
Abstract
Abstract
We evaluated the effect of dichoptic visual training based on a unique virtual reality (VR) platform mounted display in patients with intermittent exotropia (IXT). A total of 25 IXT patients (8 men, 17 women) with a mean age of 12.3 years (range, 5–39 year) were recruited. The Hirschberg test, prism and alternate cover testing (with accommodative targets for fixation at 33 cm in all patients), perceptual eye position (PEP), and stereopsis were evaluated after 1, 3, and 6 months of dichoptic visual neuroplasticity training with a computer-controlled perceptual examination evaluation system. Data collected before and after training were evaluated using SPSS software. After 6 months of perceptual training, a new order stereopsis was established, and eye positions were improved in all 25 patients. After training for 1 and 6 months, the horizontal PEP pixels were much lower than those pretraining, respectively (Δ1-0 = −0.53, p = 0.028; Δ6-0 = −0.80, p = 0.018). There was no statistically significant difference between pretraining and 3 months after training in horizontal PEP (Δ3-0 = −0.29, p = 0.370). There was no significant difference between pretraining and post-training in vertical PEP (p > 0.05). There were significant differences between pretraining and post-training in the cornea's optical reflection and prism diopters (p < 0.01). Dichoptic visual neuroplasticity training based on a VR platform is an effective nonsurgical treatment in patients with IXT. With the VR treatment, the degree of strabismus and stereopsis was improved in IXT patients. Perceptual training with VR can remove obstacles in the visual processing channel and repair defects in visual function. The clinical manifestations of improvement were the decrease in the degree of strabismus and the re-establishment of stereopsis.
Introduction
I
Zero-order stereoscopic functional examination (titmus, random point examination, and synoptophore) is widely used in clinical practice but is unable to measure the residual stereoscopic function that is often under threshold, including first-order and second-order stereopsis. Accuracy is important, since the result of the examination will determine the selection of the therapeutic regimen, including rehabilitation and rebuilding of binocular vision. Hess et al. demonstrated that the function of binocular vision in strabismus patients was normal, but the corresponding visual cortex function of the weak eye (strabismus eye) was inhibited by the dominant eye. 7 Binocular function can be restored through disinhibition therapy.
In this study, an intelligent platform of the visual perception model based on virtual reality (VR) technology was applied to detect binocular visual impairment in IXT patients. We have conducted a study on the effect of dichoptic visual neuroplasticity training based on a VR platform in a sample of IXT patients to evaluate the potential success of this therapy.
Patients and Methods
Patients
A total of 25 IXT patients (8 men, 17 women) with a mean age of 12.3 years (range 5–39 years) were recruited in this study. Inclusion criteria were patients with IXT, age 5 years old or more, and willing to perform the visual perceptual training. Patients with constant X(T), or significant coexisting ocular abnormality, such as cataract, or previous surgical history were excluded. Patients were not enrolled if they were unable to understand and follow the procedures of the visual perceptual training. All patients or their guardians have completed written informed consent before inclusion in the study. All study protocols were approved by the Ethics Committee of Guangdong General Hospital and carried out in adherence to the Declaration of Helsinki regarding ethical principles for research involving human subjects.
Measurements before training
For all patients, a detailed ophthalmic examination was conducted, including visual testing, manifest and cycloplegic refraction, cornea's optical reflection (Hirschberg test), prism diopters, anterior segment examination with the slit lamp, fundoscopy, ocular movement, and a visual perceptual examination.
The devices used to measure the visual and perceptual examination included: Windows 7 system PC host, LG2342p polarized three-dimensional (3D) monitor with a resolution power of 1920 × 1080 and refresh frequency of 120 Hz, and 3D polarized glasses. A visual and perceptual examination evaluation system invented by the National Engineering Research Center for Healthcare Devices was used. MATLAB was used to generate the stimulating template.
All examinations were carried out in a room with bright ambient lighting. All patients wore their spectacle corrections and 3D polarized glasses to perform the test. Stimuli/patterns were presented on a 3D monitor, which was positioned with the center of the screen aligned horizontally and vertically with the patient's eyes. Viewing distance was 80 cm.
Measurement of zero-order stereopsis
Patients viewed a central optotype (3° × 3°), “E,” which was made up of random dots with different disparity, such as 400′′, 300′′, 200′′, and 100′′. Patients wearing 3D polarized glasses were instructed to state the direction of the “E” and pressed the arrow keys of the keyboard to determine the position. As long as a patient can see any image, he/she has a zero-order stereopsis, and the result was recorded as “1,” or otherwise “0” (Fig. 1).
