
Abstract
Abstract
Avatars, or users' renditions within digital environments, may change depending on modifications of users' self-conception. According to literature, chronic health conditions influence patients and survivors' identity, because living with a disease requires people to reconfigure their self-representation and their own daily life and future plans. This is especially true for breast cancer, whose treatment and surgery also affect patients' body image, sexual identity, and sense of womanhood. In this study, 22 breast cancer survivors were asked to create multiple avatars resembling their actual self (AS), their ideal self (IS), and their self connected to the disease experience; then, they were asked to rate their attitudes toward their three avatars. Results show that disease avatars are significantly different in patients' attitudes toward them from AS and IS avatars. In addition, attitudes toward one's own avatars appeared partially related to clinically relevant psychological states, such as anxiety and depression. Discussion explores suggestions for usage of avatars in interventions for assessment and quality-of-life promotion among chronic patients.
Introduction
Avatars are digital figures representing human users within digital environments, ranging from static images to dynamic, often humanoid, characters able to act and move. According to projective identity theory,1,2 avatars created or customized by users maintain aspects of their identity and self-perception. For example, avatars could be similar to users in terms of physical appearance,3,4 or they may represent the users' personality traits, physical and cognitive development over time, cultural belonging, or even personal beliefs in a symbolic manner.5–8 Moreover, avatars are influenced by context; similar to social identity, they are modified by users depending on the characteristics of the Virtual World they have to enter, the activity to be performed in it (e.g., making friends, or working, or romance), and the expected online audience (e.g., friends or strangers).4,9,10 Recent studies also show that avatars tend to be customized differently when different representations of the self are used as reference. For example, an important part of literature on avatar research11–14 is based on the distinction between actual self (AS) and ideal self (IS) as theorized by Higgins 15 : people have representations of themselves related to what they actually are (AS) and what they want to be in the future or fantasy (IS). The more these two selves are different, the more the person is likely to develop psychopathologies, such as eating disorders, 16 problematic substance use and addiction,17,18 and other compulsive behaviors,19,20 and also detrimental consequences on perceived quality of life and subjective well-being should be expected.21,22 These data are consistent with many theories highlighting that self-representations and identity are multiple and malleable,15,23–25 and that different self-representations are activated by social encounters, environmental and personal circumstances, 25 even by experimental priming. 26
AS (or “real”) and IS theory has been often used in research on avatars. For example, in two studies27,28 Jin found that avatars created by users primed to refer to IS rather than AS were associated to greater self-connection and perceived interactivity during video gaming. Another study 29 showed that avatars were more similar to IS in addicted than healthy players, whereas Kim and Sundar 30 found that participants who created IS avatars were more likely to visualize their own ideal body, whereas participants who created AS avatars showed higher perceived health risk for their own bodies. These results show interesting implications of avatar customization for health care; however, to our knowledge, no studies so far have investigated avatar creation based on illness experience.
Indeed, life events and experiences may deeply influence people self-representation: for example, traumas change the self by introducing a sense of powerlessness and diminishing one's own perception of being able to cope with adverse events. 31 Similarly, chronic health conditions could influence how one sees him or herself, both at a physical level because of bodily symptoms and sensations, and at the identity level because of recurring thoughts and emotions.
Breast cancer and self-transformation
The diagnosis of a chronic disease often leads to self-transformation or changes to one's own identity32–35 ; this is related to multiple factors associated with the illness experience, such as modifications to activities and lifestyle, reconfiguration of future plans, and the embodied experience of distortions of bodily functions. This is particularly true for oncologic diseases, breast cancer in particular.
