
Abstract
Abstract
This study aimed to investigate the effectiveness of the mobile game-based neuromuscular electrical stimulation (MG-NMES) with assessing usability issues, such as attention and curiosity, and intrinsically interesting issues, which is necessary for successful poststroke rehabilitation. With the conventional NMES (C-NMES) system, the subjects underwent active repetitive cyclic NMES training. For assessment of usability issues, 20 hemiplegic stroke subjects were randomly divided into two groups. The subjects in the MG-NMES group (n = 9) and C-NMES group (n = 11) underwent 20 minutes of training each day for 5 days. We assessed the subjects' attention, curiosity, and intrinsically interesting issues; and using questionnaires they answered questions regarding their expectations of the training outcome after each training session. We found that the subjects in the MG-NMES group maintained their attention and interest for the 5 days, and their curiosity and expectation of a positive training outcome gradually increased as the training proceeded. In contrast, the C-NMES group reported no change in their attention or curiosity, but it was lower than the subjects in the MG-NMES group. In addition, their interest gradually decreased, which may have reduced their expectations of a positive outcome as the sessions progressed. There were no side effects during the training sessions in either group. The MG-NMES training paradigm developed is a new, readily available, and highly motivating MG-NMES training system. Based on the usability test, the reported advantages of the system were improved attention and flow experience during NMES training.
Introduction
F
Research has shown that neuromuscular electrical stimulation (NMES) can enhance motor relearning following damage to the central nervous system. 3 NMES applied to the muscles that drive movement improve the range of joint motion and induced volitional muscle contraction, even in severely impaired limbs of stroke patients. 4 It produced better results when applied during the acute phase of a stroke; however, it also promoted further recovery of motor impairment, even in the chronic stage of stroke patients. 5 NMES has been used in various neurological diseases, for example after a stroke,6,7 spinal cord injury,8,9 and cerebral palsy.10,11 In the field of stroke rehabilitation, a variety of therapeutic NMES, including cyclic electrical stimulation (ES), electromyography triggered ES, and functional ES have been used to facilitate the voluntary movements, improve manual dexterity and activities of daily living,12,13 arm function recovery, reduction of shoulder pain, 14 and improvement in walking ability. 15
A combination of NMES and other therapeutic interventions is useful. NMES is more effective when it is used in conjunction with other motor training, such as exercise therapy or robot-assisted training. 16 In particular, NMES with augmented voluntary activation increases neural plasticity; however, neither NMES nor voluntary movement alone had such an effect. 17 Due to the repetitiveness and monotony of NMES training, it can become “boring” and tedious very quickly in the rehabilitation setting; therefore, making exercise augmented NMES training fun and interactive is an important aspect to consider.
To overcome the boring and encourage voluntary movements, virtual reality (VR) or game technology could be one of the solutions. VR game-based training with motion controller has been widely applied in rehabilitation18–20 particularly after stroke.19,21,22 By providing well-designed attractive training environment, VR game has various advantages in rehabilitation that it augments user's engagement and motivation to participate attentively so that its compliance would be increased and positive outcomes could be expected as a result18,23; it could be easily accessible for home rehabilitation based on mobile application. 24 In addition, VR game with motion controller could give real-time motion feedback to interact with virtual environments and the feedback could give additional cue for their movements or motor planning to facilitate neural plasticity after stroke. 25 However, there are few studies and insufficient evidence that aim to evaluate the level of participation issue in VR game-based rehabilitation therapy after stroke. 26
With this in mind, we developed a mobile game-based NMES (MG-NMES) application. Relative to conventional rehabilitation training, a mobile game rehabilitation system has many advantages; it is easy to carry, it increases the dose of conventional training, and it can be used effectively in home-based rehabilitation and tele-rehabilitation. Most importantly, it may also increase the motivation of patients, and serve as a pleasurable experience during treatment by providing various feedback mechanisms and goal-directed tasks. In this study, we evaluated an MG-NMES training paradigm by assessing whether it is more fun compared with the conventional NMES (C-NMES), and we propose the possibility of using MG-NMES in clinical practice.