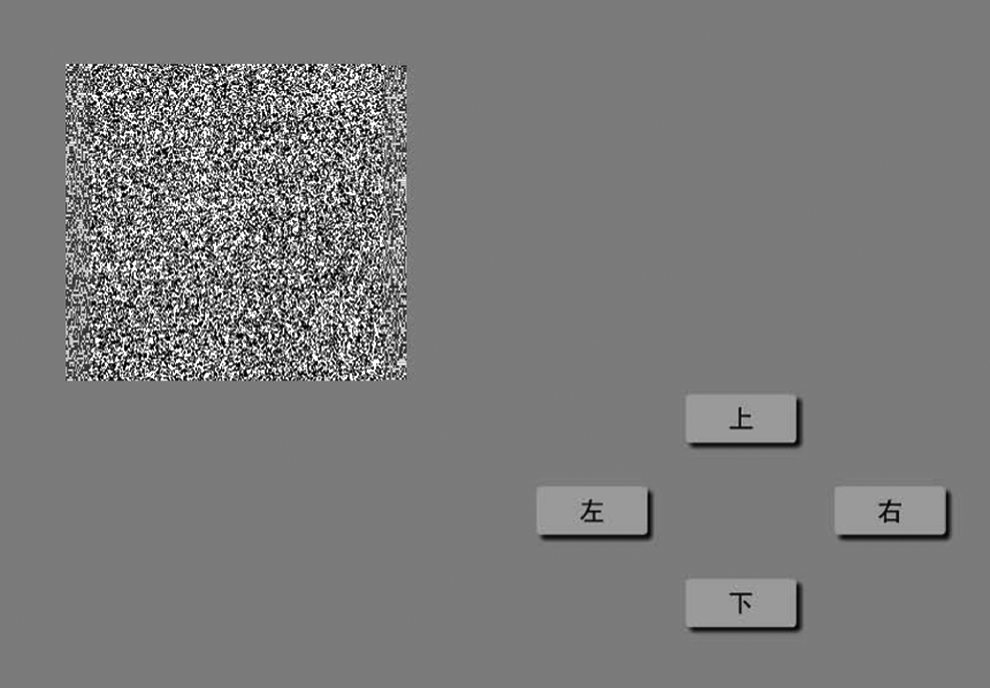
Measurement of zero-order stereopsis. Patients wearing 3D polarized glasses were asked to look at an optotype “E” on one monitor and used the arrow keys to record their directions. As long as patients can see any picture, he/she has a zero-order stereopsis, and the result record was “1,” otherwise “0.” 3D, three-dimensional.
Measurement of first-order stereopsis
Patients viewed a central optotype (6° × 6°), “E,” which was made up of random dots with 800′′ disparity. The “E” was modified in different frequencies and different disparities (50′′–600′′/ms, t = 1.2 seconds) by the experimenter using a keypad. The density and size of dynamic random dots remained unchanged. Patients wearing 3D polarized glasses were instructed to state the direction of the “E” and pressed the arrow keys of the keyboard to match their answer. The accuracy should be 100 percent to pass, which was recorded as “1,” any errors were recorded as “0” (Fig. 2).
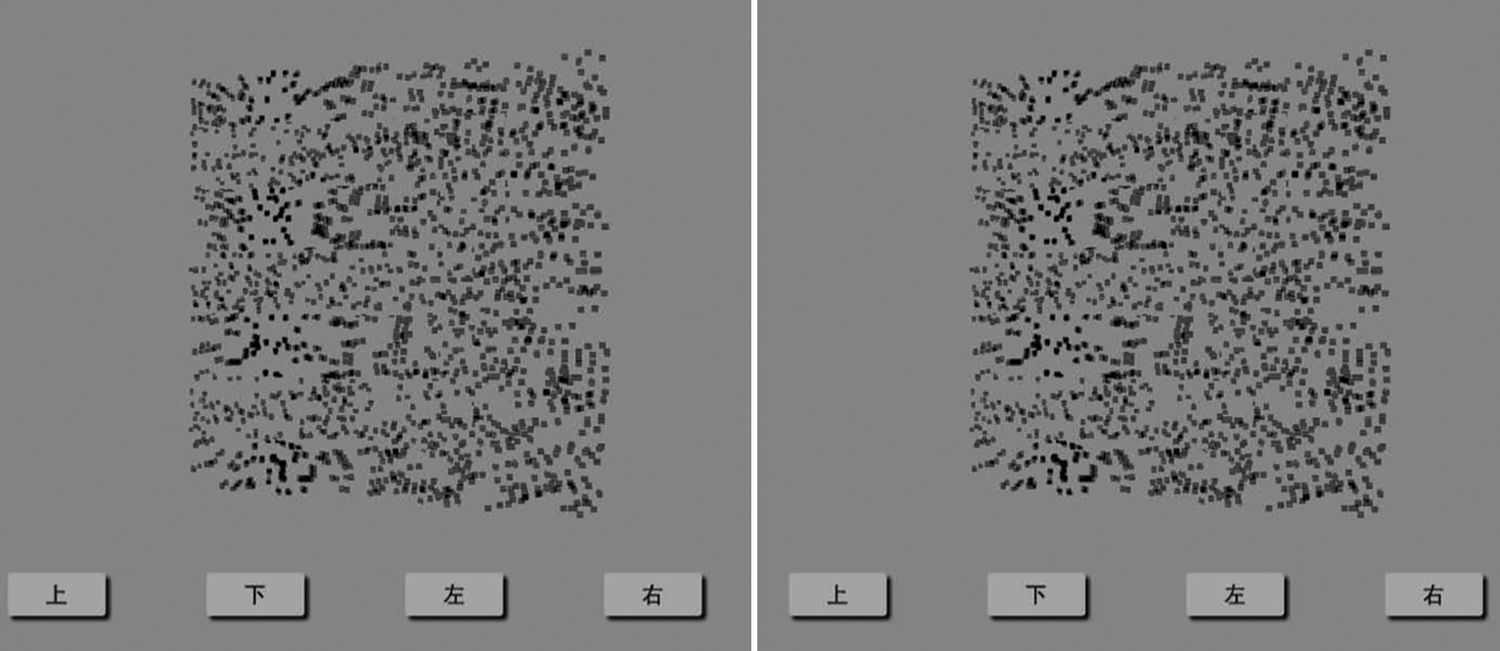
Measurement of first-order stereopsis. Patients wearing 3D polarized glasses were asked to look at an optotype “E” on one monitor and used the arrow keys to record their directions. The accuracy should be 100 percent if pass, and the result record was “1,” otherwise “0.”