Breast cancer and its related therapies frequently influence patients' identity and alter their self-conception. Perhaps, women undergoing radiotherapy could experience changes in their appearance, such as skin discoloration, soreness, and dermatitis 36 ; chemotherapy and hormonal therapy could cause hair loss, weight increase, and early menopause, abruptly reducing the possibility to become pregnant37–39 ; also, surgery may leave scars or even lead to removal of one or both breasts.40–42 In all these situations, body image is severely altered and, being closely related to self-identity, it may significantly affect individuals' self-esteem and the quality of social relationships.34,42,43 Another aspect usually heavily affected by cancer (and by treatments side effects) is sexual identity 44 : women who have or have had cancer report annoying sensations of missing parts, loss of sexual desire and pleasure, and loss of womanhood. 45 Common behaviors to cope with these symptoms and negative sensations include efforts to camouflage defects with hats or makeup, excessive grooming (e.g., hair combing), and changes of dieting and clothing. 46
Starting from these observations, we would like to see whether patients/survivors would create specific avatars referring to cancer experience, this way (a) providing additional evidence for the idea that avatars could be multiple and context specific, consistently with the multiple facets of the self; and (b) highlighting that, just like real/actual representations common in avatar research,11,13,14 also the experience of a chronic illness can be used as an independent source of information to represent a facet of the self.
To test how breast cancer affects avatar-conveyed multiple representations, we will ask a sample of patients to create avatars related to their AS and IS, as often carried out in the literature,12,14 and to the experience of cancer as well. As dependent variables, differences in attitudes toward the avatars will be analyzed, as previously carried out in avatar research on healthy individuals.6,9,47,48 Research hypotheses are as follows:
Second, it is possible that attitudes toward avatars, reconceptualized as attitudes toward representation of one's multiple selves, would be related to clinically relevant states, such as anxiety and depression. Anxiety is defined as a distressing emotional state, and a relevant hallmark of psychopathological conditions (e.g., anxiety disorders).
49
Research investigated the relation between avatars and anxiety in the field of social anxiety, showing that interaction between avatars could elicit such state in patients.50,51 Depression is a psychopathological condition characterized by low mood, anhedonia, fatigue, or low energy.
52
Research explored the use of embodied conversational agents in depression self-management,
53
but no research explored the relation between user-customized avatars and depression. For these reasons we introduced two explorative research questions:
Methods
Sample
Twenty-two women who had breast cancer diagnosis in the last 3 years and undergone treatment participated in the study. Age range was between 34 and 61 years (mean = 49.4, standard deviation = 7.73). They have been recruited by invitation among patients treated at the European Institute of Oncology, Milan, Italy. They were required to have access to an Android mobile device and give their informed consent to participate in the study, which was approved by the hospital ethical committee.
Procedure
Data collection was performed through an online platform, which participants accessed in their own personal devices. First, they received detailed instructions to create three avatars using a mobile application; these avatars resembled AS, IS, and self with cancer; participants had continual access to researchers' support if they encountered any difficulty in using the platform and/or creating the avatars, and had to send back the avatars to the researchers by saving them as images and using a dedicated e-mail address on a secure server; codes have been used to ensure participants' privacy. In the end, participants filled-in three questionnaires, one about their attitudes toward their own avatars (ordered randomly), and the other two on depression and anxiety.
Materials
Participants created their three avatars using the free mobile app Profile Avatar Maker 2 (Google Commerce Ltd., 2017) that allows the user to choose several aspects related to the digital figure, such as gender, and more specific details such as face physiognomy and emotional expression, hair and eyes, clothes and accessories, and background.
After the avatars creation, each participant responded to a questionnaire in which researchers had pasted the figures of their own avatars in a random order. This questionnaire consisted of three items per avatar rated on a 7-point Likert scale from 1 to 7, asking to evaluate each avatar regarding its attractiveness, its self-representativeness, and the difficulty experienced in creating it; then, participants were asked to evaluate the emotional state elicited by each avatar in its intensity, pleasantness, and dominance (again on a 1–7 Likert scale). These variables were previously used in avatar research.4,9,13,54,55 Given that participants were exposed to multiple questions and these had to be kept to a minimum, attractiveness and representativeness were chosen to give a comprehensive view of participants' attitudes (i.e., external looks and self-similarity), whereas difficulty in customization was used to control for participants' reaction to the avatar creation process. Finally, as emotions are considered fundamental to analyze subjective representation of illness, 56 we implemented an emotional self-report based on hedonic valence, arousal, and dominance that is believed to provide more complete information on emotional state as a whole than asking to rate intensity of categorical emotions.57,58
Once the questionnaire was completed, patients filled-in the Depression Patient Health Questionnaire-9 (PHQ-9) 59 , composed of 9 items rated on a 4-point Likert scale, a scale used for the assessment of depression diagnosis, its severity and monitoring; reliability in the present sample was 0.91. Finally, they completed the Anxiety Generalized Anxiety Disorder-7 (GAD-7), 60 which consisted of 7 items rated on a 4-point Likert scale, a scale used for the assessment of anxiety, its severity and monitoring. In this sample, the GAD-7 had a reliability index of 0.89.