Methods
System description
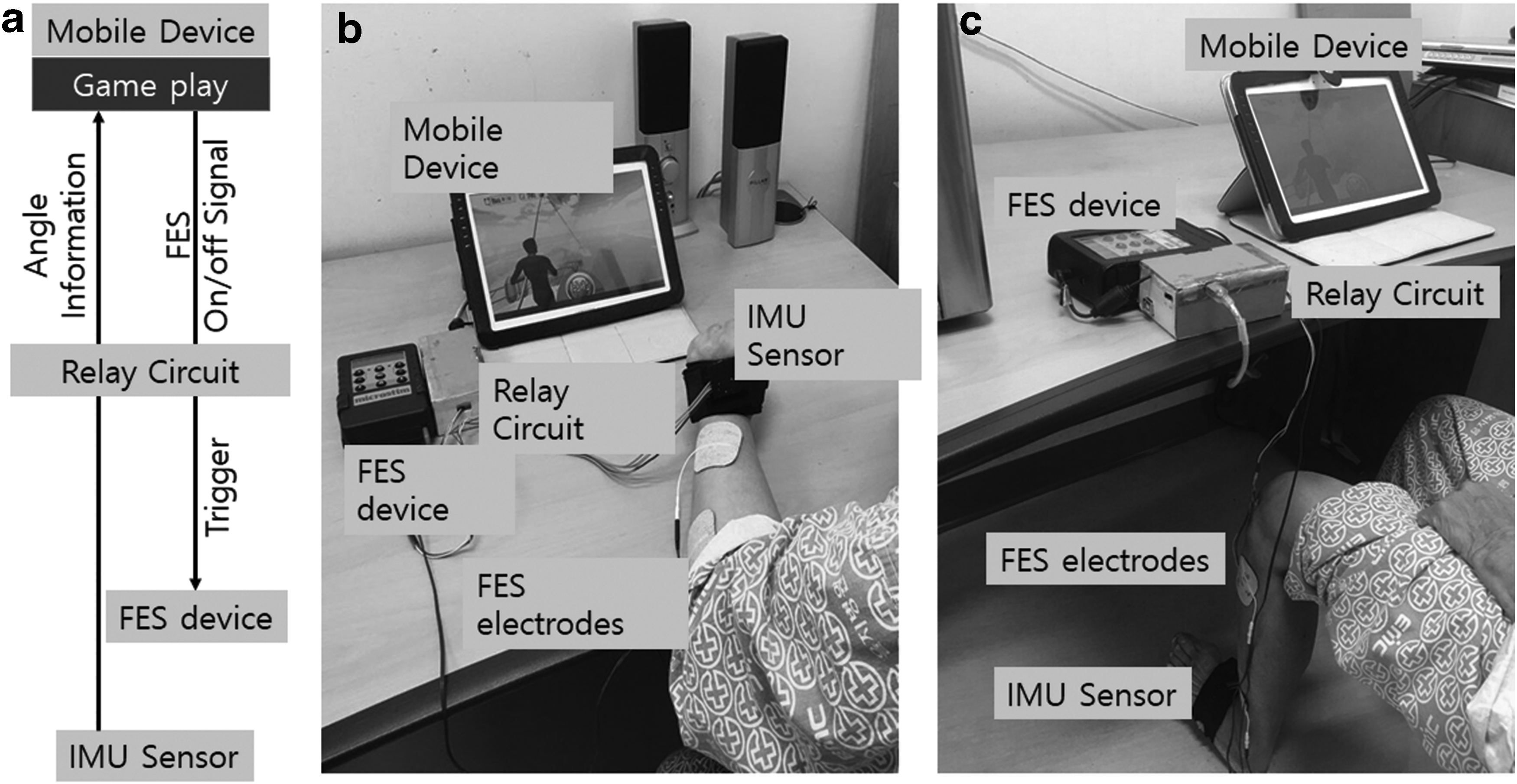
The MG-NMES system is composed of a mobile device, circuit box, control box, motion sensor, NMES device, and an electrical pad (Fig. 1). Game play commences on the mobile device (Galaxy Tab® SHW-M480W; Samsung Electronics, Korea) according to the hand angle of the user, received from the circuit box, and gives a command to trigger the NMES stimuli through the device (Microstim®; Medel GmbH, Inc., Hamburg, Germany).
Content design of the MG-NMES
The game was designed to encourage a patient's movements according to the game play, so that the user would be motivated to participate in the game play by moving of his/her wrist or ankle to a specific target. The game adopted was a fishing game with the goal of catching a fish because the explicit exercise timing and congruent movement could be important in the exercise game. In this point of view, we designed a fishing game in which a fish should be pulled up by extending the user's wrist (or ankle) to a specific angle (congruent movements) when it was caught in a fishing needle (exercise timing cue).