Measurement of second-order stereopsis
Patients viewed gray random dot stereograms (44 candela/square meter, 44 cd/m2) presented on the monitor with the mean luminance of 34 cd/m2. The size of each dot was 0.018° × 0.018°. The maximum uncrossed disparity and the maximum crossed disparity were 1800′′. The minimum was 0. The relative disparity of the random points from top to bottom followed a sinusoidal variation. Patients wearing 3D polarized glasses were instructed to state the convexity (crest) or concavity (trough) of random dot stereograms, and to press the arrow keys of the keyboard. If the accuracy was 100 percent, the result was recorded as “1,” any errors were recorded as “0” (Fig. 3).
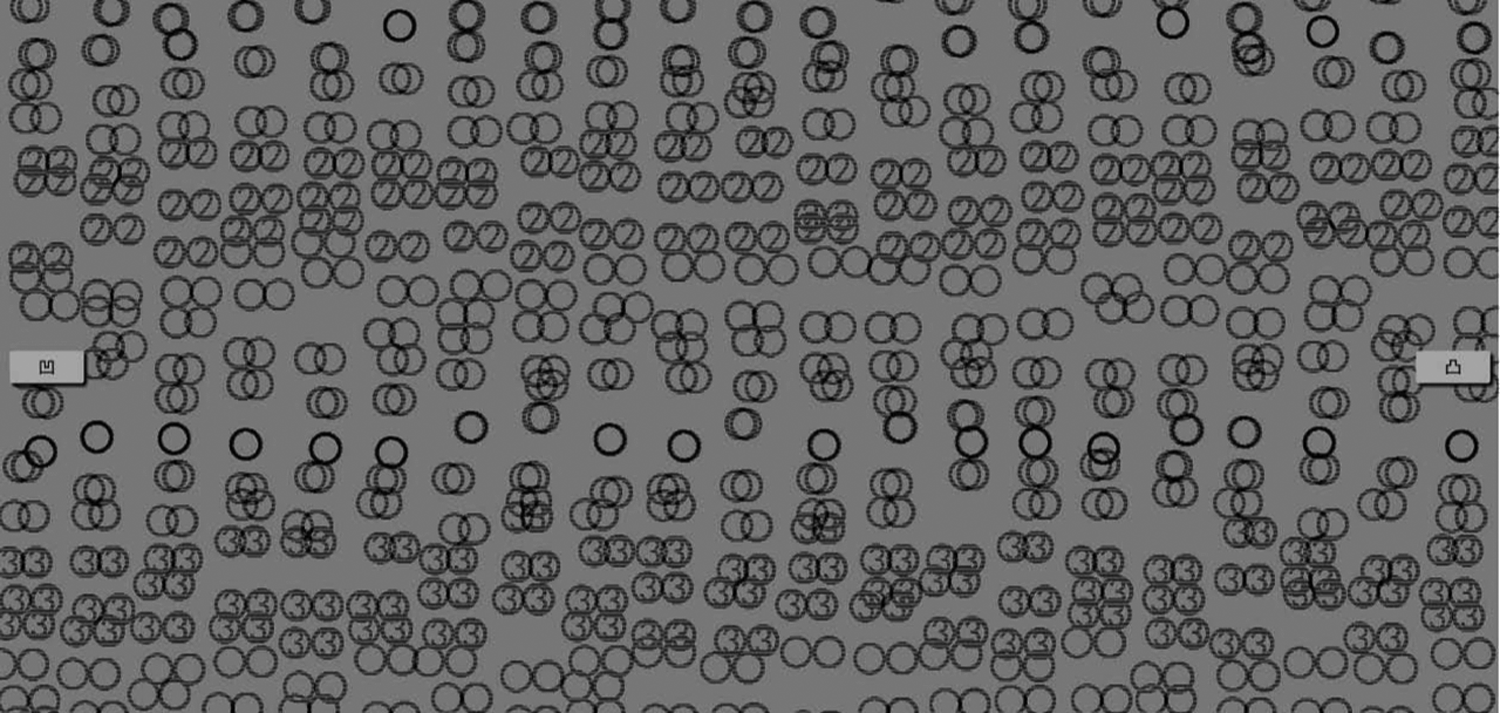
Measurement of second-order stereopsis. Patients wearing 3D polarized glasses were instructed to state the convexity (crest) or concavity (trough) of random dot stereograms and used the arrow keys to record their directions. The accuracy should be 100 percent if pass, and the result record was “1,” otherwise “0.”
