
Abstract
To explore whether individualized visual training improves the visual acuity and visual field defects of patients with glaucoma. Patients with established primary glaucoma who visited the glaucoma clinic of Beijing Shijitan Hospital, Capital Medical University from January 2018 to April 2018 were recruited. The binocular visual perception examination was performed by using the visual perception examination system, and a personalized training program was developed according to the relevant threshold conditions between the eyes of the patients. The binocular visual perception training session for 20 minutes for two sessions was completed at home by using a virtual reality helmet. The visual function, intraocular pressure, and Octopus visual field were examined, before and at the first month and the third month after training. Seven patients completed the study. None of the seven patients has fine stereopsis, four of them have large stereopsis, and two patients are without large stereopsis. The visual acuity at 3 months after training was significantly improved compared with that before training. The mean defect value after 1 month of training was significantly lower than that before training, and it was further decreased after 3 months. Similarly, the mean sensitivity value was significantly increased in both follow-ups after training. There was no significant difference in loss variance after 1 and 3 months of training when compared with that before training (p > 0.05). Our small prospective observational study indicated that individualized visual perception training can improve the visual function and improve the visual field in patients with glaucoma, and a large sample size study is warranted to further assess the value of this novel treatment.
Introduction
Glaucoma is an optic neuropathy characterized by progressive loss of the retinal nerve fiber layer and ganglion cell death, which ultimately damages the optic nerve. The primary treatment of glaucoma is to reduce intraocular pressure to prevent further damage to vision and the visual field with various approaches, including laser treatment or surgery. Without early detection, glaucoma causes permanent visual loss and visual field defects, and there is currently no treatment for patients with glaucoma to restore visual acuity and visual field damage, because such visual impairment and visual field defects are usually considered to be irreversible.
However, recent studies reported that the nervous system in eyes has significant neural plasticity. In animal studies, as long as 10 to 30 percent of retinal ganglion cells (RGCs) survive in the situation of optic nerve injury, up to 80 percent of visual function can be restored within 2–3 weeks by their own repairing capability,1,2 and these surviving cell bodies are moderately enlarged, which suggests that neural remodeling may have occurred.1,3 In addition, in the study of patients with age-related maculopathy, it was found that to adapt to the decrease of central vision, patients would replace the foveal vision by adjusting the area with parafoveal visual function and obtain useful vision by reconstructing with the cerebral cortex function, indicating that there is a large-scale visual reorganization or remodeling process in the cerebral cortex in response to the visual impairment caused by retinopathy. 4
Visual impairment in glaucoma progresses from RGC apoptosis and optic nerve damage to nerve damage in the lateral geniculate body, optic radiation, and cerebral cortex. This ability of the brain to remodel and regenerate itself underlies the neuroplasticity of visual perception. Visual reality perception may provide a novel approach to screen and treat visual function damage in glaucoma. Gudlin et al. performed visual restoration therapy (VRT) training in five patients with primary open angle glaucoma for 6 months, during which the interval was 3 months. The results showed that the ability of patients to perceive visual stimuli was significantly improved. 5 Sabel et al. also found that 15 patients with glaucoma who underwent VRT for 3 months had significantly improved visual fields and faster response times than controls. 6 No such studies has yet been reported from China.
In this study, the visual perception examination and training system developed by the National Engineering Research Center for Medical and Health Appliances was, for the first time, used to evaluate the visual perception function of patients with glaucoma. The improvement of visual acuity and visual field both before and after training was compared.
Materials and Methods
Study subjects
Patients with primary glaucoma who visited the glaucoma clinic of Beijing Shijitan Hospital, Capital Medical University from January 2018 to April 2018 were recruited.
Inclusion criteria: (a) Meet the diagnostic criteria of primary glaucoma [refer to the Expert Consensus on the Diagnosis and Treatment of Primary Glaucoma in China (2014)]; (b) There is glaucomatous visual field change 7 ; (c) Diopter power: sphere power −6.00 to +6.00D, cylinder power −3.00 to +3.00D, and anisometropia ≤2.00 D in both eyes; and (d) Able to cooperate with ophthalmological examination and follow-up, understand and accept informed consent.
Exclusion criteria: (a) High myopia, uveitis, maculopathy, diabetic retinopathy, and other ocular fundus diseases; (b) Retinal optic nerve disorders; (c) Central nervous system degeneration that may cause optic nerve degeneration; and (d) Intracranial space-occupying and other neurological diseases. The study was approved by the Ethics Committee of Beijing Shijitan Hospital, Capital Medical University, and the procedures were in accordance with the Declaration of Helsinki. Written informed consent was obtained from all study participants.
