
Abstract
Abstract
Perinatal mental illness refers to psychiatric disorders that exist during pregnancy and up to 1 year after childbirth. The aim of this systematic review was to discuss the use of Information and Communication Technologies (ICTs) on perinatal depression (PeD) screening in the past three decades. Published articles were searched between 1990 and 2018, both in English and Spanish. In the search, we used different keywords, such as “pregnancy,” “depression,” or “technology” in ScienceDirect, PubMed-NCBI, and Web of Science. We found 10 articles that combined the use of ICTs and a focus on PeD screening. Studied periods included pregnancy (n = 2) and postpartum (n = 8). The telephone was the most commonly used communication method (n = 5), followed by the Internet (n = 4). One investigation used both, the telephone and the Internet. The Edinburgh Postnatal Depression Scale was the most frequently used screening measure (n = 8). The proportion of depressed perinatal women varied across studies depending on the pregnancy status and the cutoff values used, showing a very broad range between 5.8 and 51.9 percent. Despite the increasing popularity of ICTs in health settings, their use in perinatal mental health screening is still rare. Overall, encouraging findings have been reported when using ICTs for screening of PeD, such as eliminating the need to travel to the health center to conduct the screening and allowing for a wider dissemination. However, more research is needed to support their inclusion in perinatal care.
Introduction
P
Perinatal depression (PeD) is estimated to affect between 3 and 6 percent of women. 3 During pregnancy, depression prevalence in different studies and countries has ranged from 6 to 12 percent.4,5 In the postpartum, depression has been estimated to affect between 7 and 25 percent of women.6–10
PeD is a major public health concern because of its negative consequences for the mother, the fetus, and the baby. 11 For instance, depression during pregnancy has been linked to increased childbirth complications, including premature birth, low birth weight, and preeclampsia. Moreover, postpartum depression (during the first year after delivery) is associated with poor performance in the babies' behavioral, cognitive, and emotional domains.12–14 Not surprisingly, identification and management of PeD and other mental health disorders have become a fundamental goal of the World Health Organization. 15
Fortunately, the perinatal period provides a unique opportunity for the detection of depressive symptoms because of the continuous medical monitoring of women, especially during pregnancy. Also encouragingly, previous studies and guidelines have shown that assessment of PeD can be carried out quickly with only one or two brief screening questions, which might be as valid and effective as long, structured mental health assessment methods.16–20
In this scenario, an early detection of depressive symptoms in the perinatal period, which reduces the impact of mental illness on the mother, the baby, and the family, 21 should be feasible. Unfortunately, despite the benefits of early detection and intervention of pregnant women with depressive symptoms are well known and although we have instruments to measure them, PeD is often undetected and, consequently, undertreated or addressed after its onset.22,23
There might be several reasons to explain why the identification of PeD is still unsuccessful, including difficulties in the health care professional and the mothers. On the one hand, some factors explaining why prompt and adequate screening by health care professionals is rare might include a reduced awareness about the problem, time constraints for exhaustive assessments during and between consultations, lack of established policies for care, or unclear referral networks.4,24–27
On the other hand, barriers in perinatal women have also been reported. For instance, some maternal and pregnancy characteristics, such as being a young mother with an intermediate education level, being born abroad, and being in the first trimester of pregnancy are related to lower consultation of a mental health specialist. 22 Other barriers in the mother are related to sociocultural and environmental factors. Some of these include difficulties in combining child care and face-to-face psychological interventions, not knowing where to go to receive treatment, time limitations, transportation difficulties, social stigma associated with mental illness, and fear that their baby could be removed from their care.28–32
In the light of the previous findings, the goal of this study was to review how Information and Communication Technologies (ICTs) have been used in PeD screening and to discuss to which extent they might help overcome some of the barriers presented previously. During the past years, the use of ICTs in the health service industry (eHealth) has increased spectacularly, arguably because of the decrease in their cost and their increased availability in the general population. 33 For instance, in 2017 Internet access and portable electronic devices connected to the Internet (e.g., smartphones, laptops, and tablets) were available to 87 and 65 percent of Europeans, respectively.34,35 Also importantly, 51 percent of individuals used the Internet to seek health-related information in 2017. 36
The use of ICTs in PeD might minimize some of the aforementioned barriers experimented by perinatal women when looking for mental health advice. For instance, ICTs allow a flexible access to screening and treatment, which can be performed anytime and anywhere, eliminating travel costs and facilitating the combination of child care and self care.37–39 In addition, ICTs offer anonymous help, which can minimize stigmatization, 40 improve help-seeking behaviors among perinatal women, 41 and decrease participants' inclination to give a socially desirable response, thus encouraging more honest answers because of a sense of privacy and lack of perceived judgment. 42 In fact, anonymity seems to be a key aspect in the assessment of PeD, as higher prevalence rates of PeD have been obtained when women filled out a questionnaire at home on their own compared with phone calls by nurses. 43
ICTs could also be useful for health professionals to communicate with patients and colleges in a more effective and immediate manner, as well as to support their decisions or to seek information. 44 Moreover, ICTs could make consultations more efficient if screenings completed by the mothers at their homes remotely informed the clinicians of important undesired events, such as an increase in depressive symptoms, without the need to have on-site consultations for such assessments. 45 In fact, health care professionals believe that the use of ICTs in PeD screening has important benefits, such as eliminating language barriers reducing redundancy and human errors, and increasing the client's privacy. 46
This study will review the contributions of ICTs in the field of PeD screening in the past three decades (since 1990). In doing so, we will report the sample characteristics (e.g., pregnancy period), type of ICT employed (e.g., phone calls or the Internet), procedures and instruments used for screening, and the main findings in the perinatal literature. In addition to providing an overview of existent research using ICTs for PeD screening, the implications of the findings and future lines of research will be discussed.