Measurement of perceptual eye position
The perceptual eye position (PEP) was measured by the cross-into-circle test, which allowed the left eye to view a cross and the right eye to view a circle (Fig. 4).
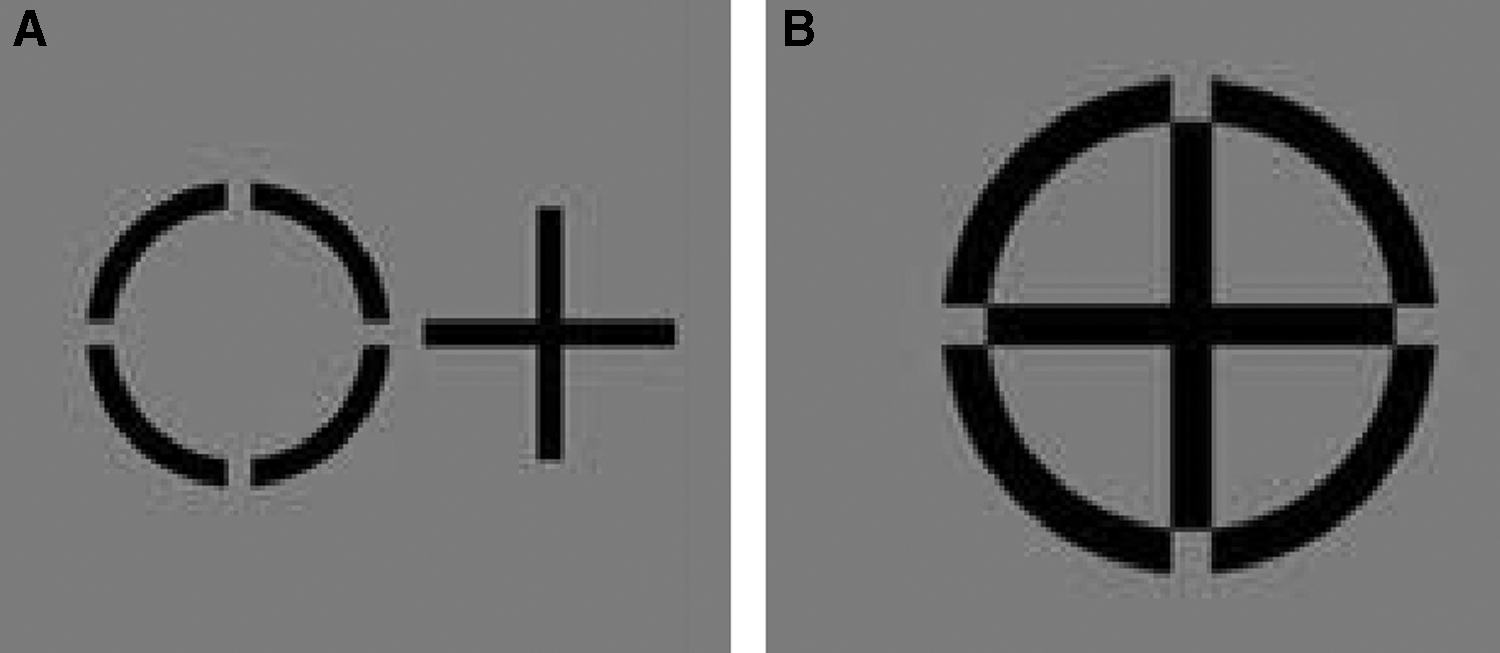
Measurement of PEP. Patients wearing 3D polarized glasses should see a cross in their left eye and a circle in their right eye
The midpoint of the monitor was kept at 80 cm, the same height as the patients' eyes, with the average light source of 80 cd/m2 in white, attenuating to 50 cd/m2 when wearing 3D polarized glasses, and 30 cd/m2 in black, attenuating to 3 cd/m2 when wearing 3D polarized glasses. The stimulating template was 51 × 29 cm in size and 38° × 18°in visual angle. The size of the circle was 0.4° × 0.4°, whereas the size of the cross was 0.33° × 0.33° (1°fixation test object). Patients used a computer mouse to place the cross within what they perceived to be the circle's center and were then instructed to click the mouse. The system automatically recorded vertical and horizontal bias by the 360° test object to observe any ocular misalignment.
