
Abstract
Visual field defect caused by glaucoma seriously affects the quality of life of patients, and clinically, this type of visual field defect has been considered to be irreversible. The aim of this study is to use binocular virtual reality training (VR training) to repair visual field defect in glaucoma patients, improve the quality of life of patients, and provide a new therapeutic strategy for the rehabilitation of glaucoma. Seventy glaucoma patients (median 56, range 15–84 years) were recruited and divided into control and training groups. Fifty-four patients' data were analyzed. The training group (n = 30) received binocular VR training for 3 months. The control group (n = 24) maintained the conventional treatment without any other intervention. Their visual field index (VFI) and mean defect (MD), and retinal nerve fiber layer average thickness (RNFL) and ganglion cell layer average thickness (GCL) average thickness before training and during followup were analyzed. In the training group, the VFI value (Z = 3.277; p = 0.001) and MD value (Z = 3.913; p < 0.0001) were significantly improved after 1 month of training. After 3 months of training, the VFI value (Z = 3.761; p < 0.0001) and MD value (Z = 3.133; p = 0.002) were significantly improved. There was no significant difference with the changes of average thickness of RNFL (p = 0.350) and GCL average (p = 0.383) after 3 months of training; whereas in the control group, except for a further reduction in GCL average thickness (Z = 3.158; p = 0.002) compared with the baseline data, the other followup data were not statistically significant compared with the baseline data. Our data suggested that binocular VR training can significantly improve the visual field defect of glaucoma patients but warrants further study with large sample size.
Clinical Trail registration number: ChiCTR1900027909.
Introduction
Glaucoma is a common eye disease characterized by damage to retinal ganglion cells and optic nerve, and its clinical features are mainly visual field defects and optic nerve damage. 1 Glaucoma is the second leading cause of blinding eye disease worldwide and the main cause of blinding eye disease in China. 2 The disease causes great damage to the physical and mental health of patients and seriously affects the quality of life of patients. 3 At present, the main clinical treatments for glaucoma include medications, lasers, and surgery to control intraocular pressure and delay the progression of optic nerve damage. 1 Traditionally, it has been considered that the optic nerve damage and visual field defect caused by glaucoma are irreversible, and there is still a lack of effective treatments to restore the visual field defect.
However, the central nervous system has significant neuroplasticity that shows a series of plastic changes after damage. 4 Recent studies have shown that visual loss is only partial, and there are some areas of residual vision (ARVs) available. In those ARVs, their visual fields do not function normally but their visual ability can be restored. Indeed, the term residual vision indicated the residual capacities that provide a structural substrate for restoration. 5 Even if only very few neurons (10 percent or less) survive, 6 their residual visual function can be restored by brain stimulation or visual training. 7