Methods
Scientific articles including the use of ICTs for depression screening during the perinatal period were consulted after an extensive literature search using vertical search options.
Literature search
The systematic search for scientific articles was carried out in March 2018. The information was consulted on the following databases: ScienceDirect, PubMed-NCBI, and Web of Science. Key terms used are in line with previous reviews on ICTs and health47,48 and included: “perinatal,” “pregnant,” “pregnancy,” “prenatal,” “postnatal,” “postpartum,” “depression,” “depressive symptoms,” “technology,” “technologies,” “Internet,” “eHealth,” “mHealth,” “ICT,” “mobile,” “app,” “application,” “phone,” “telephone,” “smartphone,” “tablet,” “PDA,” and “screening.” The search was limited to articles published between 1990 and March 2018. Key terms were searched in the abstract. The specific search terms used in ScienceDirect are reported in Appendix 1. We used the same search strategy for all databases.
Two of the authors, namely V.M.B. and C.S.R, conducted the research independently and selected the articles (see a more detailed description in section “Literature selection”). The results obtained by each researcher were compared to ensure that the final database included all the articles. The agreement in the number of articles found between both researchers was 89 percent.
Literature selection
A prerequisite to select a study was that any form of ICT was used in the screening of PeD. The review includes articles published in English and Spanish to provide an overview of the use of ICTs for PeD screening in the past decades and to discuss its current state of the art. The eligibility of studies was assessed following a series of steps according to eligibility criteria (Table 1). First, a selection was made by looking at the article title and abstract. Then, the full text was read for the selected articles and additional references were searched within the text. A flow diagram of the selection process is given in Figure 1. The diagram will only be presented for one researcher (V.M.B.) to facilitate the readability of the text. As described previously, the same procedure was followed by C.S.R.
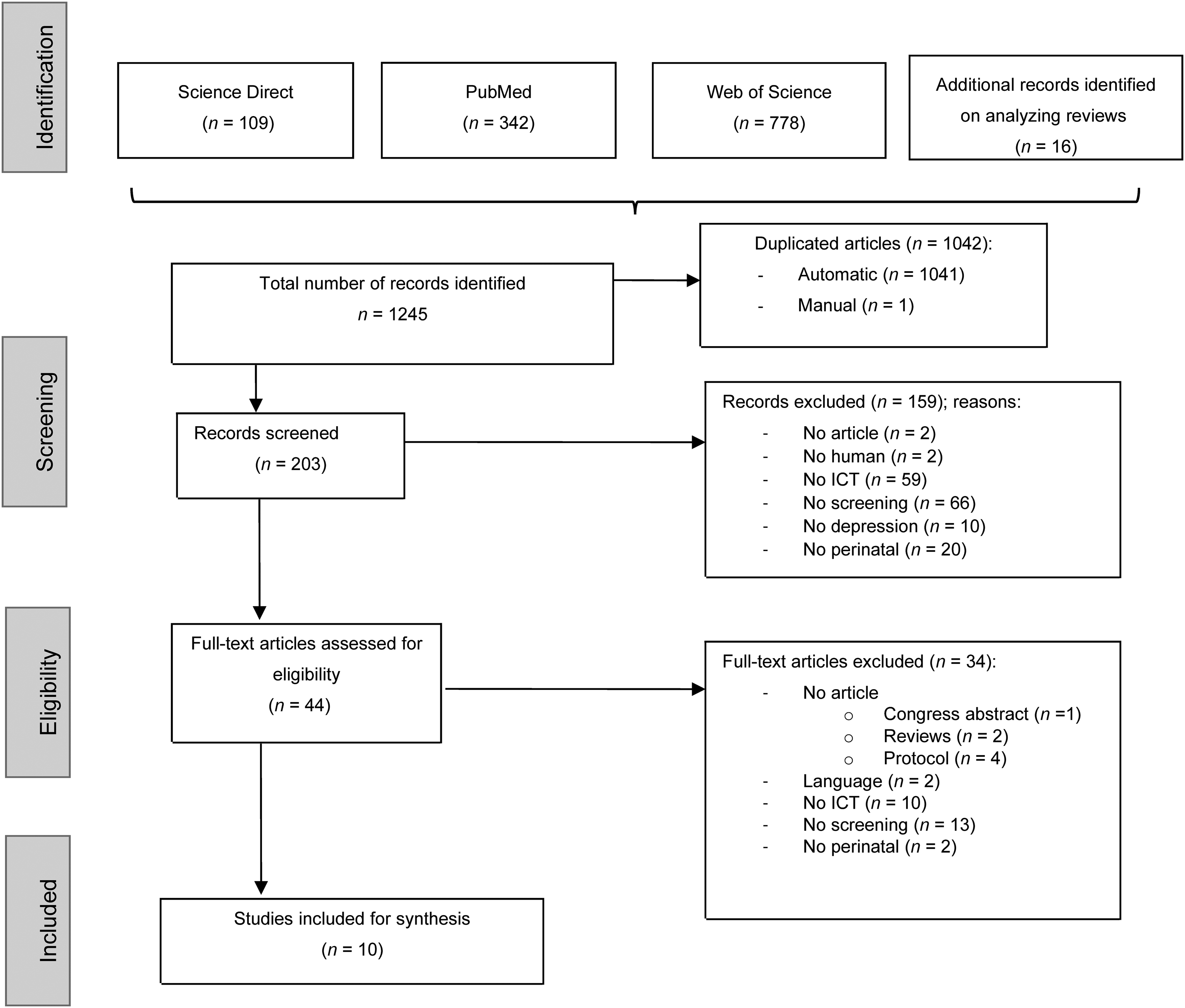
Flow diagram of study selection. ICT, Information and Communication Technology.