Results
Analyses are as reported hereunder:
Descriptive Statistics and Comparisons Between Attitudes Toward Avatars (MANOVA)
p < 0.01.
AS, actual self; IS, ideal self; MANOVA, multivariate analysis of variance; SD, standard deviation.
Individual Comparisons Between Attractiveness, Self-Representativeness, and Emotional Pleasantness Attitudes Toward Avatars
p < 0.01.
CI, confidence interval.
Given that the sample was on the small side, it was impossible to run covariance analyses. To assess possible links between attitudes toward one's own avatars and clinically relevant states (i.e., depression and anxiety), correlations were performed (see Table 3 for correlations among all the study variables).
Correlations Among Investigated Variables
p < 0.05.
p < 0.01.
GAD, generalized anxiety disorder; PHQ, Patient Health Questionnaire; SWC, self with cancer.
Regarding RQ1 and RQ2, AS attractiveness and emotional intensity seem inversely correlated with both anxiety and depression scores; AS emotional pleasantness seems inversely correlated with depression score.
Discussion
This contribution presents preliminary results on avatar-mediated self-representations by breast cancer patients. According to literature, people tend to have multiple self-representations that may be activated by different experiences or circumstances23,61,62; this is reflected by the possibility for virtual environments and social media users to create multiple avatars, depending on the context they expect to enter, and/or on the facet of self-representation that is primed by the experimental manipulation.4,10,27 By analyzing attitudes toward one's own avatars, the results showed that breast cancer patients have representations of the self that are strictly connected to the experience of the disease, which is coherent with the rich literature on breast cancer effects on identity and the self34,63,64; these cancer-related self-representations can be represented in avatars. Cancer avatars are certainly perceived differently from other self-representations, and they are associated with negative judgments and unpleasant emotions. However, breast cancer survivors do not experience more difficulty in exploring this facet of self-representations than others, maybe because they have undergone such intrapersonal process already while fighting cancer. 65 However, correlations show that differences in attitudes toward one's own avatars can be related to clinically relevant states. Indeed, depression and anxiety seem inversely related to positive attitudes (pleasantness, intensity, and attractiveness) toward the avatars representing AS that corroborates the relationship between depression/anxiety and poor self-worth,66–68 and the possibility of using avatars to gather information on users' self-perception.