The first step involved the user placing his/her own hand (or foot), with the sensor, in front of the mobile device, comfortably. The mobile device displayed the fishing game, and as a fish approaches, the user prepares to extend his/her wrist joint (or dorsiflex the ankle). When the fish bites in the game, the user should try to extend his/her limb. When the initial movement of the wrist or ankle is detected by the sensor, an NMES is generated, similar to positional feedback stimulation, which is effective for facilitating targeted muscle contraction in stroke patients.27,28 In cases where there was no movement detected in the initial predefined time an NMES also assisted the target muscle contraction.
If the user's wrist extension/ankle dorsiflexion angle reached over the predefined angle, the fish would be pulled up and caught if the limb was extended and maintained at the angle for a specific amount of time. The angle and time were adjusted to the severity of the user; however, in the cases where patients had difficulty extending their limb to the predefined minimum angle, the NMES operation mode could be set. In this mode, the user could receive an NMES stimulus when s/he extended their wrist (or dorsiflexed their ankle) to the minimum NMES angle (e.g., 5°–20°), so that s/he could play the game with the assistance of the NMES. If, when being assisted by the NMES stimulus, the wrist extension (or ankle dorsiflexion) angle goes over the predefined angle, the NMES stimulus would be OFF to prevent excessive stimulus when the angle exceeded the maximum, usually set to about 20 percent of the predefined angle (e.g., 50°). If the extended angle was smaller than the predefined angle (40°), the NMES stimulus would be delivered. In this manner, the NMES stimulus was either ON or OFF, and the user could be assisted until the fish was caught.
Subjects
Twenty-three sub-acute to chronic hemiplegic stroke subjects were recruited to the study. All patients were selected from inpatient and outpatient rehabilitation services at Eulji Hospital, Seoul, Korea. We recruited patients who had suffered their first stroke, were diagnosed by MRI or computed tomography scans, had mild to severe hemiparesis of the contralesional wrist extensor or ankle dorsiflexor, and had no limb injuries or deformities. All subjects were medically stable and able to sit upright throughout the procedure. The exclusion criteria for this study were as follows: (1) insensate affected limb; (2) cardiac arrhythmia with hemodynamic instability; (3) severe depression, apraxia, and/or cognitive deficits with a score <24 on the Mini-Mental State Examination (MMSE 29 ); (4) any precautionary state for NMES, such as poor skin condition, uncontrolled epilepsy, and subjects with active medial implants. All patients who consented to participate in this study were informed about NMES and the procedure, which was approved by the Institutional Review Board of Eulji Hospital, Seoul, Korea (2017-10-001).
Procedure
Twenty-three stroke subjects were divided randomly into two groups; MG-NMES and C-NMES. Randomization was performed using the order of entry into the study and a computerized research randomizer. Three subjects were excluded because their MMSE score was <24. Finally, nine participants received the MG-NMES training, and 11 participants received the C-NMES training daily (20 minutes duration each) for 5 days.
All subjects were first provided with the instructions regarding the experiment, providing information about the experiment, the purpose of the study, and the data protection policy. NMES were administered by one physical therapist, who had more than 10 years of experience administered ES. He attached the electrical pad on target muscle and adjusted the stimulation intensity according to individual motor abilities and monitored participation and safety issues during both training. They were positioned sitting in front of a table with their affected limb on the table. During the training sessions, the same electrical pad (50 × 50 mm) was attached to the target muscle (wrist extensor muscle or ankle dorsiflexors of the affected limb) in both groups, and a motion sensor was also attached distal to the wrist or ankle joint in the MG-NMES group (Fig. 1). The angle parameters for MG-NMES ON and OFF during the game, and the intensity of the NMES stimulation were set individually. The subject could then experience the fishing game within the MG-NMES training session, and participants tried to extend and maintain the extension according to the display on the mobile device.
The C-NMES group received sequential repetitive ES stimuli. Biphasic waveforms of electrical current pulses were delivered at a frequency of 35 Hz, pulse rate of 250 μseconds, ON–OFF period of 7/12 seconds, and the intensity (<100 mA) was individually set to a level that would allow a sufficient range of motion of the wrist and ankle. 30 During the C-NMES training, subjects were instructed to relax during the NMES OFF period, and do active voluntary target muscle contraction during the NMES ON period.