Inclusion and Exclusion Criteria
ICT, Information and Communication Technologies.
Results
Sample characteristics
After comparing the findings from both researchers, the first search yielded 188 results. Of these, 10 articles met the inclusion criteria (Table 2).
Main Characteristics of the Studies Included (n = 10)
We have included only the last name of the first author.
EPDS, Edinburgh Postnatal Depression Scale; PDSS, Postpartum Depression Screening Scale; SCID-I, Structured Clinical Interview for Disorders.
Sample characteristics are given in Table 2. The majority of studies (n = 8) have been conducted in the United States.28,39,41,43,49–52 The remaining two investigations were from England 53 and Canada. 54 Most studies have included women older than 18 years of age, but four articles also recruited adolescent mothers.43,51,52,54
Regarding the period of interest, most investigations focused on postpartum (n = 8, 80 percent).28,41,43,49–52,54 Only two articles (20 percent) screened for depression during the prenatal period.39,53 Also interestingly, we observed that the moment in which screening was conducted varied widely across investigations. For instance, in the prenatal period, studies included women at any gestational stage.39,53 Similarly, the period of interest during the postpartum varied from 7 days after childbirth to 6 months postpartum depending on the study (n = 7; 70 percent),28,41,43,49,51,52,54 whereas one investigation included screening up to 1 year after delivery. 50
Type of ICT
As given in Table 2, ICTs have included the phone (n = 5, 50 percent)39,41,49,51,54 and the Internet (n = 4, 40 percent).28,50,52,53 One investigation used both types of ICTs. 43 For those using the telephone, screening was carried out through telephone calls (n = 4, 40 percent)41,43,51,54 or through an interactive voice response system (n = 2, 20 percent).39,49 By contrast, studies that preferred the Internet as a way of screening for PeD, have used web pages (n = 3, 30 percent),28,50,52 a tablet application (n = 1, 10 percent), 53 or e-mails (n = 1, 10 percent). 43
Instruments used to assess depressive symptomatology
The Edinburgh Postnatal Depression Scale (EPDS) 55 has been the most frequently selected tool for depression screening across studies (n = 8, 80 percent).28,39,41,43,49,52–54 Some authors used the Postpartum Depression Screening Scale (PDSS) 56 as an alternative to the EPDS (n = 2, 20 percent),50,51 whereas others administered the Whooley questionnaire 20 or the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) Structured Clinical Interview for Axis I Disorders—Clinician Version (SCID-CV) 57 as a complement to the EPDS (n = 2, 20 percent).53,54
Although screening tools were similar in the majority of studies, the selected cutoff points were very diverse. The screening cutoff for the EPDS ranged from 8 to 13 across investigations. For instance, three studies (30 percent) used a single cutoff score of 8, 41 10, 43 or 13, 52 whereas other authors (n = 5, 50 percent)28,39,49,53,54 established two cutoff points, one for moderate (EPDS ≥10–11) and another for severe (EPDS ≥12–13) depressive symptoms. Taking the PDSS, selected cutoffs for moderate and severe depression were 60–80 and >80, respectively.50,51
Study findings
When screening occurred during pregnancy, the proportion of women with depressive symptoms varied considerably across studies. Some authors 39 reported that 9.3 percent women presented with mild depressive symptoms (EPDS >10 ≤ 11), whereas 29.6 percent were categorized as experiencing major depressive symptoms (EPDS ≥12). A most recent study revealed a lower proportion of severely depressed women, that is, a 7.2 percent of women with EPDS scores of between 10 and 12 and only 5.8 percent of women indicating EPDS scores >13. 53
The proportion of depressed women in the postnatal period was somewhat higher than those reported during pregnancy. However, results varied greatly across investigations, arguably as a result of the different cutoffs used. Not surprisingly, the more restrictive the cutoff was, the fewer depressed women were reported. For instance, one study using an EPDS cutoff of 8 obtained that 51.9 percent of participants were depressed. 41 By contrast, when the EPDS cutoff was set to ≥10, the proportion of depressed women decreased to between 6.2 54 and 17 percent. 49 The most recommended cutoff of 12 yielded a proportion of depressed women of between 3.4 54 and 11.1 percent. 49 Finally, when using the most restrictive cutoff of EPDS >13, the proportion of women depressed ranged from 5.5 28 to 16 percent. 52
During the postpartum, depression screening using the PDSS with a cutoff of 80 indicated that between 9 51 and 23 percent 50 of women met criteria for major postpartum depression. When authors used a lower cutoff (between 60 and 80), the prevalence of depression was found to be 15 percent. 51
Discussion
This study aimed at reviewing the existing literature into the use of ICT for PeD. The importance of the topic lies in the fact that use of these tools, which has boosted in health settings in the past decades because of their increased availability in the population, 33 has been argued to overcome some of the existent barriers in screening for PeD.40–42 For instance, health care professionals have reported time constraints that make active, repeated assessment unfeasible. 44 In addition, perinatal women have indicated that anonymity and flexibility in the time to perform the assessment or to receive treatment are important factors influencing their decision to search for mental health assistance.58,59
Despite the potential of ICT in PeD screening, this review evidenced that the integration of ICT in this field is still very rare. In addition, our study revealed some strengths (e.g., the consensus about the screening tool to be used) and weaknesses (e.g., inconsistency in the cutoffs used, infrequent use of apps for telemonitoring, exclusion of teenage mothers, and a major focus on the postpartum period) of the existent literature.
