
Abstract
Acute and chronic psychological distress are prevalent during adolescence and can have negative impacts on adolescents in all life domains. The aim of this systematic review was to appraise the use of virtual reality (VR) interventions to manage symptoms of psychological distress symptoms among adolescents. MEDLINE, PubMed, PsycINFO, and Scopus databases were searched up to June 2020. Available citations were de-duplicated and screened by two authors using title and abstract information. A total of 301 articles were retained for full-text evaluation next to eligibility criteria. Empirical studies of all designs and comparator groups were included if these appraised the impact of an immersive VR intervention on any standardized measure indicative of psychological distress in an adolescent sample. Data were extracted into a standardized coding sheet. Results were tabulated and discussed with a narrative synthesis due to the heterogeneity between studies. A total of seven studies met inclusion criteria. There were four randomized controlled trials and three uncontrolled pilot studies on new VR interventions. Distress-related issues included: state-anxiety, venepuncture, risk taking, public speaking anxiety, social anxiety disorder, sexual victimization, and chemotherapy administration. All studies reported significant changes on outcome measures after VR treatment. Six studies reported small-to-large reductions in symptoms. The average attrition rate was 3.6 percent during the active VR treatment phase. Treatment acceptability was high in the studies that assessed user engagement factors. The VR technology can provide a safe, rapidly efficacious, and acceptable treatment modality for managing psychological distress in several key adolescent populations.
Introduction
Acommon mental health challenge for adolescents is psychological distress.1–4 This can be construed as a transient state of emotional suffering that broadly includes any combination of negative mental symptomology (e.g., depression, anxiety, and perceived stress).5,6 Psychological distress can arise from negative life events such as physical health problems, 7 relationship difficulties,8,9 and environmental issues.10,11 Neurocognitive development in adolescents, where the emotional brain matures before the regulatory capacity of the prefrontal cortex matures, is seen as an additional contributor to the experience of distress. 12 This distress is often associated with somatic complaints such as pain, fatigue, heart palpitations, breathing difficulties, nausea, and other unpleasant bodily symptoms. 13 Psychological distress can significantly impair daily functioning and life quality, both chronically and acutely. 6 For instance, adolescent psychological distress from school bullying has been linked to restrictive eating, 14 sleeping difficulties, 15 school absenteeism, 16 self-injury, and suicidality. 17 Acute distress may arise as a response to unexpected or distressing environmental events such as vaccination and other painful medical procedures. Therefore, it is essential to help adolescents suffering from psychological distress with evidence-based mental health interventions. 18
Virtual reality (VR) provides one treatment modality for mental health issues.19,20 It involves the use of immersive computer technology (e.g., stereoscopic headsets, motion sensors, and haptic feedback devices) to imbed users into interactive digital worlds. 21 This can induce “presence,” a cognitive state of being deeply connected and engaged in the VR world. 21 Empirical evidence indicates that immersive VR interventions can therapeutically distract people from painful and distressing real world experiences,22,23 induce relaxation with calming virtual environments, 24 and provide mental health skill training with virtual avatars. 25 Participants can learn to overcome anxiety-related disorders with VR exposure therapy (VRET), presenting digital representations of real-life distressing stimuli. For instance, moderate-to-large effect sizes in symptom relief have been reported for VRET compared with waitlist and placebo control conditions.26–28 This level of treatment effectiveness is comparable to traditional cognitive behavioral therapy and in vivo exposure.26,29 Overall, VR appears to be a promising health care tool for managing psychological distress. However, some limitations have been identified.
The VR has potential ethical, health, and safety risks. 30 These can include physical injuries from poor posture, repetitive strain, user collisions with real-world objects, and particularly in health settings, discomfort with headsets, infection control, and risk of inducing epileptic seizures and migraine headaches.19,30–33 The VR may cause “simulator sickness,” a physiological condition consisting of nausea, disorientation, and oculomotor difficulties.34,35 There are also concerns about negative mood changes. 30 For instance, VRET stimuli may be too anxiety provoking and lead to participant dropout. 29 However, Benbow and Anderson 36 found that VRET attrition is not significantly different to in vivo exposure. Further, deterioration is less likely in VRET patients compared with waitlists. 37 When looking at safety outcomes, a recent review on VR interventions for distressed burn victims found little-to-no negative side effects. 23 Nevertheless, VR use may be problematic for some people depending on individual characteristics, specific technology, and virtual task requirements.30,34 Therefore, user engagement factors are important to consider when determining populations that are suitable for VR interventions.
