
Abstract
This study determines the feasibility of using virtual reality (VR) for residents with and without dementia in the residential aged care (RAC) environment (also referred to as nursing homes or long-term care). A mixed-methods study was conducted with 13 residents of varying cognitive capacity in a residential aged care facility (RACF) operated by a not-for-profit organization in Brisbane, Australia. Residents participated in one facilitated VR session, either as a group or individual session. Residents' mood and apathy were measured by the Observed Emotion Rating Scale (OERS) and the Person–Environment Apathy Rating Scale. Residents also completed a structured interview to provide their feedback after the VR session. In addition, four RACF staff members were interviewed about their experience of using the VR in residents and the ongoing feasibility. The experience of VR administered by a researcher and leisure and lifestyle coordinator as a leisure activity, significantly reduced apathy in residents (Z = −2.818, p = 0.005) through observations of increased facial expression, eye contact, physical engagement, verbal tone, and expression. The study did not find a VR impact on the OERS measures; no significant increase in fear/anxiety was observed. Reminiscence was clearly observed in six of the nine residents with the ability to verbally communicate. VR was found not to be helpful in residents during episodes of acute neuropsychiatric and behavioral symptoms. This study suggested feasibility of using fully immersive VR delivered by mobile phone technologies. It provides preliminary data for a controlled trial presently underway examining the effectiveness of VR as a group activity in RAC to improve mood states, behavioral symptoms, and pro re nata psychotropic medication use. Residents indicated that VR was enjoyable with low levels of physical and emotional discomfort reported or observed.
Introduction
Residential aged care (RAC) facilities provide long-term care for older people in an institutionalized setting. Transition to RAC is a life-changing event that has significant implications for residents' daily routines, social networks, and autonomy. 1 Leisure activities comprise a number of discretionary activities and may contribute to greater adaptation to life within RAC because of increased relatedness and self-determined motivation. 2 Engagement in enjoyable leisure activities underpin residents' enjoyment of daily life, 1 and has been shown to reduce depression 3 and improve life satisfaction through improved cognitive function, self-perceived health status, and functional ability. 4 A number of leisure activities have been shown to benefit residents in RAC. Psychosocial interventions such as cognitive stimulation, cognitive behavior therapy, reminiscence therapy, sensory stimulation, and tailored activity programs have been found to be successful in RAC at improving cognition, reducing problematic behaviors, or contributing to improved mental wellbeing, as have some cultural arts interventions. 5 The addition of tailored leisure activities suitable for both residents with and without dementia is therefore of special interest to most person-centered RAC facilities.
Virtual reality (VR) has recently gained traction as a novel leisure activity suitable for the RAC environment. In the past two decades VR has been used in a variety of health care and aged care settings to enhance the ability to perform activities of daily living in patients with dementia, stroke, and Parkinson's disease6,7(Thangavelu K, et al. Unpublished work. Designing VR treatment for anxiety in older adults living with Parkinson's Disease: integrating literatures to inform next steps). The use of VR and gaming systems to enable physical activity has also been tentatively explored in older adults.8,9 However, only recently has the use of immersive VR experiences in RAC been identified as a possible avenue to improve resident quality of life. Previous research into the use of VR in people with dementia or cognitive impairment as a sensory experience,10,11 or to provide attentional 12 or memory-based 13 training, provides further evidence of possible feasibility in the RAC setting.
The development of a suite of VR videos specially targeted toward aged care has the potential to provide RAC staff with another tool in their arsenal to engage residents by providing them with a pleasurable immersive experience. Previous research has shown that limited activity choices, impaired physical functioning, resources, and transportation, are major barriers to residents participating in leisure activities. 14 The use of VR technology to provide unique three-dimensional immersive experiences to “transport” users to other environments voids the need for transportation, physical mobility, and ongoing costs. VR has previously been explored in a hospital-based setting and found to elicit positive responses with minimal discomfort. 15 This study undertakes a similar immersive VR technology in RAC to measure and describe the effectiveness of fully immersive VR on engagement and apathy in residents with and without dementia in an RAC environment. This study also aims to explore the feasibility of implementing such technologies as usual care in RAC. This study uses a library of videos consisting of relaxing scenes, such as underwater themes, beaches, farmyard animals, travel destinations, and snowscapes.