All examinations were performed under the best corrected visual acuity. Each examination was repeated three times.
Measurements after training
Patients visited the clinic at 1, 3, and 6 months after training started. At each visit, the cornea's optical reflection (Hirschberg test), prism diopters, stereopsis, and PEP were recorded.
Statistical analysis
Statistical analysis was performed using SPSS Statistics for Windows (ver. 20.0.; IBM Corp., Armonk, NY). p Value <0.05 was considered to be a statistically significant difference. Comparisons among the data that had been logarithmically transformed were made using the mixed linear model.
Results
Demographics of patients
A total of 25 patients of ages from 5 years to 39 years old were enrolled in the study. The mean age was 12.30 ± 8.253 years old. There were 16 children (80.0 percent) and 4 adults (20.0 percent) in this study (Table 1).
Summary Demographics of Patients in the Study
Numbers of patients.
PEP, perceptual eye position.
Comparison of stereopsis before and after training
Twenty-five patients had different levels of stereoscopic examination results, including zero-order stereopsis, first-order stereopsis, and second-order stereopsis. There were five patients (1, 8, 13, 18, and 25) without zero-order stereopsis before training. Patient 1 had no zero-order or first-order stereopsis but had second-order stereopsis. Patient 8 had no stereopsis. Patient 13 and patient 18 both had first-order and second-order stereopsis without zero-order. Patient 25 had first-order stereopsis without zero-order and second-order. After training for 6 months, three patients (1, 13, and 18) had recreated zero-order stereopsis, whereas two patients (8 and 25) did not. Patient 8 and patient 25 who were without zero-order and first-order stereopsis had recreated second-order stereopsis (Table 2).
The Stereoscopic Baseline Characteristics and Results of the Sample of Patients Who Performed the Visual Perceptual Training
Comparison of PEP before and after training
After training for 1 and 6 months, the horizontal PEP pixels were much lower than those pretraining, respectively (1 month: Δ1-0 = −0.53, p = 0.028; 6 months: Δ6-0 = −0.80, p = 0.018). There were no statistically significant difference between before training and after training for 3 months in horizontal PEP (Δ3-0 = −0.29, p = 0.370) (Fig. 5). There was no significant difference between before training and after training for 1, 3, and 6 months, respectively, in vertical PEP (1 month: Δ1-0 = −0.27, p = 0.203; 3 months: Δ3-0 = −0.06, p = 0.832; 6 months: Δ6-0 = −0.48, p = 0.083; p > 0.05) (Fig. 6).