Our study is to investigate whether binocular virtual reality (VR) training can repair visual defects in patients with glaucoma. Seventy glaucoma patients were recruited and divided into control and training groups. The training group received binocular VR training for 3 months and the control group maintained the conventional treatment without any other intervention. Their visual field and retinal anatomical structure before and after visual training under the condition of stable intraocular pressure were analyzed.
Materials and Methods
Study subjects
After obtaining ethical approval from the ethics committee of Beijing Shijitan Hospital, Capital Medical University, and written informed consent, 70 glaucoma patients diagnosed in the glaucoma clinic of the Department of Ophthalmology, Beijing Shijitan Hospital, Capital Medical University, were recruited from March 2019 to January
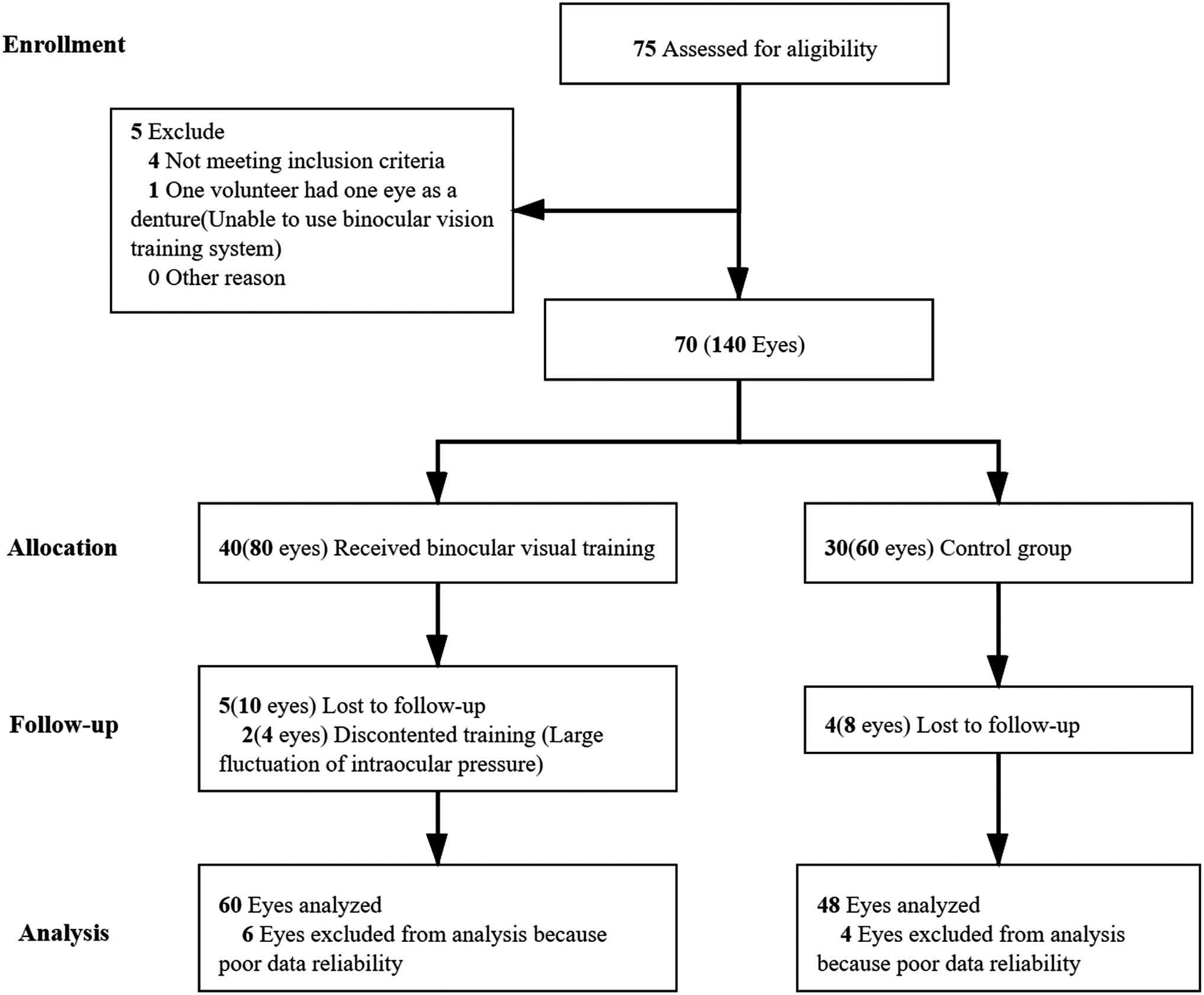
Consolidated standards of reporting trials diagram.
Baseline Data
GCL, ganglion cell layer average thickness; MD, mean defect; RNFL, retinal nerve fiber layer average thickness; VFI, visual field index.
Inclusion criteria were (a) the clinical diagnostic criteria of glaucoma patients; (b) glaucoma visual field defect; (c) visual field stability for >3 months; (d) intraocular pressure ≤21 mmHg; (e) refraction: sphere −3.00DS to +3.00DS, cylinder −3.00DC to +3.00DC, anisometropia ≤2D; and (f) willing to participate in the study.
Exclusion criteria were (a) high myopia (refraction: sphere more than −6.00DS), uveitis, maculopathy, diabetic retinopathy, and other retinal optic nerve diseases; (b) history of surgery affecting the retinal optic nerve within half a year; and (c) other central nervous system degenerative diseases that may cause optic nerve degeneration.
Withdrawal criteria were if any of the following occurs in patients, they were withdrawn from this study: (a) patients who need to adjust glaucoma medication or surgery due to changes in the condition (such as large fluctuations in intraocular pressure and acute attack of glaucoma) and poor compliance; (b) patients who cannot tolerate VR training; (c) patients who cannot be trained as instructed; and (d) patients who cannot be followed up regularly.
Methods
Visual field assessment: Automated perimetry was performed with the Humphrey Field Analyzer (model 3-860) using the standard full threshold 24-2 program of Zeiss Humphrey 3-860 perimeter. All tests were performed by the same skilled examiner. Perimetry was performed at least twice before recruitment. The second or third more reliable perimetry result was selected as the baseline visual field of the patient. Reliability criteria included fixation loss <20 percent and false negative and false positive rates <15 percent. The visual field index (VFI) and mean defect (MD) values were recorded for each patient. Patients' eyes with unreliable visual fields were excluded for further analyses.