Both groups received training for 20 minutes, once a day for five consecutive days. To assess the motivation and active engagement during each training session, we assessed the attention, curiosity, and intrinsically interesting issues using a modified version of the questionnaire from Park and Ryu, 31 (Table 2). Each patient completed a self-report paper and pencil style five-point Likert questionnaire (from 1 Strongly disagree to 5 Strongly Agree) after each session and two items (one in attention and the other in intrinsic interest category) was reverse coded. Statistical analysis was performed using independent sample t-tests and repeated measure analysis of variances (ANOVAs), using SPSS 23.
Results
The demographic data of the two groups showed no significant baseline difference in age, gender, side of hemiplegia, duration after stroke onset, MMSE score, MRC grade, or modified Ashorth scale of applied muscle and modified Barthel score (Table 1). The causes of stroke were infarction in seven patients and hemorrhage in two patients in the MG-NMES group. In the C-NMES group, infarction in six patients and hemorrhage in five patients.
C-NMES, conventional neuromuscular electrical stimulation; MAS, Modified Ashworth scale; MBI, modified Barthel index; MG-NMES, mobile game-based neuromuscular electrical stimulation; MMSE, Mini-Mental State Examination; MRC, Medical Research Council.
The usability issues in the MG-NMES group and C-NMES group showed significant differences when the mean values for the 5 days in each category were compared; the MG-NMES group reported significantly higher ratings of attention (t = 2.517, p = 0.022), curiosity (t = 2.164, p = 0.044), and interest issues (t = 2.339, p = 0.031) compared with the NMES only group while there were no significant differences in subjective expectation of the training outcomes of functional enhancement (t = 0.978, p = 0.341) and beneficial effect (t = 0.643, p = 0.528) (Table 2).
Represented the reverse coded items; mean and standard deviation for 5 days were presented for each group and category. Attention, curiosity, and intrinsic interest items were adopted from the flow questionnaire. 31
We found that the MG-NMES group maintained their attention better in the first four days (t = 2.187, p = 0.042, choen's d = 0.99 for day 1; t = 3.023, p = 0.007, choen's d = 1.37 for day 2; t = 2.099, p = 0.050, choen's d = 0.95 for day 3; t = 2.550, p = 0.020, choen's d = 1.16 for day 4). We found that MG-NMES group maintained their interest as the training proceeded but the C-NMES group decreased to make significant differences in the fourth and fifth days (t = 2.377, p = 0.029, choen's d = 1.08 for day 4 and t = 2.954, p = 0.010, choen's d = 1.28 for day 5). Their curiosity and positive expectations of the training outcome gradually increased as the training proceeded in MG-NMES group and ended up with the significant differences between two groups (Fig. 2). MG-NMES group reported better maintenance of their curiosity in day 2 (t = 2.431, p = 0.026, choen's d = 1.12) and day 5 (t = 4.180, p = 0.001, choen's d = 1.192), better expectation of functional enhancement in day 5 (t = 2.358, p = 0.032, choen's d = 1.03), and better expectation of beneficial effect in day 5 (t = 2.396, p = 0.028, choen's d = 1.10) compared with C-NMES group.