One important finding in this study was that the EPDS seems to be the preferred tool in studies using ICT for PeD screening,28,39,41,43,49,52–54 followed by the PDSS.50,51 Readers should keep in mind that the EPDS and the PDSS are not diagnostic tools, so women scoring above the cutoff should undergo a formal diagnosis assessment by a mental health specialist.56,60,61 However, investigations have shown that brief screening questions have a good diagnostic validity compared with structured mental health assessment and are recommended before a more in-depth evaluation is made.16–20
In contrast to the popularity of the EPDS, our review revealed that the ICT use to perform the final diagnostic assessment has been very rare, 54 which suggests that health care professionals still rely on face-to-face interaction for the diagnosis of PeD. A recent study supports this idea, as sanitarians (psychologists and psychiatrists) seem to trust e-mental health applications for screening, prevention, followup, and positive psychology intervention, but they are skeptical with regard to their use in other forms of treatment and diagnosis of maternal depression. 45
Another interesting result in this investigation was that, despite the consensus about the use of the EPDS for PeD screening using ICT, the cutoff to be used is not well-established. Specifically, a number of studies selected the recommended cutoff of 12 for severe depressive symptoms,28,39,49,53,54 but less (EPDS >8 or EPDS ≥10)41,43 and more restrictive cutoffs have also been utilized (EPDS ≥13). 52 This is problematic, as prevalence scores will likely differ as a function of the cutoff used and, most importantly, this will affect the recommendation made to the mothers. According to the existent literature on the EPDS, the recommended cutoff of 12 55 should be preferred unless clearly justified. In support of this, studies using this cutoff have reported prevalence scores between 3.4 and 11.1 percent, which are similar to the prevalence reported by the American Psychiatric Association. 3
An important goal in this study was to explore the types of ICT used by researchers. The past decades have seen a surge in the number tools available, from the first fixed devices (e.g., phones and computers) to smartphones and wearable technology that have made ecological, momentary assessment feasible. Despite the current advances in ICT, research into PeD has mostly relied on phone calls and, to a lesser extent, web pages for screening.28,41,43,50–52,54 In fact, our search indicated that only one study used an application for a portable device, that is, a tablet 53 and no investigation included a smartphone app to ecologically screen for depression.
At this point, some considerations should be made. Recent reports have repeatedly indicated that the proportion of individuals owning a portable electronic device connected to the Internet 35 and the use of the Internet to seek for health-related information 36 have grown spectacularly. Similarly, the use of smartphone applications by perinatal women is becoming more and more frequent. 62 In fact, the use of smartphone apps is argued to be the current gold standard assessment method in health settings as it reduces costs (phone calls by the health care professional are substituted for a continuous assessment with the app), it allows for telemonitoring (it captures and communicates data in real time), it is ecological (mothers can answer wherever they are removing the need to connect to their computer at home or to travel to the clinic), and it is minimally invasive (mothers can decide when to answer to the app, which is more difficult when phone calls are used for assessment). 63 Also importantly, there is recent evidence to suggest that the use mobile devices when administering validated screening scales does not affect data equivalence compared with traditional assessment modes, such as paper64,65 and that less personal assessment tools (e.g., mail as opposed to phone calls) result in higher PeD prevalence rates, 43 supporting the use of more impersonal screening tools, such as smartphone apps, in PeD.
In addition to the infrequent use of modern, anonymous ICT screening tools, our review of the literature also evidenced a tendency to exclude teenage mothers in studies using ICT for PeD screening. This is alarming because young mothers are less likely to consult a mental health specialist. 22 Furthermore, teenager mothers seem to present with higher depression prevalence rates than adult mothers (17 and 3.3 percent, respectively) and many of them (up to 20 percent) report having committed suicide attempts during pregnancy. 66 For these reasons and also because this population arguably has a high knowledge of ICTs, teenage mothers are good candidates to benefit from ICT screening programs for PeD and should not be excluded from future research into this topic.