The aim of this systematic review was to appraise the empirical status of VR interventions for managing psychological distress among adolescents. Prior VR mental health research has predominately focused on adults,29,37,38 or mixed age samples of youth and adults.23,39,40 Adolescents are developmentally distinct from young children and adults in their neurocognitive, psychosocial, and physical development. 41 They face unique life challenges related to puberty, schooling, self-identity, intimate relationships, and financial dependencies. 41 Clinically, adolescence is a critical period for the onset of mental health disorders.42,43 It is, therefore, important to evaluate how VR has been used to manage their distress on key factors of effectiveness, acceptability, and adherence. Further, an up-to-date account of the evidence base in this domain is warranted, as VR is a rapidly evolving field with new technological advances being made in hardware and software capabilities.21,44,45 By synthesizing extant research findings, it will be possible to identify effective and engaging VR interventions for adolescent psychological distress. This information can help guide future efforts when researching and implementing VR in health settings.
Method
This systematic review was conducted by using the PICO (patient/population, intervention, comparison, and outcomes) framework and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 46 The protocol of this systematic review was prospectively registered in the PROSPERO international database (CRD42020198984).
Search strategy
The following electronic databases of scientific research were extensively searched: PubMED, MEDLINE, PsycINFO, and Scopus. Keywords used to search each database were: ((virtual reality or VR) and (child* or adolescent* or pediatric* or youth or teen* or high school or juvenile) and (depress* or anxiety or stress or distress or phobia or fear or pain or anger or frustration or well-being or mental health)). The reference lists of included papers were also manually searched.
Eligibility criteria
To be included in the review, articles needed to meet the following criteria. Based on the World Health Organization 47 definition of adolescence, an age range of 10 to 19 years was specified for participants. If the data set contained participants who were older or younger than the age range of interest, their data were only used if subgroup analysis was available or if adolescents made up greater than 50 percent of participants. The VR intervention under investigation needed to be delivered through a head-mounted display (HMD) hardware system. This is the most widespread and affordable form of immersive VR technology.21,44,45,48 Empirical studies of all research designs (e.g., randomized controlled trials [RCT], nonrandomized studies, quantitative descriptive studies) and all comparators (e.g., waitlist control, active intervention, no treatment concurrent control) were included. This criterion was set to ensure that the review was comprehensive. The studies were required to report on empirical outcomes obtained from any standardized measure indicative of psychological distress (e.g., depression, anxiety, traumatic stress, anger, frustration, or other negative mood states). This criterion was set to ensure the psychometric validity and reliability of the reported VR intervention outcomes and to ensure a broad range of potential distress-related conditions were included. Articles were restricted to those written in the English language and published in peer-reviewed journals from January 2005 up to June 2020. This time frame was set to ensure that modern VR technology was evaluated. 21
Article selection
After de-duplicating search results, two researchers (J.K. and B.R.) scanned the remaining article titles and abstracts. Promising articles were retained for full-text appraisal. Study inclusion was then determined by both researchers using the eligibility criteria. Divergent views on inclusion were resolved through discussion and mutual agreement.
Data extraction
Data from included studies were extracted by one reviewer (J.K.) into a standardized coding sheet and then checked by a second reviewer (B.R.). Data items extracted for synthesis included the following:
Reference source: first author surname, year of publication, and title. Participants: distress issue, clinical status, sample size, age, sex, and country. Methodology: study design, comparator trial arms, measurement points, and study quality rating. VR intervention: name, software, hardware, treatment purpose, treatment length, and therapist guidance. Treatment efficacy: distress measures, outcomes, and effect sizes. User engagement: attrition rate, treatment satisfaction, and intention-to-treat analysis.