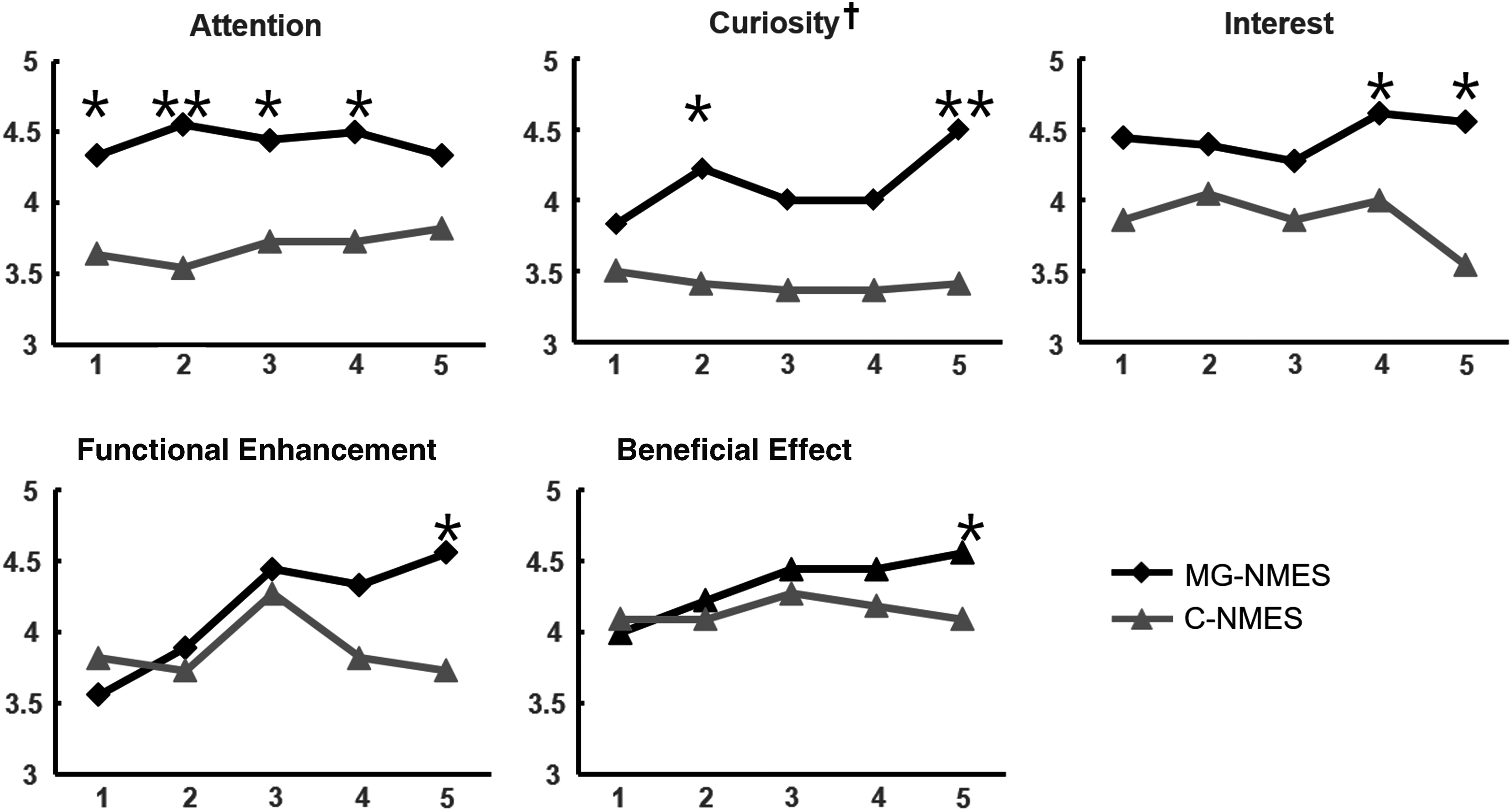
The subjective score changes in each category for attention, curiosity, interest, functional enhancement, and beneficial effect. * and ** represent p < 0.05 and p < 0.01 respectively in the comparison between the MG-NMES and C-NMES groups using an independent t-test. †The curiosity scores showed significant interaction (F = 3.131, p = 0.047) in the repeated measures ANOVA. ANOVA, analysis of variance; NMES, neuromuscular electrical stimulation; C-NMES, conventional neuromuscular electrical stimulation.
In particular, there was a significant interaction effect in curiosity (F = 3.131, p = 0.047), but not in other measures, when analyzed using a repeated measures ANOVA. In contrast, the C-NMES group reported no change in their attention or curiosity, but it was lower than those of the MG-NMES group, and showed a gradual decrease in interest, which may have prevented positive outcome expectations as the sessions progressed (Fig. 2). There were no side effects observed during the training sessions in either group.
Discussion
In this study, we compared game-based NMES and conventional NMES to examine the motivation and active engagement of training, which could influence the outcome of the training. We asked patients who underwent 5 days of training, with one of two types of training paradigm, to answer subjective opinion-based questions in five categories; attention, curiosity, interest, functional enhancement, and beneficial effect.