Methods
This mixed-methods study conducted between March and April 2018 (data collection) consisted of quantitative validated observer tools, a resident feedback survey, and staff interviews.
Human research ethics approvals were obtained from the University of Queensland (2018000022) and UnitingCare Queensland (21317).
Participants
Written consent was obtained from participants that was determined to have a Psychogeriatric Assessment Scale (PAS) of 4 or <4 (indicating no or minimal cognitive impairment). For residents with a PAS score of >4, substituted written consent was obtained from their legal guardians. Assent before each VR session was obtained from every resident. Residents were drawn from a 56-bed residential aged care facility (RACF) and had a range of cognitive and verbal capabilities. Families and residents were made aware of the program through advertising and an opt-in approach was undertaken. The program was open to all residents, where a signed consent form could be obtained.
Residents were aged between 66 and 93 years with a mean of 82 ± 8 years. There were nine female and four male participants. There were nine participants with dementia and all participants had some level of cognitive impairment. Four residents had mild cognitive impairment, two had moderate impairment, and seven had severe impairment. The mean time residents had spent in the RACF was 21 months (range: 3–58 months). Residents were excluded if they had symptoms or a diagnosis of contagious conditions, serious ill health, or were in palliative care. Residents were required to be seated for the VR experience; therefore, residents who were bed bound and unable to sit up were excluded.
Intervention
A Samsung Galaxy S7 (weight = 152 g), preloaded with an aged care VR library, in tandem with a Samsung Gear VR headset (weight = 345 g) was used to create a fully immersive VR experience for residents. The phone was inserted into the headset and applied to the residents face with both a horizontal and vertical Velcro strap to secure the device safely and distribute the weight. Straps were adjusted to fit each individual's face. The 360-degree videos contained within the library consisted of relaxing scenes, such as underwater themes, beaches, farmyard animals, travel destinations, and snowscapes that were specially created for the aged care industry. These videos lasted between 4 and 5 minutes each, with the perception changing in response to the viewers head movements. Scenes also consisted of relaxing background music and narration about the relevant scene. An image of the main menu for the application is given in Supplementary Figure S1. Residents were engaged in one VR session in an individual or a small group session while at rest. Sessions were run by the leisure and lifestyle coordinator, to provide a relaxing and engaging leisure activity, with documentation completed by the research coordinator. Attempts were also made to implement VR as a diversion therapy in response to acute disruptive behaviors, distress, or agitation at the time of presenting symptoms. This was facilitated by two registered nurses (RNs) within the facility, and proved unsuccessful because of practical limitations such as staffing and time delays, and resident factors such as agitation.
Residents were monitored for any symptoms or signs of cyber sickness including general discomfort, fatigue, headache, eye strain, difficulty focusing, increased salivation, sweating, nausea, difficulty concentrating, fullness of head, blurred vision, dizziness, vertigo, stomach awareness, and burping. 16 Residents were also monitored for fear and anxiety using the observational tools described hereunder and for physical discomfort of the device. To reduce the risk of cyber sickness the technology used did not contain sudden scene changes, all residents were seated throughout the experience, and residents with deteriorating ill health were excluded. In cases where the resident was observed to have symptoms or signs of cyber sickness the device was removed immediately and the resident was monitored by care staff over the course of the day. Where residents reported physical discomfort, the device straps were readjusted. In cases where the VR elicited a negative emotional response, a different scene was trialed, with resident assent, to determine whether it was the particular scenery experience or the VR experience itself that caused a negative response.
Procedure
(a) Researcher observed the residents for 10 minutes before the VR experience and administered baseline emotion and apathy measures using the Observed Emotion Rating Scale (OERS) and Person–Environment Apathy Rating Scale (PEARS), respectively.
(b) Facilitator (Lifestyle Coordinator, RN, or personal carer) set up the VR program/application based on resident's profile/preference (facilitator asked resident to choose their preferred scenery).