Methods
Visual field assessment
The threshold inspection procedure, dG2 procedure, of Octopus 101 automatic perimeter produced by Swiss company HAAG-STREIT is used. During the inspection, the pupil diameter of the subject is required to be ≥3 mm, and the appropriate corrective lens is selected. Reliable factor <15 percent results were considered to be reliable. The following changes were considered to be glaucomatous changes: (a) a decrease of 5 dB in visual sensitivity at three adjacent points, with a decrease of 10 dB at one point; (b) a decrease of 10 dB at two adjacent points; and (c) a difference of >10 dB in visual sensitivity between the upper and lower two points at the nasal level (7). At least the visual field test was done twice before enrollment, and the second or third more reliable visual field test result was selected as the baseline visual field of the patient.
Binocular visual function examination
Inspection equipment: LG2342p computer, 24-inch wide-screen polarized light display, and examination software developed by Guangzhou Medical Instrument Research Institute (Guangzhou, China). For each examination, the subject was seated, with both eyes equal in height to the midpoint of the screen, 80 cm apart, resolution 1920*1080, and wearing polarized glasses.
(a) Motion parallax stereo vision: background high-speed movement, the subject judges the opening direction of the E word in the diagram and clicks the corresponding button of the interface as the confirmation. Among them, the high-speed movement stereopsis inspection is relatively easier to detect, the low-speed movement stereopsis is more difficult to judge, and the correct rate is 100 percent.
(b) Large-scale rough stereoscopic inspection: The subject judges whether the visual mark in the figure is at the crest (protruded) or trough (concave in) and clicks the corresponding button to determine. The correct rate is 100 percent.
(c) Fine random dot stereoscopic inspection: a random dot distribution map (54 cd/m2) with a gray background (44 cd/m2), with a size of 5° × 5°, and an E optotype (3° × 3°) consisting of random dots in the central part of the map with non-zero disparity of 400, 300, 200, and 100, respectively, with peripheral dots as a reference and always relative zero disparity. Wear split view lens, judge the opening direction of E-word in the figure, press the arrow keys of the keyboard, or click the corresponding button on the interface as confirmation. There were four pictures, which were divided into 400′′, 300′′, 200′′, and 100′′, and they were judged to have fine stereopsis as long as they could perceive between 400′′ and 100′′.
The binocular visual function training
The binocular visual function training adopts the binocular visual function push-pull model training method provided by the National Research Center for Medical and Health care Appliance Engineering Technology. Through the series of binocular visual perception examination mentioned earlier and short-term plasticity examination of about 5 to 10 minutes, the threshold point parameters of different types of stereoscopic vision of patients are obtained.
Then, using the engineering realization means of virtual reality, based on the balance of binocular stereopsis function perception, more precise energy suppression (sine disappearance) is performed on the relatively better eye of the patient in time, and energy enhancement (strong flicker) is performed on the worse eye. The better eye was spatially filtered (contrast reduction), and the worse eye was filtered and enhanced (spatial frequency low-pass filtering).
Patients wore a virtual reality binocular separation tool and performed individualized push-pull model training on time, once a day for 20 minutes.
Baseline examination and follow-up
Baseline examination and follow-up of the enrolled patients with routine ophthalmology (visual acuity, best-corrected visual acuity, 24-hour intraocular pressure, anterior segment, fundus, optical coherence tomography, and other examinations) and glaucoma routine examination (24 hours intraocular pressure curve examination, Octopus visual field examination), the use of the National Research Center for Medical Devices Engineering Technology developed a visual perception examination system for binocular vision, according to the examination to develop a personalized brain vision training strategy, wearing polarized glasses at home to complete 20 minutes training twice. During the first and third month after training, the visual function, mean intraocular pressure, and Octopus visual field test were measured, and the changes of parameters before and after training were compared.
Statistical analysis method
SPSS 16.0 was used for statistical analysis. Visual function, mean intraocular pressure, mean sensitivity (MS), mean defect (MD), and loss variance (LV) values before training, 1 and 3 months after training were analyzed by paired t test or Wilcoxon test; the results of binocular visual perception examination were analyzed descriptively. p < 0.05 was considered statistically significant.
Results
A total of 21 patients were enrolled in the study; of those, 12 either did not complete the training on time or were lost to follow-up, and 2 were unable to adhere to training because of dry eye symptoms. In the end, data from 7 patients (14 eyes) (5 males and 2 females aged: 47.29 ± 10.32 years old) were analyzed and reported. Patients' general characters are shown in Table 1.