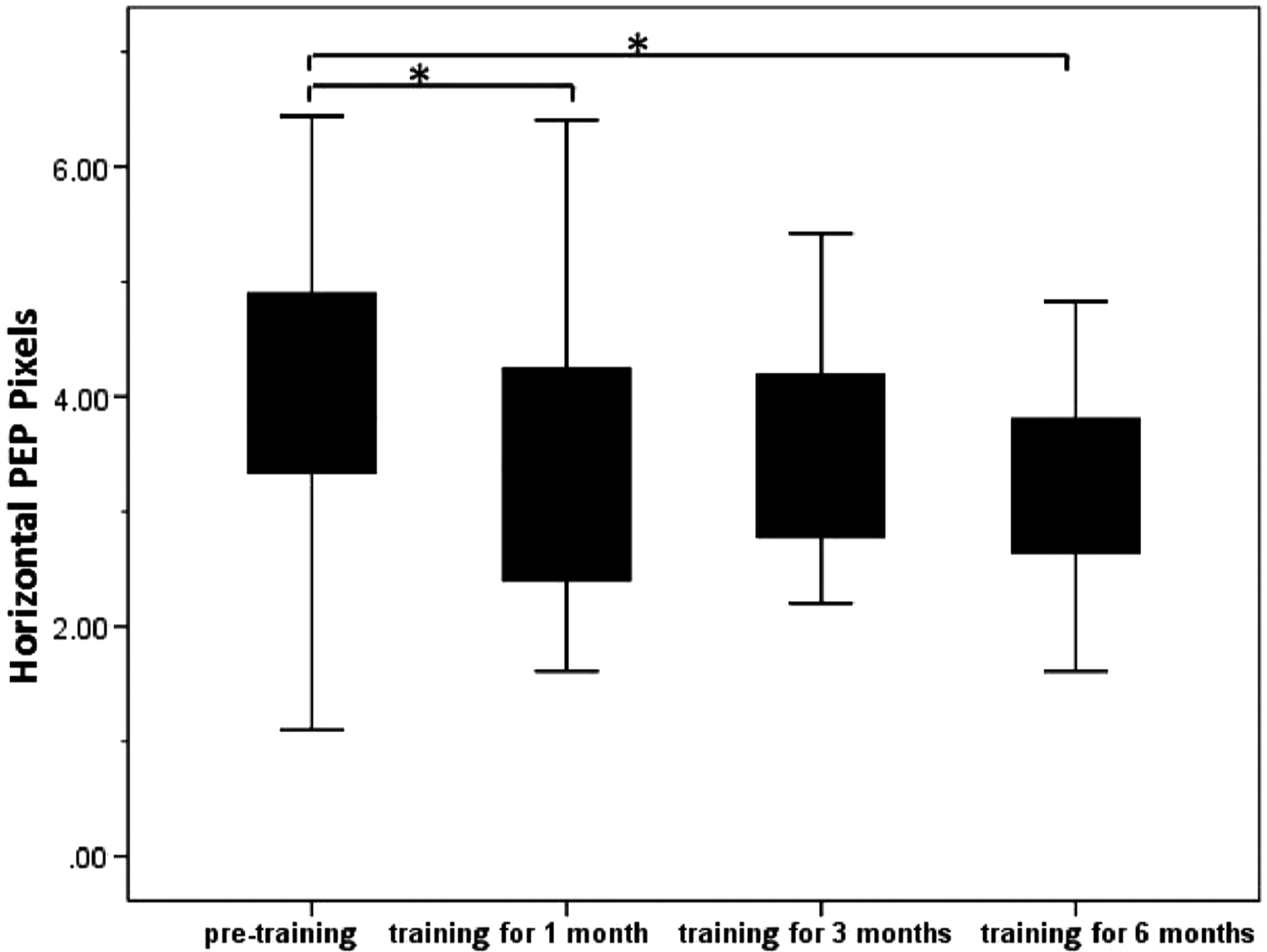
Bar graph showing the horizontal PEP pixels of each such examination. Error bars showed the 95% CI. *Statistically significant difference. CI, confidence interval.

Bar graph showing the vertical PEP pixels of each such examination. There was no statistically significant difference among each such examination. Error bars showed the 95% CI.
Comparison of corneal optical reflection and prism diopter before and after training
There were significant differences between before training and after training for 1, 3, and 6 months, respectively, in the cornea's optical reflection and prism diopter (p = 0.000, p < 0.01) (Figs. 7 and 8).
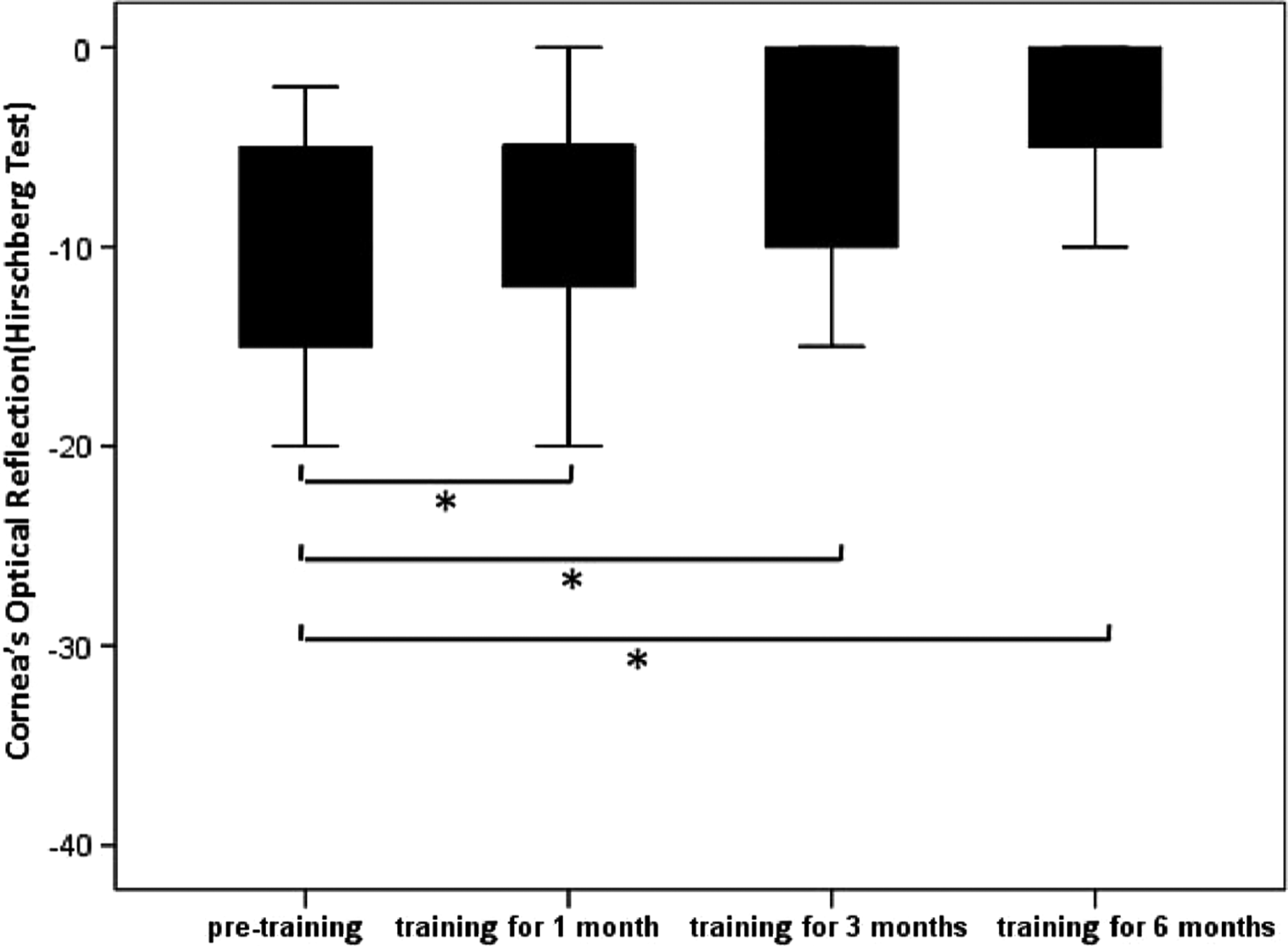
Bar graph showing the corneal optical reflection degree of each such examination. Error bars showed the 95% CI. *Statistically significant difference.

Bar graph showing the prism diopters of each such examination. Error bars showed the 95% CI. *Statistically significant difference.
Discussion
Complications after IXT surgery include overcorrection, under correction, and regression of the degree of strabismus, and are not uncommon. 8 Overcorrection of vision function in young patients can lead to serious consequences including X(T), amblyopia, and distant and near stereoscopic loss. 9 There are disagreements on the timing of surgery for IXT. Factors that determine the timing of surgery include the age, the frequency and duration of strabismus, the angle of strabismus, the reduction of fusion, and whether patients have distant and near stereoscopic loss. Some experts advocate early surgery whereas others suggest terminal surgery. Increasingly many experts favor surgery after stereoscopic loss as the best form of treatment. Serrano-Pedraza et al. reported that IXT patients generally still had stereopsis. 10 When X(T) occurred, the binocular vision information was inconsistent; the corresponding abnormal information on the retina would induce the recurrent vision mechanism in the optic center. It would activate the inhibition blind spot of the temporal retina to inhibit the strabismus eye, with only emmetropia left to avoid diplopia. In general, binocular parallax can induce convergence. 