Optical coherence tomography (OCT) examination: The average thickness of the inner segment cell layer (ganglion cell layer [GCL]) within the range of 5 * 5 mm in macular area and the average thickness of retinal nerve fiber layer (RNFL) were measured using CirrusTMHD-OCT5000 (Version 4.0; Zeiss).
Binocular VR training: As reported in our pilot study, 8 binocular VR training was performed by using the binocular visual function push-pull training system provided by the National Center for Medical Device Engineering and Technology (Guangzhou, China). The binocular visual function push-pull training system includes the following parts.
(a) Binocular VR training and eye movement following: As shown in Figure 2, through the red and blue spectacles for visual separation, the red lens is put on the “bad” eye (more visual field loss) and the eye movement pursuit function is used to find out the icon corresponding to all the targets in the upper right corner (the red heart) and clicks with the quasi-star alignment. The binocular split icon will be randomly distributed on the interface. Moving collimator will magnify the icon of aiming range and the mouse is clicked to magnify again. Visual split stimuli (scaling) within different binocular fields were completed by pursuit search, the differential visual targets remained high-energy flashing, the stimuli were further scaled after paired clicks, and saccade pairing judgments were continuously performed.
(b) Binocular stereopsis training and eye movement fixation training: As shown in Figure 3, by wearing red and blue glasses for binocular split vision, the binocular parallax of foveal contour stereopsis will undergo cross and noncross changes. Peripheral vision sees a wide range of rough stereo vision, and also undergoes crossover and noncrossover changes of binocular parallax. Through this mode, the patient's dynamic stereo vision can be trained and the peripheral vision can be activated.
(c) Binocular VR training and eye movement saccade training: As shown in Figure 4, through the red and blue spectacles for visual separation, the red lens is put on the “bad” eye. The Gabor spot undergoes dynamic phase stimulation changes. The patient needs to determine the global orientation of the Gabor spot, and at the same time adjust other Gabor spots that are different from the global orientation to the same orientation as the global orientation through the eye movement saccade function.
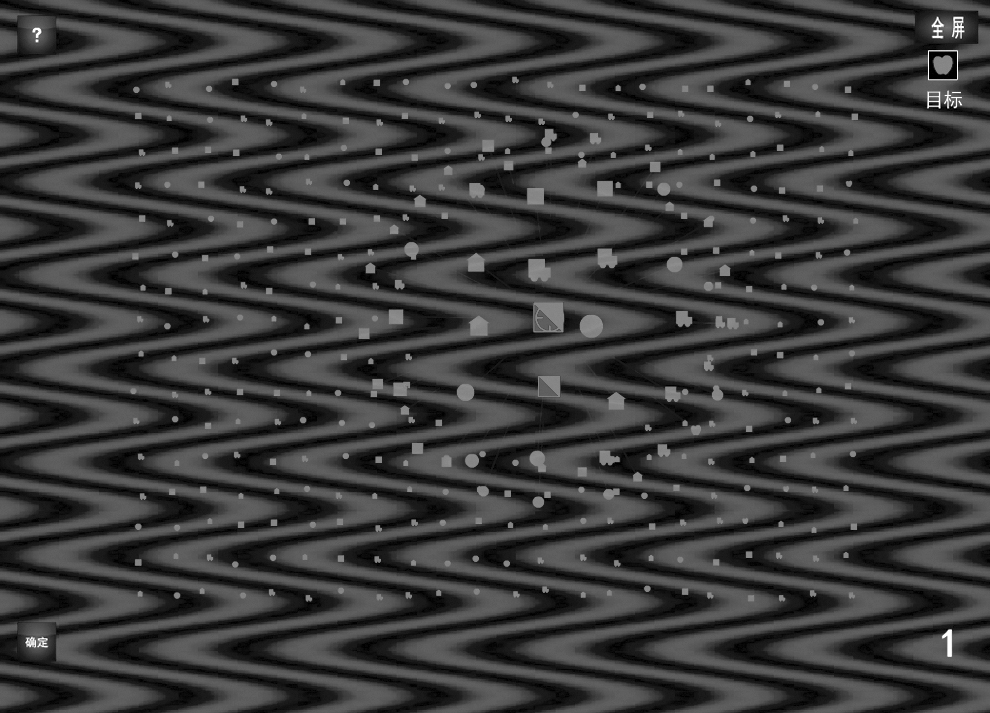
Binocular VR training and eye movement: Through the red and blue spectacles for visual separation, the red lens is put on the “lazy” eye (more visual field loss), the eye movement pursuit function is used to find out the icon corresponding to all the targets in the upper right corner (the red heart) and clicks with the quasi-star alignment. The binocular split icon will be randomly distributed on the interface. Moving collimator will magnify the icon of aiming range and the mouse is clicked to magnify again. Visual split stimuli (scaling) within different binocular fields were completed by pursuit search, the differential visual targets remained high-energy flashing, the stimuli were further scaled after paired clicks, and saccade pairing judgments were continuously performed. VR, virtual reality.