Clinical Data of Enrolled Patients
POAG, primary open angle glaucoma; SLT selective laser trabeculoplasty; C/D cup/disc ratio.
None of the seven patients has fine stereopsis, four patients have large stereopsis, and two patients have no large stereopsis.
There was no significant difference in visual acuity between patients before and 1 month after training (p = 0.066), but visual acuity was significantly improved 3 months after training when compared with that before training (Fig. 1). No significant difference was found in intraocular pressure during the follow-up period (p > 0.05) (Fig. 2).
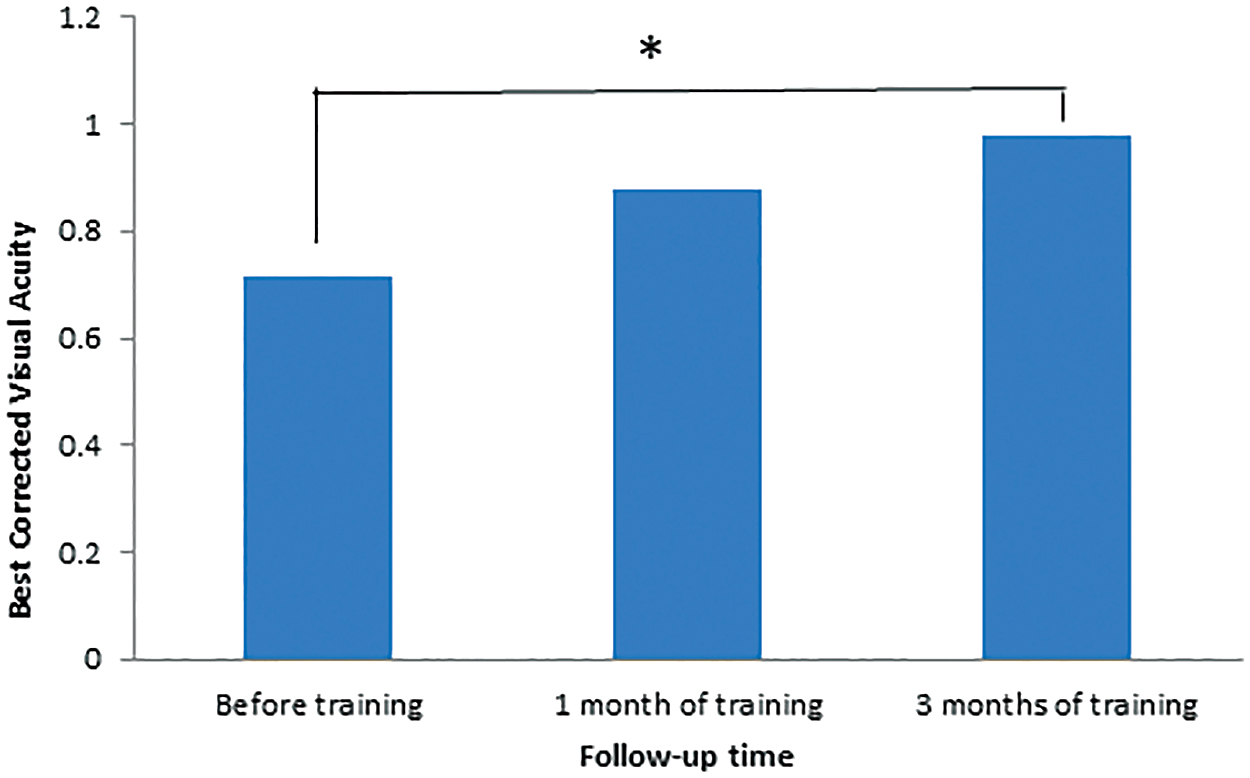
Comparison of patients' best-corrected visual acuity during follow-up. *The best corrected visual acuity after 3 months of training was statistically significant compared with that before training. Color images are available online.

Comparison of intraocular pressure of patients during follow-up. Color images are available online.
Comparison of the changes in pseudocolor maps of Octopus perimetry in 14 eyes of 7 enrolled patients is shown in Figure 3. The changes in MS, MD, and LV values are shown in Table 2. Among them, the MD value after 1 month of training was significantly lower than that before training, and the MD after 3 months of training was significantly lower than that after 1 month of training; similarly, the MS value increased in both follow-ups after training, and the difference was significant.

Comparison of pseudocolor perimetry before and after binocular training in seven patients with POAG. POAG, primary open angle glaucoma. Color images are available online.