Attrition in this review was defined and measured as the relative number of participants who completed the pretest measurements but did not complete the post-test measurements for the active VR treatment phase.
Quality assessment
This systematic review included non-RCT studies. Therefore, the Mixed Methods Appraisal Tool was used to assess the quality of all included studies. 49 This critical appraisal tool can assess methodological quality across five study categories: RCT, nonrandomized studies, quantitative descriptive studies, qualitative studies, and mixed-methods studies.
Data analysis
A narrative synthesis approach was used to describe the findings of this systematic review. This is due to the small number of included papers and their heterogeneity on key data items (e.g., methodology, measures, comparators, and outcomes).
Results
Study selection
The literature search yielded 2,150 papers. A total of 1,457 records remained after duplicate removal. Of these records, seven met the eligibility criteria (Fig. 1).
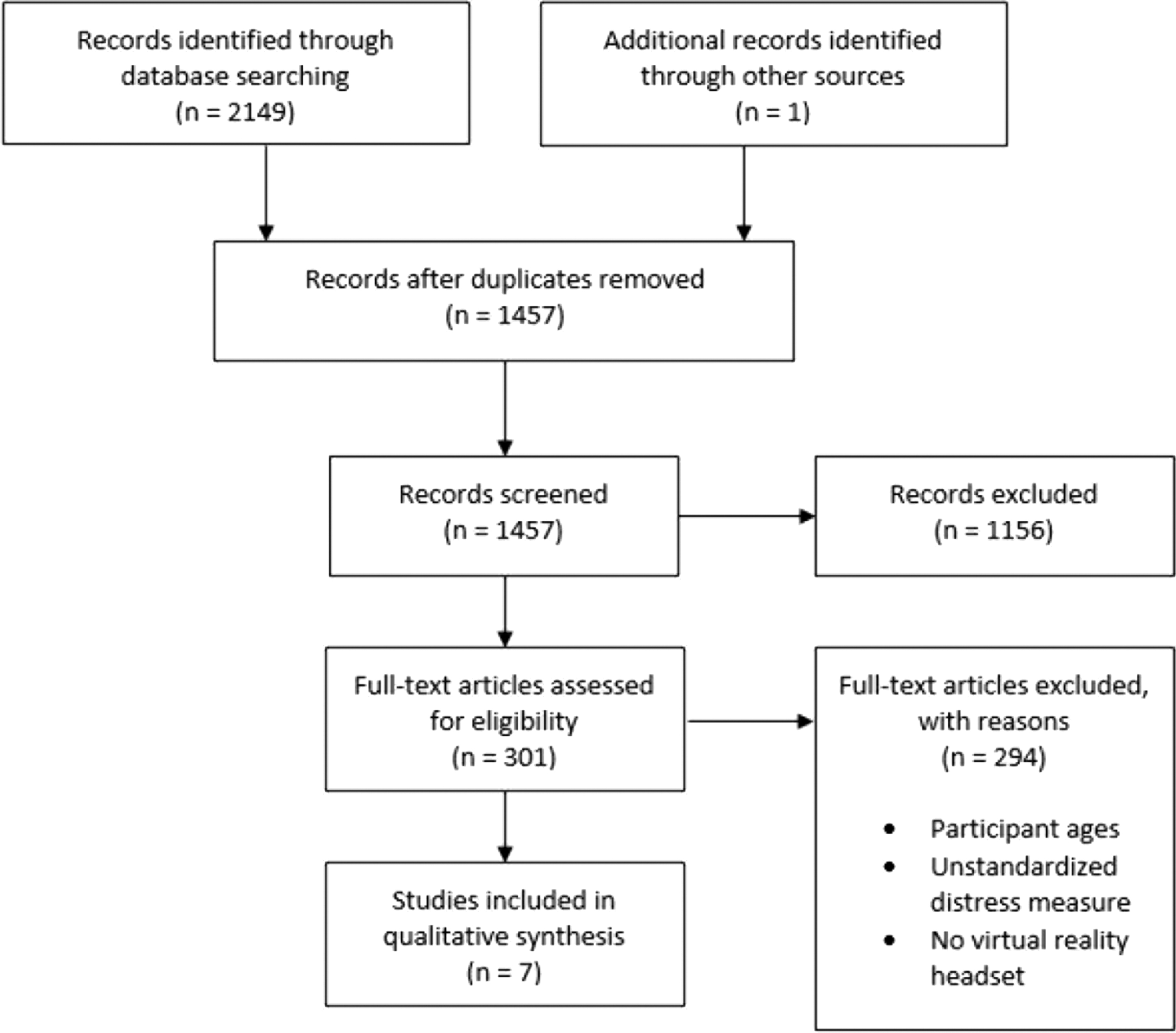
Flowchart of systematic review search results.