(c) Facilitator informed the resident about the procedure and what to expect.
(d) Facilitator applied the VR headset for fully immersive VR experience.
(e) Facilitator facilitated engagement by asking questions. For example:
-What do you see?
-What do you think of the view?
-Have you visited a place similar to this?
(f) Facilitator informed the resident at least 1 minute before the session ends and explained what the facilitator will do next. Facilitator also provided prompts to reduce simulator sickness for example, closing eyes before removal and slowly opening eyes to adjust to change in lighting.
(g) Facilitator asked/observed for simulator sickness and asked the participant about the experience.
(h) The headset was wiped down with alcohol wipes between residents for hygiene reasons. Residents presenting with flu-like or gastrointestinal symptoms were excluded to avoid cross-contamination.
Researcher observed the session and completed the OERS, PEARS, and qualitative feedback questionnaire with the resident after the session.
Data collected
Data were collected by the research coordinator, in collaboration with the leisure and lifestyle coordinator at the RACF by verbally discussing responses during observation. This was important as care staff with close relationships to their residents are able to identify usual behaviors and emotions expressed by the resident and divergences from these norms. There was no disagreement to responses between the two. Observational and qualitative data were recorded using the following methods:
(a) PEAR
17
apathy subscale was used to assess resident apathy before and during the VR session. Apathy was measured by observing six indicators: facial expressions, eye contact, physical engagement, purposeful activity, verbal tone, and verbal expression, on a 1–4 scale, with higher scores indicating a greater level of apathy. (b) The OERS
18
was used to measure residents' emotional response. Residents were observed for their emotional state using the OERS for 10 minutes before the VR session and for 10 minutes after. The tool allowed quantification of five observed emotions: pleasure, anger, anxiety/fear, sadness, and general alertness. Emotions were rated on a scale representing the frequency of the observed emotions over a 10-minute period (1 = never; 2 = <16 seconds; 3 = 16–59 seconds; 4 = 1–5 minutes; 5 = >5 minutes; and 7 = not in view). (c) Residents were asked a series of structured questions at the end of their VR session. Residents were asked to rate on a scale of 1–5 (1 = not at all, 5 = very much) their enjoyment, their success in navigating the program, their discomfort, and whether they would use the program again. In addition, residents were asked three open-ended questions: “What were the best aspects of the program? What were the worst aspects of the program? Where would you like to go next (using the VR)?” Resident responses were recorded verbatim on the resident feedback form. (d) Residents were observed for signs of simulator sickness. Signs and symptoms of simulator sickness were defined by the item on the Simulator Sickness Questionnaire.
19
Data analysis
Data analysis was conducted using SPSSv24. The Wilcoxon signed rank test was used to analyze pre–post changes in the OERS and PEAR scores because of the nonparametric nature of the variables. The sum of the individual subscales was used to measure total changes in emotion and apathy. An alpha level of 0.05 was used to determine significance.
Results
Thirteen residents completed observed VR sessions. Residents with mild to moderate cognitive impairment completed the tasks as a group in an allocated quiet area of the dining room. These residents were able to sit, observe fellow residents using the VR headset, and participate in group discussions. Residents with severe cognitive impairment were also given the opportunity to participate in a group setting; however, the majority declined because of the wait time of using the VR between other participants and preferred one on one attention with the leisure and lifestyle coordinator and research assistant. In these cases, VR was administered individually, either in the resident's room or in a quiet area of the dining room based on resident preference.
Apathy and emotion
The VR experience significantly reduced apathy in residents (Z = −2.818, p = 0.005) (Fig. 1). Total scores reduced from a mean (standard deviation) of 15.54 (±6.11) to 11.38 (±3.93). This was because of observations of increased facial expression (Z = −2.489, p = 0.013), eye contact (Z = −2.070, p = 0.038), physical engagement (Z = −2.887, p = 0.004), verbal tone (Z = −2.428, p = 0.015), and verbal expression (Z = −2.714, p = 0.007). VR did not significantly impact measures of the OERS; no significant increase in fear/anxiety was observed. A trend was observed for increased pleasure (Z = −1.725, p = 0.084) and general alertness (Z = −1.639, p = 0.101).