A final shortcoming revealed by the present investigation is that the majority of reviewed studies had a focus on the postnatal period, despite the well-established benefits of early screening during pregnancy.37–39 Considering the existing link between prenatal and postpartum depression,67–69 the high prevalence rates of prenatal depression obtained in this review (between 5.8 and 29.6 percent), and the consequences of prenatal depression on the fetus and later on the baby,12–14 routine depression screening throughout the pregnancy period should be an urge.
Related to this, we found that the majority of reviewed investigations have been cross-sectional studies with a single screening point, with no consensus about the best time for screening during pregnancy or postpartum and with no followup. In our opinion, the fact that prenatal depressive symptoms often persist at least during the first year postpartum,70–72 future research and screening programs should be characterized by a more frequent assessment starting early during pregnancy and finishing no sooner than 1 year after delivery. We believe that the use of ICTs will surely facilitate this repeated screening of depressive symptoms during obstetric (pregnancy) and pediatric (postpartum) revisions. 41 However, further research is needed to determine the optimal quantity and timing of evaluations to rapidly and efficiently detect the onset of PeD.
Implications for Future Research and Clinical Practice
The use of e-health and m-health will surely change the way screening will happen in the future in perinatal care. There are, however, some challenges to their implementation that will need to be addressed in future developments. Engagement, for instance, is a critical element that will determine whether individuals are willing to use these technologies. There are some characteristics intrinsic to ICTs that may favor engagement in perinatal women. For instance, ICTs give the control and responsibility of medical care to the patient, who can decide when and how to perform the evaluation.
Making the technology customizable is another way of enhancing engagement, as reported by women.38,58 Virtual and augmented reality might serve this purpose,73,74 as both technologies make customization feasible. To date, however, the utility of virtual and augmented reality for mental health screening in perinatal women remains unexplored. Other strategies to promote engagement in self-monitoring using ICT are gamification and social interactions.75,76 For instance, participating women could be allowed to share their experiences with other women using the same technologies and could obtain rewards in the form of unlocking treatment content (i.e., a module on emotion regulation or psychology quotes) as they respond to the assessments.
As a final remark, we would like to draw attention to perceived utility and ease of use as key factors that should be considered in future developments of ICT in perinatal care, as both elements are excellent predictors of technology use. 77 Some strategies in this direction would include involving the target population in technology development and providing immediate feedback to the individual and the health care provider.78–80 To sum, what this study indicates is that the use of ICT in perinatal screening is very limited and mostly represented by old-fashioned tools that make repeated, self-monitoring and telemonitoring almost impossible. There is a need to adopt more modern screening strategies that eliminate common barriers for seeking mental care in the perinatal period.
Conclusions
Routine screening for perinatal mental health is crucial both for the mother and the baby. 51 However, barriers in the mother (e.g., difficulties travelling to the clinic, the stigma of mental health, and combining childcare and face-to-face consultations) and the health care professional (e.g., lack of time) make repeated assessment difficult. The use of ICT, especially smartphones, has been argued to overcome some of the limitations described previously as it allows for telemonitoring without the need for face-to-face interactions and eliminates the need to involve a human evaluator. 81 Not surprisingly, smartphone apps are perceived by many as the current gold standard assessment tools in health settings.44–46,65
Despite the aforementioned potential advantages of using smartphone apps for routine screening of depression in perinatal women, our review underlined that (a) ICT methods used to date tend to require a human evaluator (e.g., phone calls), (b) repeated screening to explore the evolution of mothers is very rare (frequently only once), (c) the cutoffs used for depression have been inconsistent, (d) the focus has been mostly on postpartum mental health, and (e) teenage mothers have been frequently ignored. In the light of these findings, we believe that there is an important gap in the literature into screening for PeD using ICT. Future research should explore the feasibility and utility of routine screening from early pregnancy periods to at least 1 year postpartum using smartphone apps, so that the onset of depression can be rapidly detected at any stage during the perinatal period.
Footnotes
Acknowledgments
This study was partially supported by the Universidad de Zaragoza, Gobierno de Aragón, (Departamento de Innovación, Investigación y Universidad), FEDER “Construyendo Europa desde Aragón”; Fundación Universitaria Antonio Gargallo (2013/B006 y 2014/B006), and Obra Social Ibercaja.
Author Disclosure Statement
No competing financial interests exist.