Participant characteristics
Four of the VR studies were from the United States and one each from Iran, Norway, and Netherlands (Table 1). Nearly all participants were aged between 10 and 19 years. However, the Gold and Mahrer 50 study had a small number of participants aged 20–21years (16/143, 11 percent of sample) that were defined as adolescents by the authors as they were attending a Children's Hospital. Across all studies, sample sizes ranged from 8 to 143 participants (median of 41). Participants were mainly female with an average sample proportion of 65.6 percent (range 12.5 to 100 percent). Each study focused on a unique distress-related issue. Four studies tested VR therapy on clinical samples, consisting of adolescents with various clinical diagnoses of mental disorders51,52 and medical conditions,50,53 whereas the remaining three studies tested VR with nonclinical samples.54–56 Clinical diagnoses included attention-deficit/hyperactivity disorder, autism spectrum disorder, reactive attachment disorder, oppositional defiant disorder, personality disorder, social anxiety disorder, eating disorder, and cancer (i.e., osteosarcoma, Ewing's sarcoma, brain tumors, ovarian cancer, and skeletal muscle cancer.
Description of Participants and Research Designs in Reviewed Studies
Refers to total number of participants in the study.
Refers to number of participants.
ABAB, baseline (A), intervention (B), withdrawal or no intervention (A), intervention (B); BC, between-cases; BG, between-groups; ER, emotion regulation; FU, followup; Post, post-test; Pre, pretest; RCT, randomized controlled trial; RP, role-play; SA, socially anxious; SC, standard care; VR, virtual reality; WG, within-groups; WLC, waitlist control.
Research designs
Table 1 shows that four studies used RCT designs. Control groups consisted of standard care (n = 2), waitlist (n = 1), and role-play intervention (n = 1). The chemotherapy study by Sharifpour et al. 53 has been classified as an RCT in this review. The authors confirmed in e-mail correspondence that participants were randomly assigned, with the control group receiving the same standard of care as the intervention group but without the VR component. The remaining three studies were uncontrolled pilot studies. Five studies reported between-group analyses, six studies reported within-group analyses, and one study reported between-cases analyses on their respective measures. Pretest and post-test assessments were used in five studies, with three of these studies also having followup assessments ranging from 1 week to 3 months.
Details of the VR interventions
All studies tested a unique VR intervention (Table 2). Six studies made use of interactive virtual environments that were custom-built for their intended treatment purpose. The remaining study used a passive VR film to distract participants during chemotherapy. 53 Treatment purposes included distraction, relaxation, exposure therapy, and psychological skill training. Across all studies, treatment ranged from 1 to 8 sessions, with a mode of 1. The time length of each session ranged from 5 minutes to 2.5 hours. A facilitator was present in all sessions to help guide the adolescent participants. All studies used a unique HMD configuration.
Details of the Virtual Reality Interventions and Their User Engagement Outcomes
—, not applicable; GPQ, Gatineau Presence Questionnaire; HMD, head-mounted display; NSQ, nonstandardized questions; PQ, Presence Questionnaire.
