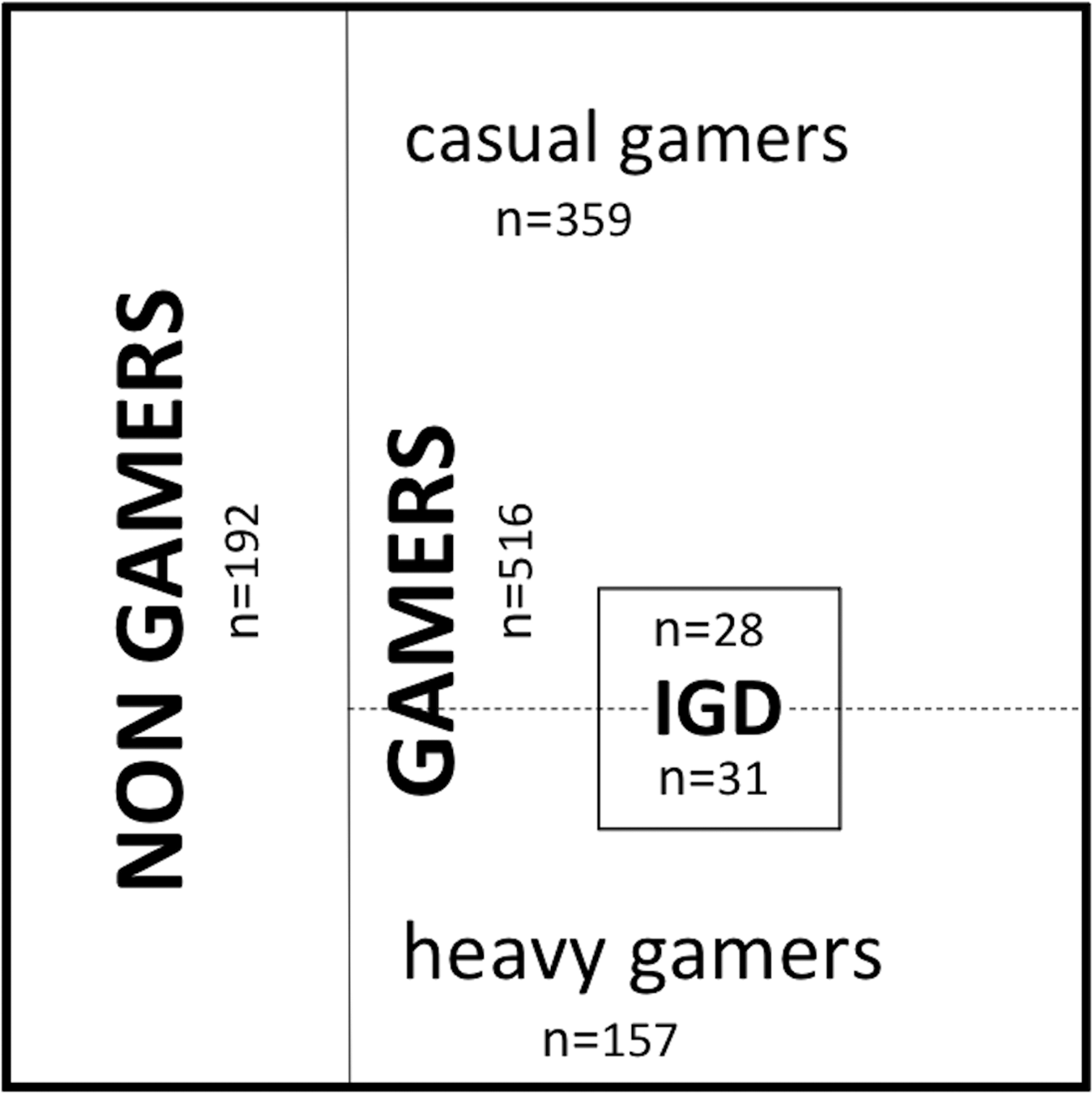
Distribution of frequencies of gamers (heavy gamers and casual gamers) and IGD+ subjects (subjects scoring 5 or higher in the IGD-9 scale) in the sample. IGD-9, Nine-Item Internet Gaming Disorder Scale.
F, female; M, male; SD, standard deviation.
χ2 test was used for proportion comparisons and Student's T test for mean comparisons. Significant differences (p < 0.01) are indicated with (*). ES measures are shown in significant differences between brackets (Cohen's D for Student's T test in quantitative variables and Cramer's V for χ2 test in qualitative variables).