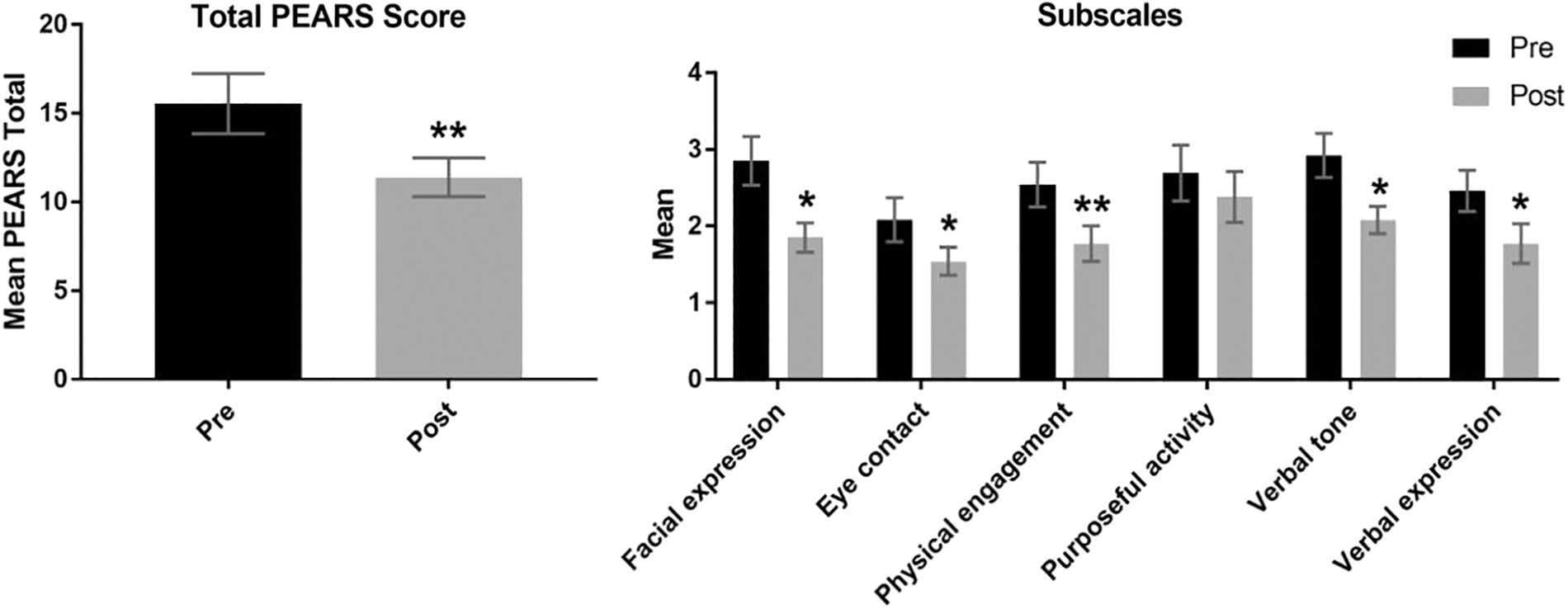
Changes in total mean PEAR apathy scores in response to virtual reality. *Significantly different from preintervention at p < 0.05. **Significantly different from pre intervention at p < 0.005. PEAR, Person–Environment Apathy Rating.
Resident experience
Ten of the 13 residents were able to participate in completing a survey of their experience, with 9 residents verbally responsive and 1 resident indicating scale responses with physical gestures. Scenes preferred by residents included a farmyard scene comprising goats and chickens, an underwater scene of the Great Barrier Reef, a beach scene, and a scene comprising penguins in the snow. Travel scenes of Bali, Merida and canoeing down a river were used to a lesser extent. One resident with visual impairment found that the scene of penguins in the snow was easier to observe because of the contrasting black and white. Scenes comprising animals or waterscapes dominated resident's choices.