Figure 1 includes some examples of avatars created by the participants, which anecdotally show cancer-related avatar features and the differences between multiple self-representations.
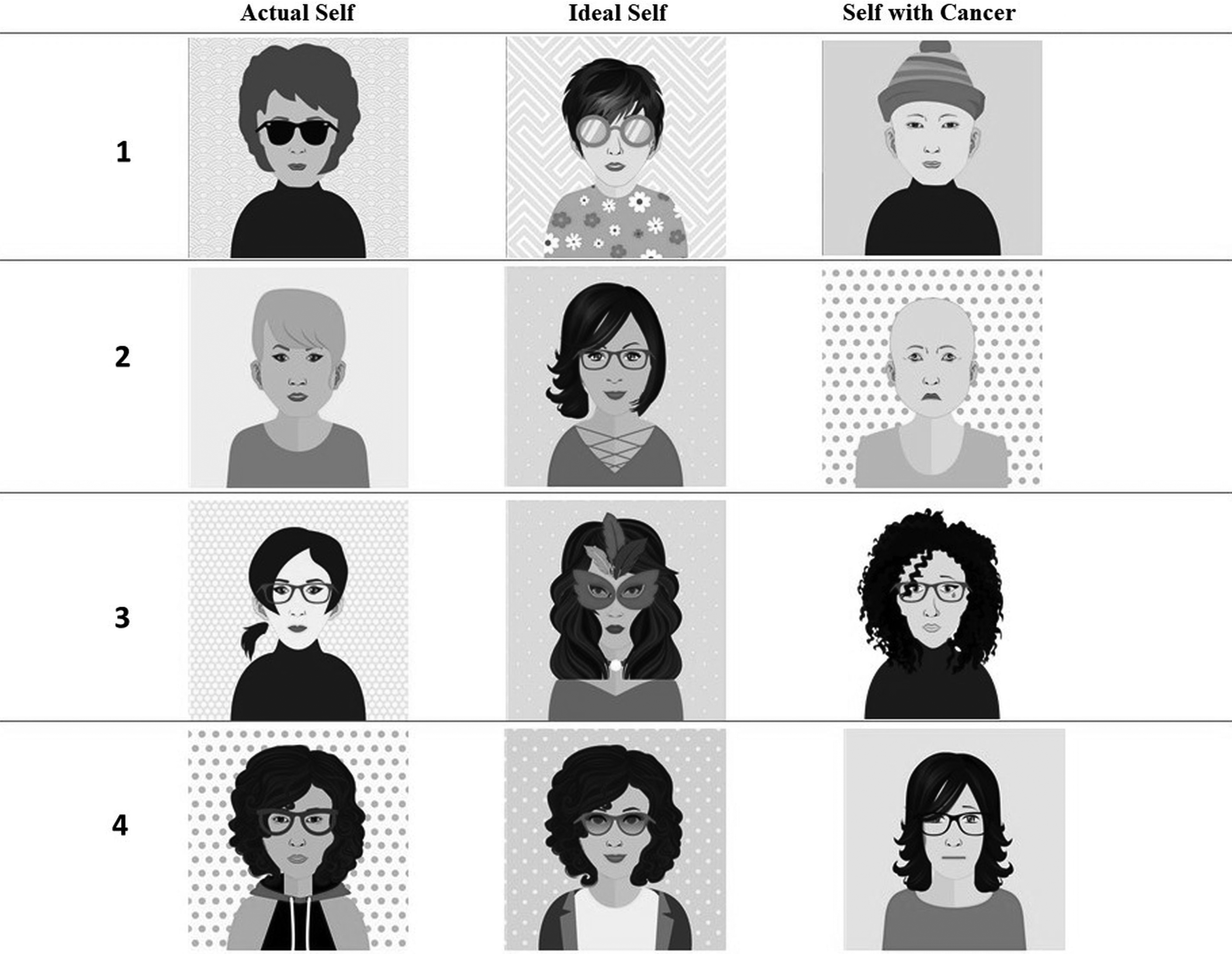
Examples of avatars created by some of the participants to show the readers how the patients' self-representations vary between actual self, ideal self, and self with cancer.
This study should be seen as a preliminary exploration: the sample is on the small side, because of the difficulty to recruit women having comparable experiences (surviving breast cancer) who accept to participate in such kind of “creative” task, have access to appropriate device, and adequate competence in digital technologies; no objective measures of avatars' features were possible because of the simplicity of the avatar creation platform, rather, for now, we only focused on attitudes toward avatars. Another limitation is related to the lack of a dedicated measure to control for participants' ability and satisfaction in avatar creation for different facets of the self. Future research should explore more complex and objective avatar-related variables, and their relationship with clinically relevant states (e.g., anxiety and depression, and also severity of physical and psychological symptoms), and personal traits and abilities (e.g., coping). In addition, future studies could compare ill and healthy participants to analyze whether avatars' characteristics and attitudes toward them could differ basing on the experience of a disease.
Although this study is only a first step, it is possible to prefigure two possible interesting aims for future avatar research: first, deepening avatars' possible usage as additional tools for psychological assessment, by continuing to explore their relationship with multiple self-representations and clinically relevant states, thereby empowering medical treatment's consideration of psychocognitive factors 69 ; second, informing eHealth and positive technology applications (i.e., technologies for promoting health and well-being) on how to use avatars not only as secondary add-on, but as tools for helping patients to express their inner states, and their personal representations of disease, treatment, and health.
Footnotes
Acknowledgments
Lucrezia Savioni and Valeria Sebri are PhD students within the European School of Molecular Medicine (SEMM).
Author Disclosure Statement
No competing financial interests exist.