Final Search Terms in Science Direct
| Search | Keywords | Results |
|---|---|---|
| 1 | “perinatal” AND “depression” AND “technology” AND “screening” | 0 |
| 2 | “perinatal” AND “depression” AND “technologies” AND “screening” | 0 |
| 3 | “perinatal” AND “depression” AND “Internet” AND “screening” | 4 |
| 4 | “perinatal” AND “depression” AND “eHealth” AND “screening” | 1 |
| 5 | “perinatal” AND “depression” AND “mHealth” AND “screening” | 0 |
| 6 | “perinatal” AND “depression” AND “ICT” AND “screening” | 0 |
| 7 | “perinatal” AND “depression” AND “mobile” AND “screening” | 0 |
| 8 | “perinatal” AND “depression” AND “app” AND “screening” | 0 |
| 9 | “perinatal” AND “depression” AND “application” AND “screening” | 0 |
| 10 | “perinatal” AND “depression” AND “phone” AND “screening” | 2 |
| 11 | “perinatal” AND “depression” AND “telephone” AND “screening” | 3 |
| 12 | “perinatal” AND “depression” AND “smartphone” AND “screening” | 0 |
| 13 | “perinatal” AND “depression” AND “tablet” AND “screening” | 1 |
| 14 | “perinatal” AND “depression” AND “PDA” AND “screening” | 0 |
| 15 | “perinatal” AND “depressive symptoms” AND “technology” AND “screening” | 0 |
| 16 | “perinatal” AND “depressive symptoms” AND “technologies” AND “screening” | 0 |
| 17 | “perinatal” AND “depressive symptoms” AND “Internet” AND “screening” | 3 |
| 18 | “perinatal” AND “depressive symptoms” AND “eHealth” AND “screening” | 1 |
| 19 | “perinatal” AND “depressive symptoms” AND “mHealth” AND “screening” | 0 |
| 20 | “perinatal” AND “depressive symptoms” AND “ICT” AND “screening” | 0 |
| 21 | “perinatal” AND “depressive symptoms” AND “mobile” AND “screening” | 0 |
| 22 | “perinatal” AND “depressive symptoms” AND “app” AND “screening” | 0 |
| 23 | “perinatal” AND “depressive symptoms” AND “application” AND “screening” | 1 |
| 24 | “perinatal” AND “depressive symptoms” AND “phone” AND “screening” | 0 |
| 25 | “perinatal” AND “depressive symptoms” AND “telephone” AND “screening” | 1 |
| 26 | “perinatal” AND “depressive symptoms” AND “smartphone” AND “screening” | 0 |
| 27 | “perinatal” AND “depressive symptoms” AND “tablet” AND “screening” | 0 |
| 28 | “perinatal” AND “depressive symptoms” AND “PDA” AND “screening” | 0 |
| 29 | “pregnant” AND “depression” AND “technology” AND “screening” | 0 |
| 30 | “pregnant” AND “depression” AND “technologies” AND “screening” | 0 |
| 31 | “pregnant” AND “depression” AND “Internet” AND “screening” | 2 |
| 32 | “pregnant” AND “depression” AND “eHealth” AND “screening” | 0 |
| 33 | “pregnant” AND “depression” AND “mHealth” AND “screening” | 0 |
| 34 | “pregnant” AND “depression” AND “ICT” AND “screening” | 0 |
| 35 | “pregnant” AND “depression” AND “mobile” AND “screening” | 0 |
| 36 | “pregnant” AND “depression” AND “app” AND “screening” | 0 |
| 37 | “pregnant” AND “depression” AND “application” AND “screening” | 3 |
| 38 | “pregnant” AND “depression” AND “phone” AND “screening” | 2 |
| 39 | “pregnant” AND “depression” AND “telephone” AND “screening” | 2 |
| 40 | “pregnant” AND “depression” AND “smartphone” AND “screening” | 0 |
| 41 | “pregnant” AND “depression” AND “tablet” AND “screening” | 2 |
| 42 | “pregnant” AND “depression” AND “PDA” AND “screening” | 0 |
| 43 | “pregnant” AND “depressive symptoms” AND “technology” AND “screening” | 0 |
| 44 | “pregnant” AND “depressive symptoms” AND “technologies” AND “screening” | 0 |
| 45 | “pregnant” AND “depressive symptoms” AND “Internet” AND “screening” | 1 |
| 46 | “pregnant” AND “depressive symptoms” AND “eHealth” AND “screening” | 0 |
| 47 | “pregnant” AND “depressive symptoms” AND “mHealth” AND “screening” | 0 |
| 48 | “pregnant” AND “depressive symptoms” AND “ICT” AND “screening” | 0 |
| 49 | “pregnant” AND “depressive symptoms” AND “mobile” AND “screening” | 0 |
| 50 | “pregnant” AND “depressive symptoms” AND “app” AND “screening” | 0 |
| 51 | “pregnant” AND “depressive symptoms” AND “application” AND “screening” | 0 |
| 52 | “pregnant” AND “depressive symptoms” AND “phone” AND “screening” | 0 |
| 53 | “pregnant” AND “depressive symptoms” AND “telephone” AND “screening” | 0 |
| 54 | “pregnant” AND “depressive symptoms” AND “smartphone” AND “screening” | 0 |
| 55 | “pregnant” AND “depressive symptoms” AND “tablet” AND “screening” | 0 |
| 56 | “pregnant” AND “depressive symptoms” AND “PDA” AND “screening” | 0 |