The results showed that patients who experienced the MG-NMES training reported significantly higher scores to questions asking their opinion regarding attention, curiosity, interest, and functional enhancement in one or more of the 5 days compared with patients in the C-NMES group. The participants' attention was significantly sustained at a higher level in the first 4 days, and curiosity and functional enhancement were increased in the MG-NMES group as the training sessions progressed, whereas the C-NMES group showed consistently lower score across the five sessions. Meanwhile, for the interest parameter, the MG-NMES group kept higher in average than that of C-NMES, while the C-NMES group's interest level had a tendency to decrease as the training sessions progressed, in particular showing a significant difference in the fourth and fifth training session.
Overall trend of the higher attention score could mean that the participants were more attentive during the MG-NMES training, and maintained their attention as sessions progressed. Although the attention level was lower in the C-NMES paradigm, it was also kept low. Considering the participants were randomly assigned and matched, the difference would be from the difference in the paradigm. The MG-NMES training provided a more interactive scheme, whereas the C-NMES training session was noninteractive and passive. In addition, the MG-NMES training provided a visual display synchronous with the subjects' movements. This could also be one of the factors influencing the attention.
The score for interest shows a gradually decreasing pattern in the C-NMES group, whereas that of the MG-NMES group was kept high to become significantly higher by the fifth day. When considering interest, the motives, exploration, and learning 32 are needed for the person's engagement in the environment. The MG-NMES training sessions might positively influence in keeping the participants motivated and engaged with plenty of motor learning during the training sessions, whereas the C-NMES training failed to motivate them as the sessions progressed. The C-NMES training became more boring as the sessions progressed because they were repetitive, and passive stimuli were provided without any variation or interaction, so the motor learning effect became diminished. However, the MG-NMES training prevented the participants from becoming bored, which may be because it provided various stimuli that varied according to the movements evoked by the NMES stimuli or voluntary intention.
In contrast, other scores for curiosity, functional enhancement, and beneficial effect, showed a gradual increase for the MG-NMES group, whereas for the C-NMES group, the score remained low as the sessions progressed. Curiosity refers to the desire to know, see, or experience that motivates exploratory behavior directed towards the acquisition of new information. 33 These results could suggest that the MG-NMES paradigm led the participants' desire to obtain stronger motor ability, meaning the increased desire could affect the participants' expectations of their functional enhancement and beneficial effect. It is also associated with the approach to behavior and experiences of reward. Therefore, the results of the MG-NMES training was as expected, with improvement seen in the participants' rehabilitation, and positive effects on their motor learning being observed. These positive effects should encourage the participants to use the system again.
A previous study reported more positive results when ES was triggered by voluntary stimulation compared with passive ES alone. 34 In this study, all subjects were instructed to actively contract the target muscles during ES during MG-NMES or C-NMES training. Therefore, the difference in scores was not the result of voluntary activation of the muscle itself.
As far as we know there are a few trials that combine position feedback NMES and mobile game application 35 although VR application in rehabilitation field has been widely used.18–20 One of representative advantages of VR is that it could give cue information that is hard to be perceived and feedback regarding the movements. 25 It could sustainably capture user's attention during the whole period of playing the game. In addition, mobile paradigm in rehabilitation could have potential to be easily accessible in rehabilitation. 24 Likewise, the position feedback NMES paradigm is effective in that it could capture the user's intention, and assist him/her to move according to his/her intention, which could facilitate their training. In addition, NMES combined with a game, as suggested in this study, could provide an additional effective paradigm to facilitate their motor mechanism by capturing their attention and interest even further during their training.
However, there are some limitations in our study. First of all, we measure the outcomes in a subjective manner with a questionnaire, so the patients' daily conditions could influence the results. In addition, relatively small sample size also makes it hard to lead to secure conclusion. We could not design this study as a cross over study, which refers to a study in which the same participant receives both trainings but at different times so that outcomes would be examined and it might have shown the differences more clearly. However, we believed that because some of the subjects to be in the stage of sub-acute recovery, the results could be affected if the training period was longer (e.g., more than 5 days).
These results suggest that the MG-NMES paradigm could keep a patient's interest as time progresses, which leads to increased curiosity, sustained attention, and positive expectations regarding training outcomes. It may improve the participant's active engagement and increase the “dose” of training, which could result in positive motor learning outcome. Therefore, we conclude that the MG-NMES paradigm could be an effective tool for the rehabilitation of stroke patients.
Footnotes
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (No. NRF-2017R1A2B4011920).
Author Disclosure Statement
No competing financial interests exist.