User engagement with the VR interventions
The average attrition rate was 3.6 percent across all studies in the active VR treatment phase, with a range of 0 to 10.6 percent (Table 2). One study reported the use of an intention-to-treat analysis. 56 Most studies used nonstandardized questions on VR user experience factors of presence, satisfaction, acceptability, attendance, simulator sickness, and engagement. However, two studies used standardized measures on VR user presence.52,55 These measures included the Gatineau Presence Questionnaire 57 and a modified version of the Presence Questionnaire. 58 Two studies did not report on user engagement factors.51,53
Psychological distress measures and outcomes
Details of the psychological distress measures and their VR treatment outcomes in the reviewed studies are summarized in Table 3. Measures included the Visual Analogue Scale, 59 Facial Affective Scale, 59 Spielberger State-Trait Anxiety Inventory, 60 Affect Dysregulation Scale, 61 Emotional Self-Efficacy, 62 Public Speaking Anxiety Scale, 63 Subjective Units of Distress Scale, 64 Trauma Symptom Checklist, 65 Pain Anxiety Symptoms Scale, 66 Pain Catastrophizing Scale, 67 and the “Lack of Emotional Awareness” and “Difficulty Accessing Emotion Strategies” subscales from the Difficulties in Emotional Regulation Scale. 68 The VR treatment effect sizes across all studies that reported them ranged from small to large in magnitude.
Details on Study Psychological Distress Measures and Reported Outcomes
ADS, Affect Dysregulation Scale; BC-SMD, between-case standardized mean difference; d, Cohen's d effect size; DAES, Difficulty Accessing Emotion Strategies; DEA, Difficulty in Emotional Awareness; ESE, Emotional Self-Efficacy; FAS, Facial Affective Scale; PCS, Pain Catastrophizing Scale; PASS, Pain Anxiety Symptoms Scale; PSAS, Public Speaking Anxiety Scale; STAI, State-Trait Anxiety Inventory; SUDS, Subjective Units of Distress; TSC, Trauma Symptom Checklist; VAS-A, Visual Analogue Scale-Anxiety; ηp 2 , partial eta-squared.
Quality assessment results
The included studies were quality assessed with the Mixed-Methods Appraisal Tool criteria. In all four RCT studies,50,54,56,53 randomization was appropriately performed, and participants reportedly adhered to their assigned VR intervention. Except for Sharifpour et al., 53 all RCT studies reported comparable baseline group analyses, and complete outcome data were defined as ≥80 percent. Only the RCT study by Gold and Mahrer 50 had blinding of outcome assessors, which was applied at pretest measurements. In the three quantitative descriptive studies,51,55,52 the sampling strategy was relevant to the research question, measures fulfilled inclusion criteria, nonresponse bias was low, and statistical analyses were appropriate. However, nonprobability sampling was used in these studies. It is also uncertain whether the adolescents sampled in the Parrish et al. 52 study for condition assignment were representative of those with social anxiety disorder due to the use of self-report measure scores rather than clinical diagnoses from a mental health professional.
Discussion
This review identified a low number of studies specifically directed at adolescents, with most previous studies using mixed age samples23,39,40 and at the time of writing is the first review so to do. Psychological distress is a prevalent and debilitating issue among adolescents,1–4 and it is important to identify and manage. Due to profound neurocognitive and psychosocial developmental differences between adolescents and these other life stages, 41 as well as rapid advancements in VR technology,21,44,45 this systematic review sought to provide a contemporary account on the impact of VR for managing psychological distress in adolescent samples. The included studies show that in various settings and contexts, VR interventions can quickly reduce negative symptoms as well as improve self-efficacy and access to emotion regulation strategies for specific adolescent populations.
Each study in this review pioneered a new VR intervention that made use of a unique HMD setup and software program. The VR hardware devices used in all included studies are affordable and commercially available for public use. Further, both active (e.g., playing an interactive game) 50 and passive (e.g., watching a film) 53 VR experiences were therapeutic for distressed adolescents. This implies that it may not be necessary to acquire expensive hardware, or build elaborate interactive virtual worlds, to achieve positive therapy outcomes with adolescents using VR.