| 57 | “pregnancy” AND “depression” AND “technology” AND “screening” | 1 |
| 58 | “pregnancy” AND “depression” AND “technologies” AND “screening” | 1 |
| 59 | “pregnancy” AND “depression” AND “Internet” AND “screening” | 2 |
| 60 | “pregnancy” AND “depression” AND “eHealth” AND “screening” | 0 |
| 61 | “pregnancy” AND “depression” AND “mHealth” AND “screening” | 0 |
| 62 | “pregnancy” AND “depression” AND “ICT” AND “screening” | 0 |
| 63 | “pregnancy” AND “depression” AND “mobile” AND “screening” | 0 |
| 64 | “pregnancy” AND “depression” AND “app” AND “screening” | 0 |
| 65 | “pregnancy” AND “depression” AND “application” AND “screening” | 5 |
| 66 | “pregnancy” AND “depression” AND “phone” AND “screening” | 3 |
| 67 | “pregnancy” AND “depression” AND “telephone” AND “screening” | 7 |
| 68 | “pregnancy” AND “depression” AND “smartphone” AND “screening” | 0 |
| 69 | “pregnancy” AND “depression” AND “tablet” AND “screening” | 0 |
| 70 | “pregnancy” AND “depression” AND “PDA” AND “screening” | 0 |
| 71 | “pregnancy” AND “depressive symptoms” AND “technology” AND “screening” | 0 |
| 72 | “pregnancy” AND “depressive symptoms” AND “technologies” AND “screening” | 0 |
| 73 | “pregnancy” AND “depressive symptoms” AND “Internet” AND “screening” | 1 |
| 74 | “pregnancy” AND “depressive symptoms” AND “eHealth” AND “screening” | 0 |
| 75 | “pregnancy” AND “depressive symptoms” AND “mHealth” AND “screening” | 0 |
| 76 | “pregnancy” AND “depressive symptoms” AND “ICT” AND “screening” | 0 |
| 77 | “pregnancy” AND “depressive symptoms” AND “mobile” AND “screening” | 0 |
| 78 | “pregnancy” AND “depressive symptoms” AND “app” AND “screening” | 0 |
| 79 | “pregnancy” AND “depressive symptoms” AND “application” AND “screening” | 0 |
| 80 | “pregnancy” AND “depressive symptoms” AND “phone” AND “screening” | 0 |
| 81 | “pregnancy” AND “depressive symptoms” AND “telephone” AND “screening” | 2 |
| 82 | “pregnancy” AND “depressive symptoms” AND “smartphone” AND “screening” | 0 |
| 83 | “pregnancy” AND “depressive symptoms” AND “tablet” AND “screening” | 0 |
| 84 | “pregnancy” AND “depressive symptoms” AND “PDA” AND “screening” | 0 |
| 85 | “prenatal” AND “depression” AND “technology” AND “screening” | 0 |
| 86 | “prenatal” AND “depression” AND “technologies” AND “screening” | 0 |
| 87 | “prenatal” AND “depression” AND “Internet” AND “screening” | 0 |
| 88 | “prenatal” AND “depression” AND “eHealth” AND “screening” | 0 |
| 89 | “prenatal” AND “depression” AND “mHealth” AND “screening” | 0 |
| 90 | “prenatal” AND “depression” AND “ICT” AND “screening” | 0 |
| 91 | “prenatal” AND “depression” AND “mobile” AND “screening” | 0 |
| 92 | “prenatal” AND “depression” AND “app” AND “screening” | 0 |
| 93 | “prenatal” AND “depression” AND “application” AND “screening” | 0 |
| 94 | “prenatal” AND “depression” AND “phone” AND “screening” | 1 |
| 95 | “prenatal” AND “depression” AND “telephone” AND “screening” | 0 |
| 96 | “prenatal” AND “depression” AND “smartphone” AND “screening” | 0 |
| 97 | “prenatal” AND “depression” AND “tablet” AND “screening” | 2 |
| 98 | “prenatal” AND “depression” AND “PDA” AND “screening” | 0 |
| 99 | “prenatal” AND “depressive symptoms” AND “technology” AND “screening” | 0 |
| 100 | “prenatal” AND “depressive symptoms” AND “technologies” AND “screening” | 0 |
| 101 | “prenatal” AND “depressive symptoms” AND “Internet” AND “screening” | 0 |
| 102 | “prenatal” AND “depressive symptoms” AND “eHealth” AND “screening” | 0 |
| 103 | “prenatal” AND “depressive symptoms” AND “mHealth” AND “screening” | 0 |
| 104 | “prenatal” AND “depressive symptoms” AND “ICT” AND “screening” | 0 |
| 105 | “prenatal” AND “depressive symptoms” AND “mobile” AND “screening” | 0 |
| 106 | “prenatal” AND “depressive symptoms” AND “app” AND “screening” | 0 |
| 107 | “prenatal” AND “depressive symptoms” AND “application” AND “screening” | 0 |
| 108 | “prenatal” AND “depressive symptoms” AND “phone” AND “screening” | 0 |
| 109 | “prenatal” AND “depressive symptoms” AND “telephone” AND “screening” | 0 |
| 110 | “prenatal” AND “depressive symptoms” AND “smartphone” AND “screening” | 0 |
| 111 | “prenatal” AND “depressive symptoms” AND “tablet” AND “screening” | 0 |
| 112 | “prenatal” AND “depressive symptoms” AND “PDA” AND “screening” | 0 |
| 113 | “postnatal” AND “depression” AND “technology” AND “screening” | 1 |