11 But the parallax in strabismus patients was so large that it is beyond the fusion range. Recurrent vision mechanisms are activated to inhibit the strabismus eye and reduce the stimulus, which leads to a decrease in convergence and deflection of the eye position. 10
Binocular vision plays an important role in IXT and it brings new approaches to the development of more effective treatments. Binocular vision training can eliminate the suppression/noise of visual processing channels, 7 enlarge the vision signal of the strabismus eye to make the patient identify diplopia, reversely inhibit recurrent vision mechanism, enhance central control, and thus stimulate correction of the eye position. This study used the binocular dichoptic visual training based on VR technology, which used visual perception and neural plasticity training to remove the obstacle in the visual processing channel and repair the defect of visual function by nonsurgical therapy. This approach can avoid the occurrence of surgical complications, decrease the patients' physical and psychological burden, strengthen patients' confidence, and improve work efficiency further.
Studies in psychophysics and neurobehavioral physiology have demonstrated that there are differences among zero-order, first-order, and second-order perceptual processing areas of multidimensional spaces in the brain. These processing channels also have discrepancy. 12 Hibbard et al. found that the second-order mechanism is related to the first-order mechanism. 13 These channels can enhance the accuracy and depth range of stereoscopic vision, namely stimulation and integration between the first-order and second-order mechanisms to increase the visual signal. 13 Previous studies have found that some patients who were stereonomalous are able to localize stimuli in depth through coarse disparity signals. 14 And some visual normal subjects were not able to judge the relative depth of diplopic targets. 15 These findings might suggest that the impairments of strabismus and amblyopia patients at zero-order may still have first-order and second-order space perceptions. Amblyopia patients who have undamaged zero-order space perceptions can also have impairments of first-order and second-order space perceptions.