All but one resident indicated that they wanted to experience the VR again. The resident that indicated that she would not like to use VR in the future stated that she was “just not that sort of person,” and was uninterested in the activity. Future experiences residents expressed were of interest to them were country areas of Australia, particularly those that had a link to their past, and the beach; for example, one resident stated that she “would love to wander through the country areas where it's peaceful.” Another resident indicated that they would love to see their hometown where they grew up and another wished to visit places where he had been stationed during their time in the Defense Force.
During the VR experience, reminiscence was also observed in six residents with the ability to verbally communicate.
Marvellous. It feels like you want to touch it. I'm milking goats. I used to milk goats, when I was younger (farmyard scene).
The colour. It seemed so natural to me because I lived down there. It was lovely to see it (beach scene).
Residents indicated that VR was enjoyable with low levels of discomfort reported. Two residents with impaired vision reported that the scenery was blurring. Possible eyestrain and blurring vision was recorded as symptoms of cyber sickness. One other resident found that the headset was slightly uncomfortable and slid down their face because of the weight of the device. One resident who used the VR during an experience of acute behavior, and not in an individual or group session, reported that the VR made her feel “giddy,” which was temporary upon removal of the device. This was in interpreted by medical staff as an instance of cyber sickness and was closely monitored. Observances of emotion identified one resident with severe cognitive impairment as anxious at the onset of the experience. This was mediated by changing of the scenery from a water scene to a farmyard. These were the only adverse responses observed in this sample.
Discussion and Conclusion
This study highlights the feasibility of using fully immersive VR and mobile technologies in RAC, which has previously not been reported. Minimal side effects were observed and the results corroborate a recent finding from a nonimmersive VR study conducted in RAC facilities, reporting reductions in resident apathy. A pilot study conducted by Moyle et al., 11 into the use of a nonimmersive VR rendered forest scene in RAC facilities, revealed a reduction in PEAR apathy scores. However, unlike this study, a significant increase in anxiety/fear, pleasure, and general alertness were also observed. Participants in this study were not observed to suffer increased fear/anxiety, and increases in resident pleasure and general alertness did not reach significance, despite similar sample size to the previous study. However, the small sample sizes in both studies may have impacted the statistical significance of results.
This study contained participants with cognitive impairment with 9 of 13 diagnosed with dementia. Half the participants had severe cognitive impairment (n = 7), reflecting the typical make up of RAC facilities in Australia.20,21 This was important to determine the feasibility of VR in the typical aged care environment. There was no increase in adverse reactions in participants with severe cognitive impairment and the VR experience significantly improved apathy (Z = −2.207, p = 0.027) in this cohort. The inclusion of people with cognitive impairment resulted in the use of observer rated tools and the necessity for care staff known to the resident to be included in the procedure. Future research should focus on how VR can be tailored to participants with differing levels of cognitive impairment.
Qualitative results from residents revealed that VR was regarded as an enjoyable experience, one that most residents wished to do again. The experience provided some residents an opportunity to converse in a group setting, whereas others preferred one-on-one experiences. The flexibility of the VR program allowed for tailoring of the activity. Participants were able to choose their destinations. This is important, as personal autonomy in RAC is low, particularly in matters concerning residents' social life within the facility 22 ; it however, added a level of heterogeneity to the procedure. It is possible that group dynamics augment the experience of VR. Residents both with and without severe cognitive impairment enjoyed the experience, further highlighting the versatility of VR.
At the completion of this pilot study, VR was implemented by the leisure and lifestyle coordinator in an on-going manner at the participating site. Feedback from staff and residents indicated ongoing feasibility of VR technologies in aged care. A forthcoming controlled trial of group VR sessions will further explore the use of VR to improve mood and wellbeing within RAC (clinical trial registry ACTRN12618000749202).
Footnotes
Acknowledgments
The authors acknowledge the valuable input of Jean Moss, Mathew James, and Gurgit Bhuller for aiding in project implementation.
Authors Contributions
Two researchers were employed by the not-for-profit organization at time of data collection; however, the researcher responsible for data collection was employed by a separate department with no provisions on publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.