| 114 | “postnatal” AND “depression” AND “technologies” AND “screening” | 1 |
| 115 | “postnatal” AND “depression” AND “Internet” AND “screening” | 2 |
| 116 | “postnatal” AND “depression” AND “eHealth” AND “screening” | 0 |
| 117 | “postnatal” AND “depression” AND “mHealth” AND “screening” | 0 |
| 118 | “postnatal” AND “depression” AND “ICT” AND “screening” | 0 |
| 119 | “postnatal” AND “depression” AND “mobile” AND “screening” | 0 |
| 120 | “postnatal” AND “depression” AND “app” AND “screening” | 0 |
| 121 | “postnatal” AND “depression” AND “application” AND “screening” | 2 |
| 122 | “postnatal” AND “depression” AND “phone” AND “screening” | 3 |
| 123 | “postnatal” AND “depression” AND “telephone” AND “screening” | 6 |
| 124 | “postnatal” AND “depression” AND “smartphone” AND “screening” | 0 |
| 125 | “postnatal” AND “depression” AND “tablet” AND “screening” | 1 |
| 126 | “postnatal” AND “depression” AND “PDA” AND “screening” | 0 |
| 127 | “postnatal” AND “depressive symptoms” AND “technology” AND “screening” | 1 |
| 128 | “postnatal” AND “depressive symptoms” AND “technologies” AND “screening” | 1 |
| 129 | “postnatal” AND “depressive symptoms” AND “Internet” AND “screening” | 1 |
| 130 | “postnatal” AND “depressive symptoms” AND “eHealth” AND “screening” | 0 |
| 131 | “postnatal” AND “depressive symptoms” AND “mHealth” AND “screening” | 0 |
| 132 | “postnatal” AND “depressive symptoms” AND “ICT” AND “screening” | 0 |
| 133 | “postnatal” AND “depressive symptoms” AND “mobile” AND “screening” | 0 |
| 134 | “postnatal” AND “depressive symptoms” AND “app” AND “screening” | 0 |
| 135 | “postnatal” AND “depressive symptoms” AND “application” AND “screening” | 0 |
| 136 | “postnatal” AND “depressive symptoms” AND “phone” AND “screening” | 0 |
| 137 | “postnatal” AND “depressive symptoms” AND “telephone” AND “screening” | 1 |
| 138 | “postnatal” AND “depressive symptoms” AND “smartphone” AND “screening” | 0 |
| 139 | “postnatal” AND “depressive symptoms” AND “tablet” AND “screening” | 1 |
| 140 | “postnatal” AND “depressive symptoms” AND “PDA” AND “screening” | 0 |
| 141 | “postpartum” AND “depression” AND “technology” AND “screening” | 2 |
| 142 | “postpartum” AND “depression” AND “technologies” AND “screening” | 2 |
| 143 | “postpartum” AND “depression” AND “Internet” AND “screening” | 5 |
| 144 | “postpartum” AND “depression” AND “eHealth” AND “screening” | 0 |
| 145 | “postpartum” AND “depression” AND “mHealth” AND “screening” | 0 |
| 146 | “postpartum” AND “depression” AND “ICT” AND “screening” | 0 |
| 147 | “postpartum” AND “depression” AND “mobile” AND “screening” | 0 |
| 148 | “postpartum” AND “depression” AND “app” AND “screening” | 0 |
| 149 | “postpartum” AND “depression” AND “application” AND “screening” | 3 |
| 150 | “postpartum” AND “depression” AND “phone” AND “screening” | 3 |
| 151 | “postpartum” AND “depression” AND “telephone” AND “screening” | 13 |
| 152 | “postpartum” AND “depression” AND “smartphone” AND “screening” | 0 |
| 153 | “postpartum” AND “depression” AND “tablet” AND “screening” | 0 |
| 154 | “postpartum” AND “depression” AND “PDA” AND “screening” | 0 |
| 155 | “postpartum” AND “depressive symptoms” AND “technology” AND “screening” | 1 |
| 156 | “postpartum” AND “depressive symptoms” AND “technologies” AND “screening” | 1 |
| 157 | “postpartum” AND “depressive symptoms” AND “Internet” AND “screening” | 2 |
| 158 | “postpartum” AND “depressive symptoms” AND “eHealth” AND “screening” | 0 |
| 159 | “postpartum” AND “depressive symptoms” AND “mHealth” AND “screening” | 0 |
| 160 | “postpartum” AND “depressive symptoms” AND “ICT” AND “screening” | 0 |
| 161 | “postpartum” AND “depressive symptoms” AND “mobile” AND “screening” | 0 |
| 162 | “postpartum” AND “depressive symptoms” AND “app” AND “screening” | 0 |
| 163 | “postpartum” AND “depressive symptoms” AND “application” AND “screening” | 0 |
| 164 | “postpartum” AND “depressive symptoms” AND “phone” AND “screening” | 0 |
| 165 | “postpartum” AND “depressive symptoms” AND “telephone” AND “screening” | 2 |
| 166 | “postpartum” AND “depressive symptoms” AND “smartphone” AND “screening” | 0 |
| 167 | “postpartum” AND “depressive symptoms” AND “tablet” AND “screening” | 0 |
| 168 | “postpartum” AND “depressive symptoms” AND “PDA” AND “screening” | 0 |
| 109 |
ICT, Information and Communication Technologies.