ES, effect size; IGD, Internet gaming disorder; IGD-9, Nine-Item Internet Gaming Disorder Scale; HG, heavy gamer.
As for reliability of the IGD-9 scale in our sample, the omega coefficient (ω) was 0.81 (values considered acceptable lay between 0.70 and 0.90). Mean IGD score was 2.1 ± 1.8 and 59 students (8.3 percent) scored 5 or more and were classified as IGD+ (Table 3). These numbers are within the range found in several other countries.9,31 Figure 1 shows distribution and overlapping of HGs and IGD+ subjects among gamers. In the χ2 test, both HG and IGD+ scores were significantly associated with the male sex as well as online and MMORPG gaming. However, as far as psychosocial status and adjustment were concerned, Student's T test showed that IGD+ subjects had significantly worse (i.e., higher) scores than IGD−, both in global and three of the five subscales (self-esteem and prosocial behavior being borderline significant with p: 0.025 and p: 0.012, respectively) (Table 4). Conversely, HGs did not significantly differ from CGs globally or in any of the five subscales.
ES measure is shown in significant differences between brackets [Cohen's D].
CGs, casual gamers; HG, heavy gamers; IGD+, subjects scoring 5 or higher in the IGD-9 scale; IGD−, subjects scoring 4 or less in the IGD-9 scale; p, level of significance.
The multivariate analysis (logistic regression) showed that IGD+ scores were significantly associated with worse psychosocial health and adjustment (p < 0.001), while the other variables (male sex, online and MMORPG gaming, and HG) were not significantly associated (p > 0.01) (Table 5). The odds ratio for psychosocial health was 1.05 (99% confidence interval: 1.028–1.081); this means that for every point of worsening in psychosocial scale scores, there is a 5 percent increase in the likelihood of being IGD+ (Table 6).
R2: Cox–Snell = 0.108, Nagelkerke = 0.211.
Confidence intervals for main variables.
Discussion
IGD is included in DSM-5 as a condition worthy of future study, and gaming disorder has been proposed to be included in the ICD-11. 2 Suspected PVG in children and adolescents is a concern for parents and carers and it is becoming a frequent reason for referral to clinical psychologists. Therapists need to handle this problem with appropriate instruments and evidence-based knowledge.
This study of Spanish adolescents adds to the growing body of international data on IGD, indicated as necessary by the inclusion of IGD in the appendix of the DSM-5. We aimed to study gaming features and to estimate PVG prevalence. We also aimed to assess whether, as studies in other countries suggest, subjects fulfilling DSM-5 IGD criteria have poorer psychosocial health and adjustment and are therefore candidates for a clinical intervention. In addition, an association between IGD+ scores and potential risk factors for PVG was investigated. As for methodology, the sample was close in size to similar studies (774 in the Spanish sample of a multicenter study). 32 It was extracted from multiple centers, and different age groups and socioeconomical statuses were appropriately represented, all of which strengthen the validity of our results. We followed expert guidelines regarding scale and variable selection and also to help with generalization of our findings. 24
The prevalence of IGD was 8.3 percent of our sample of 708 Spanish adolescents. Only two studies had previously addressed IGD frequency in Spain, with contradictory results of 0.4 and 7.7 percent,32,33 our result being closer to the latter study. Scale selection may be responsible for the observed differences as none of the previous studies used DSM-5 IGD criterion-based scales. We believe these criteria are useful from a practical perspective as they are similar to the questions a psychologist would pose in a clinical setting. However, and although DSM-5 IGD criteria have good sensibility, they lack the specificity of a full clinical interview, and thus the possibility of overestimation of the disorder cannot be ruled out. Categorical instead of dimensional criteria may compromise reliability in this regard.
Male students reported significantly longer periods of gaming (both daily hours and days of the week) and engaged significantly more in online VG and MMORPGs than female students. This fits with most other studies. 6 Males fulfilled HG criteria in a much higher proportion (35 and 6 percent, respectively). More importantly, IGD+ incidence was significantly higher (nearly 13 percent vs. 2.5 percent), in line with previous reports by Gentile et al. and van Rooij et al., which showed results of 12 percent versus 4.6 percent and 5 percent versus 1 percent, respectively.6,10 However, in the multivariate analysis, association among IGD+ scores and male sex did not remain significant after controlling for psychosocial health. Differences observed between sexes are likely to reflect the higher use of VG in male students, rather than a true sex effect.