Comparison of Visual Field Parameters (Mean Defect, Mean Sensitivity, and Loss Variance) Before and After Training
MD, mean defect; MS, mean sensitivity; LV, loss variance.
There was no significant difference in LV after 1 and 3 months of training compared with that before training (p > 0.05).
Discussion
Visual recovery in glaucoma does not refer to restoration of absolute blindness, but to activation of residual vision. The residual visual acuity is mainly located at the boundary of visual field defect. There is a residual area of visual acuity (ARV) between the complete visual field area and the damaged area. Clinical studies and animal experiments have found that this area has plasticity and is the target area for therapeutic intervention. 8 German scholars Kasten and Sabel et al. developed a computer-based training method, called VRT, and it was marketized by NovaVision, Germany, and gradually promoted in European countries and the United States.8–11 The key of VRT is to find out the patient's ARV through HRP detection and perform a lot of repeated stimulation, and the patient responds to the perceived stimulation. The visual field can be expanded by an average of 5° in two-thirds of patients after training, whereas the other third of patients do not respond to treatment. 8 The VRT training is a stimulation training for one eye.
The visual stimulation training developed by the National Engineering Technology Research Center for Medical and Health Appliances used in this study is aimed at the stimulation of both eyes, repairing the low-level channels from the advanced channels between the two eyes, using the plasticity and mobility of the brain's nervous system, activating the visual signal pathway through personalized visual stimulation and visual learning, and improving the signal processing ability of the brain's nervous system, so as to achieve the purpose of treatment. 12 This training method has been applied with some success in the fields of pediatric amblyopia and refractive error.13,14 However, there is no report on how to restore the visual information transmission and improve the visual function and visual field of glaucoma patients through visual perception stimulation remodeling.
No relevant studies on fine stereopsis function in patients with glaucoma have been reported, and this study found that none of the seven enrolled glaucoma patients had fine stereopsis function.
This study found that the stimulation function of binocular vision can improve the visual function of glaucoma patients to some extent. In the study, the best corrected visual acuity of eight eyes in seven patients showed different degrees of improvement at 1 or 3 months after training. We speculate that this is related to the improvement of signal processing efficiency of the brain nervous system by binocular vision training. This study did not find that the training can affect intraocular pressure.
In this study, we found that the MD value of the visual field in patients with glaucoma after 1 month of training was significantly lower than that before training, and the MD value continued to decrease after 3 months of continued training. MD value is a sensitive index to reflect the diffuse visual field defect. Through training, patients with glaucoma can improve the diffuse visual field defect to some extent. MD values continue to improve with prolonged training, and we speculate that visual field defects in glaucoma patients can be improved by long-term training. MS values also changed significantly before and after training, and they increased significantly after 1 and 3 months of training. Through the change of MS value, we speculated that retinal light sensitivity could be increased by brain vision training. However, there was no significant change in LV values after 1 and 3 months of training, which may be related to the small sample size. In the future, the sample size should be increased to better analyze the indices of visual field.
Through the pseudo-color map (Fig. 3), the changes in visual field before and after training can be visually reflected, such as the changes in the visual field of patient three and patient seven are particularly obvious, and the visual field improvement area usually appears at the edge of the visual field damage area, which is also consistent with the theory of ARV. 8
There are certain limitations of our study. First, this study has a small sample size and the patients have mostly advanced glaucoma. In the future, we should also increase the sample size to explore the training effect of different periods of glaucoma. Second, there is no control group in this study, and we cannot exclude the Hawthorne effect. For example, patients with glaucoma may get more attention from the researchers to improve the examination results. Third, functional magnetic resonance imaging has been reported to show brain remodeling in both cortical and pericortical areas after visual stimulation in patients with acute optic neuritis, 15 but the damage site of the visual information transmission network system from the retina to the visual cortex in patients with glaucoma in different periods is not clear.
Conclusion
Although this study is a small sample study, through a personalized closed-loop type of binocular vision test and training, the results show that it can improve the visual acuity and the visual field defect of patients with glaucoma to a certain extent, which provides a new idea for the treatment of glaucoma. International research has been done to try to treat glaucoma through monocular personalized precision stimulation and brain bio-enclosed loops5,16 and those results are promising. The previous studies and our current study strongly suggest that individualized visual perception training gives a hope to improve the visual acuity and the visual field defect of patients with glaucoma; therefore, a large sample size study is urgently needed to further assess the value of this novel treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Beijing Municipal Administration of Hospitals Clinical Technology Innovation Project (XMLX201808); Youth Fund of Beijing Shijitan Hospital (2017-q47); Major Special Fund of Guangdong Province (2017B010110013).