In this study, the intelligent platform of the visual perception module based on VR technologies can reveal a series of brain neural processes and responses after images were received by retinal cells. VR optical tools can be more accurate in measuring the binocular visual perceptual defect status and in accurately quantifying the neural response threshold. We reported a preliminary result of this study evaluating the outcomes of binocular dichoptic visual training based on VR platform display in IXT patients. After 6 months of neuroplasticity training of visual sensory perception, stereopsis and eye position of all 25 IXT patients had been improved. These results are consistent with those reported also in a previous study evaluating the effects of other dichoptic training in amblyopia. 16 We found no previous VR studies about IXT. In our sample, eye positions of three patients (13, 18, and 25) who did not have zero-order stereopsis but did have second-order stereopsis after the treatment had been corrected. There are three possible reasons: there are wide individual differences in brain plasticity and lower brain plasticity might be one of the reasons for the absence of stereopsis improvement in three patients, these three patients might have undetected residual zero-order stereopsis or have recreated it (there is no developed dynamic test of stereo acuity to allow fully informed patient management decisions to be made), and motivation of patients may play an important role in the results. In future studies, we will vary the patterns and schemes of visual testing to further understand and determine these study results.
IXT patients were affected due to their ability to control the eye position with fusion force although convergence was diminished. 11 Subsequently, the frequency and degree of strabismus increased gradually, which aggravated the loss of fusion control and the formation of the inhibition blind spot. The eye position and differences in binocular vision were commonly used to evaluate the severity of IXT. However, the examinations that were most widely used to measure the eye position clinically, such as synoptophore, separate the eyes in unnatural conditions, sometimes without the same visual background, which leads to the inhibition of the strabismus eye. Hence, it has limited the accuracy of distance stereopsis examination in IXT patients and fails to better reflect the relationship between the eyes. In our study, dichoptic examination was applied. Compared with clinical routine eye level examinations, there was a change in the perceptual condition, which was closer to the physiological state. The quantitative detection of the eye level was more accurate because of the results found using pixel values. Zhao et al. 17 defined it as the PEP. In our study, the average pixels of horizontal PEP before treatment were 146.24 ± 204.52 pixels; the average pixels of vertical PEP were16.72 ± 29.35 pixels. These outcomes decreased obviously along with longer training time. The average pixels of horizontal PEP after training for 6 months were 38.54 ± 35.36 pixels (Δ6-0 = −0.80, p = 0.018); the average pixels of vertical PEP were 4.75 ± 5.64 pixels (Δ6-0 = −0.48, p = 0.083). It might suggest that the fusion ability was enhanced, the central control ability was enhanced, and the level of brain perception was improved to control eye position. In contrast, the average pixels of horizontal PEP after training for 3 months were not significantly different (Δ3-0 = −0.29, p = 0.370). The results may reflect the additional time and repetition required to establish new nerve reflexes. These results seen are similar to previous studies.18–20 Because the function of the cerebral visual center had been strengthened, the degree of corneal optical reflection and prism diopters after training were gradually improved. Satisfactory alignment was defined as esophoria/tropia ≤5Δ to exophpria/tropia ≤8Δ. 21 There were 18 out of 25 patients who achieved normal eye position after training.
In this preliminary study, we have applied a program of training twice a day for 6 months. The reason for choosing this protocol was based on the following factors: the length of time required for the formation of new nerve reflexes, issues of compliance in patients' treatment (the duration of each training session is short: 10 minutes), and the stimulation intensity is moderate, between the two training sessions. Short-term plasticity is more effective in the long-term potentiation for the process of establishing synapses.22–24
Our results demonstrate that neuroplasticity perceptual learning based on VR cognitive technology can be applied in IXT treatment to promote the establishment of a patient's binocular relationship and correction of offset eye position. These noninvasive techniques offer an alternative to strabismus surgery. A limitation of our study was the small sample size. We are currently expanding our sample size to further verify the effectiveness of this nonsurgical therapy.
Patients younger than 18 years had a larger amplification of diopter in the early period compared with normal children of the same age. The amplification tended to be stable from 3 to 6 months. It is possible that in the early training phase, the binocular relationship is still developing, central control is weak, and the stability of foveal vision fluctuates, stimulating axial growth. 25 After 6 months of training, certain neural relays will have been established, central control enhanced, foveal vision becomes stable, binoculus is balanced, and the refractive degree stability established. Further research will be necessary to confirm this hypothesis.
Footnotes
Acknowledgments
This study was supported by the Major Program, International Science and Technology Cooperation Program of Science and Technology Program of Guangzhou, China (Grant No. 201704020048) and Science and Technology Planning Project of Guangdong Province of China (Grant No. 2017B010110013).
Author Disclosure Statement
No competing financial interests exist.