The VR interventions were shown to be efficacious for distressed adolescents when delivered in a hospital, 50 research laboratory, 52 chemotherapy clinic, 53 and school,51,54,56 indicating the adaptability of VR technology to multiple settings. The large effect sizes found from the adolescent VRET feasibility studies52,55 mirror the outcomes of adult VRET studies on social anxiety disorder and performance anxiety. 26 These findings suggest that the adolescents found the VR environments to be analogous to real-world settings and emotionally evocative. Given the prevalence of mental health concerns during adolescence, the fact that VR can effectively impart psychoeducation and mental health skill training to help adolescents manage distressing situations is of particular interest. Adolescents were able to learn and practice adaptive behaviors on emotion regulation 54 and assertive resistance. 56
The data on distraction during medical procedures is reassuring and results are similar in children and adults, 23 indicating that any outlay on equipment is likely to be cost-effective for health services. The VR treatment also appears to provide rapid relief from psychological distress. In four of the studies, a single session varying from 5–150 minutes was sufficient to induce positive results for distress related to exposure therapy, 55 distraction, 50 and assertive resistance to victimization. 56
When consumer response was undertaken, adolescents rated their VR experiences favorably and reported little-to-no simulator sickness. Four reviewed studies screened out adolescents who reported a history of health issues, such as seizures and audio–visual impairments, from participation.50,52,54,55 The attrition rate appeared lower than adult studies.29,36 This suggests that adolescents may, indeed, find VR more engaging than adults and lends support to the almost universal assumption that adolescents will naturally respond positively to digital technologies.
Our conclusions are limited by the low study and participant numbers, the heterogeneity of methods between the RCTs and uncontrolled pilot studies, most participants being from a single country setting, and variable outcome indicators. Currently, there is no single suite of empirically validated VR tools to measure the effectiveness of this treatment for adolescent psychological distress. There is also comparatively more adult VR therapy research on other distress-related conditions that also affect adolescents, such as panic disorder, fear of flying, spider phobia, eating disorders, and post-traumatic stress disorder.26,29,37 Further, the adult data show that VR therapy effects can be sustained up to 12 months with little to no symptom deterioration. 37 Despite rapid advancements in VR technology posing a challenge for longitudinal intervention studies, followup periods greater than 3 months are still required to ascertain the duration of effects and whether VR could be considered a medium- to long-term management modality for adolescents, rather than just an acute intervention. Evaluating user experience factors with standardized measures (e.g., System Usability Scale) would help verify which VR devices, software environments, and therapeutic activities are preferred by adolescents, caregivers, and clinicians.
The paucity of studies precluded the capacity to perform a meta-analysis on VR treatment effects. Our methodology excluded conference handouts or gray literature. It is also possible that some VR intervention studies may have been missed due to nomenclature. For instance, a computer game may be playable in VR but may not have been described as a VR intervention. 44 In addition, the review focus was on HMDs, and it did not include other immersive technologies such as cave automatic virtual environments. 48
Conclusion
In summary, all studies reported benefits when using VR to manage psychological distress in adolescents and these benefits occurred across a range of treatment scenarios. One therapeutic modality serving multiple purposes is very attractive for clinical use. Adolescent participants rated their VR experience favorably, and low attrition rates were reported across all studies. However, conclusions on the effectiveness of VR in managing adolescent distress are limited by the lack of high-quality controlled studies, and the heterogeneity found in existing ones. It is unclear how effective VR interventions will be for moderate to long-term use, how they compare with other available treatment methods, and their appropriateness for adolescents across all distress-related issues and backgrounds. Therefore, more experimental studies of high methodological rigor (e.g., RCT) are required. Nevertheless, these preliminary findings suggest that VR is a valuable treatment modality for adolescent psychological distress. Moving forward, there are many opportunities for future VR studies to build on this empirical foundation.
Footnotes
Acknowledgments
This project was resourced by the Wellbeing Health & Youth Centre of Research Excellence in Adolescent Health, funded by the National Health and Medical Research Council (NHRMC).
Authors' Contributions
All authors have reviewed and approved of this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.