Online gaming and MMORPG gaming were significantly more frequent in IGD+ subjects, as other authors have previously noted. 34 Certainly, the Internet has had a huge impact in VG, making possible the transition from a human–computer interaction, as described in technological addictions, to a more complex, appealing, and potentially addictive human–computer–human interaction. 1 Online gaming offers a set of rules, aims, and contexts to the human interaction, making it more attractive and may satisfy subject's need for socialization. This revolutionary phenomenon might be responsible for the apparent increase of PVG in recent years. However, according to the multivariate analysis, these gaming features were not significantly associated with IGD+ scores or poor psychosocial health. This suggests that they may simply reflect more frequent gaming patterns and not be risky per se.
Similarly, gaming time, while commonly alarming for parents and carers, has a controversial association with PVG. As mentioned previously, there is no consensus definition of excessive gaming time, and medical association recommendations (as American Pediatric Association) of screen time are purely empirical. 35 Experts consider daily hours more useful than weekly days spent on gaming. 17 Our definition of HGs (≥10 hours weekly and/or binge gaming of ≥5 hours) takes into account these reports and also our clinical experience with suspected PVG patients. Most references analyze raw gaming time without considering gaming time pattern in a continuous manner. This approach would not detect many binge gamers (1 hour a day five days a week would be equal to 5 consecutive hours once a week), misclassifying them as light gamers. Our definition was designed to make sure that the binge gamer pattern was appropriately detected. This way of classifying HGs has made it possible to isolate a remarkable gaming pattern so far unreported. Interestingly, in our sample, HGs had a similar psychosocial health and adjustment as CGs, and gaming time was not significantly associated with IGD+ scores. Since our study is transversal, we cannot exclude gaming time as a risk factor for PVG, but our findings are in agreement with other authors who point at a nonadaptive gaming pattern (and not gaming time) as the main risk factor for PVG.8,9,17 In our sample, we confirmed a profile of a healthy gamer without negative psychosocial consequences despite the time devoted to gaming, as other authors had suggested. It is important to underscore that this gaming pattern, which may seem superficially alarming for parents and psychologists, may not be intrinsically negative, although more data are needed to confirm this hypothesis.
Finally, we found consistent results as far as psychosocial health was concerned. Both global scores and satisfaction with life, physical aggression, and loneliness subscales were significantly associated with IGD+ scores in the univariate analysis. Other authors found similar findings using different scales, in some cases more complex (13-item gaming scale and 112-item psychosocial scale in Müller's study), in others extremely brief (two psychosocial questions in López-Fernández's study).32,33 We chose to follow Lemmens's work to use a scale based on the DSM-5, including all symptoms while being concise, to find a reliable screening instrument for a Spanish population in nonclinical settings. 24 It is a remarkable strength of the IGD-9 to be able to detect psychosocial disturbances without overtly inquiring about them only with gaming-related dichotomous questions. We cannot elucidate whether PVG as diagnosed by IGD criteria is a neatly defined disorder or the tip of the iceberg of a deeper psychosocial process, but our study underscores the usefulness of this scale to screen for child and adolescent dysfunction related to gaming.
Our study has certain limitations. First, being a transversal study, we cannot establish the causal nature of the observed associations, and long followup studies are warranted to confirm our findings. Sample size was estimated solely on the basis of previous references (minimum around 700 subjects). This might have limited the potency of out study (increasing type II error probability), although the detection of highly significant findings argues against this. A strength of our study is the multicenter sampling that includes different socioeconomic groups. Nonetheless, a larger sample, including different cities, would be more representative to establish the true prevalence and nature of PVG in Spain. Finally, self-administered questionnaires may be susceptible to memory and social desirability bias, although the latter may be compensated by anonymity. Subjectively reported gaming time may be inaccurate, probably tending to underestimation.
Despite these limitations, our sample was a representative sample of Spanish urban students. We ascertained a substantial frequency of HGs (over 20 percent) and subjects fulfilling DSM-5 IGD criteria (up to 13 percent of male students), the latter yielding poor psychosocial health in a set of complete and functionally relevant scales. Our statistical analysis was able to control for potential confounders and showed that problematic gaming was the only variable consistently linked to psychosocial problems. While awaiting a formal definition, the phenomenon of PVG needs to be acknowledged by psychologists, school counselors, and parents as a proportion of these subjects may require further clinical approach. In addition, the observation of a well-defined subgroup of HGs without negative psychosocial consequences advises against raising unnecessary alarm as children and adolescents most frequently enjoy VG in a healthy manner.
Footnotes
Acknowledgments
The authors wish to thank all the students and school counselors for their critical help and assistance to collect all the relevant data and information. The study was not privately or publicly funded.
Author Disclosure Statement
No competing financial interests exist.