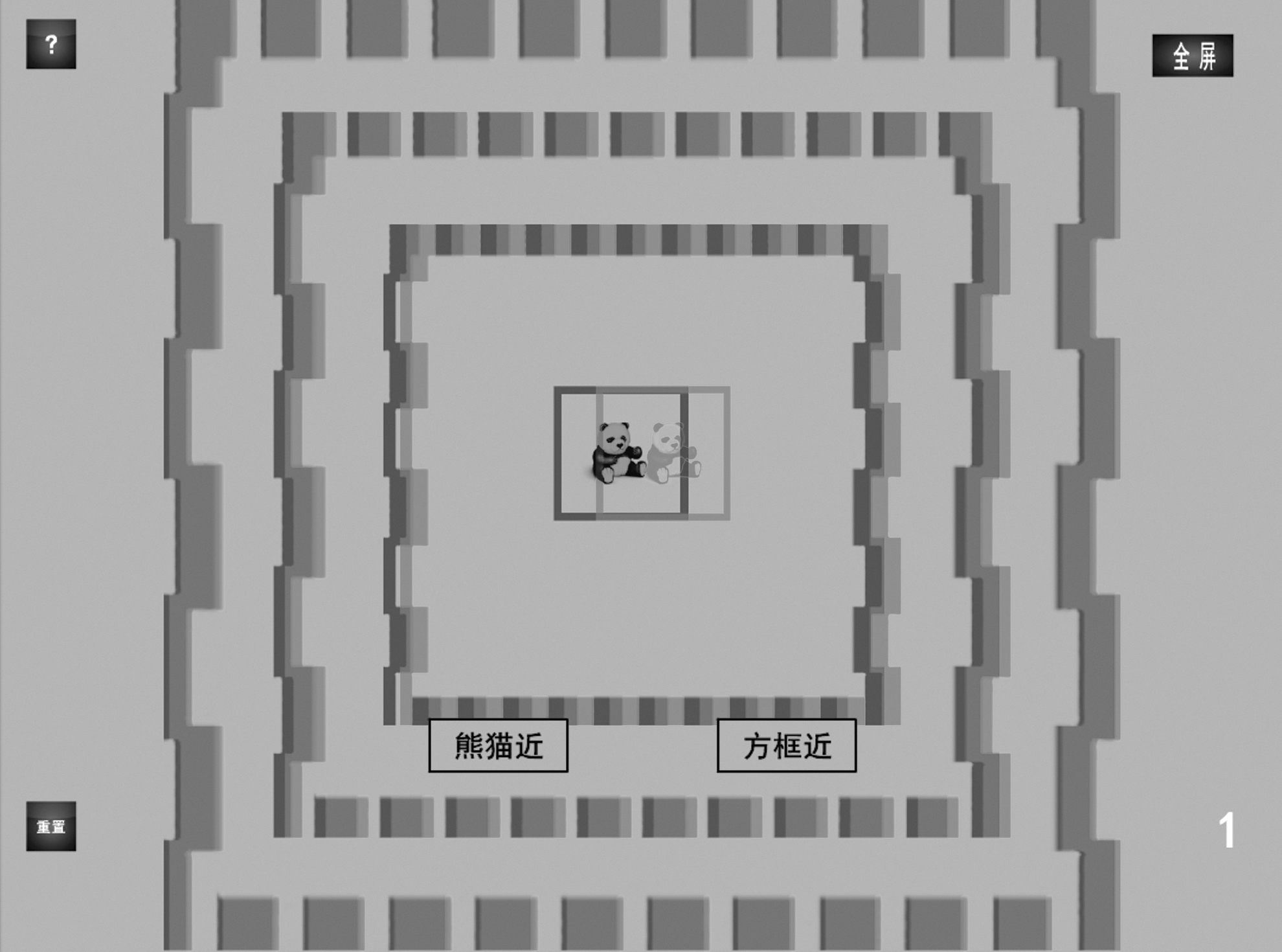
Binocular stereopsis training and eye movement fixation training: By wearing red and blue glasses for binocular split vision, the binocular parallax of foveal contour stereopsis will undergo cross and noncross changes. Peripheral vision sees a wide range of rough stereo vision, and also undergoes crossover and noncrossover changes of binocular parallax. Through this mode, the patient's dynamic stereo vision can be trained and the peripheral vision can be activated.
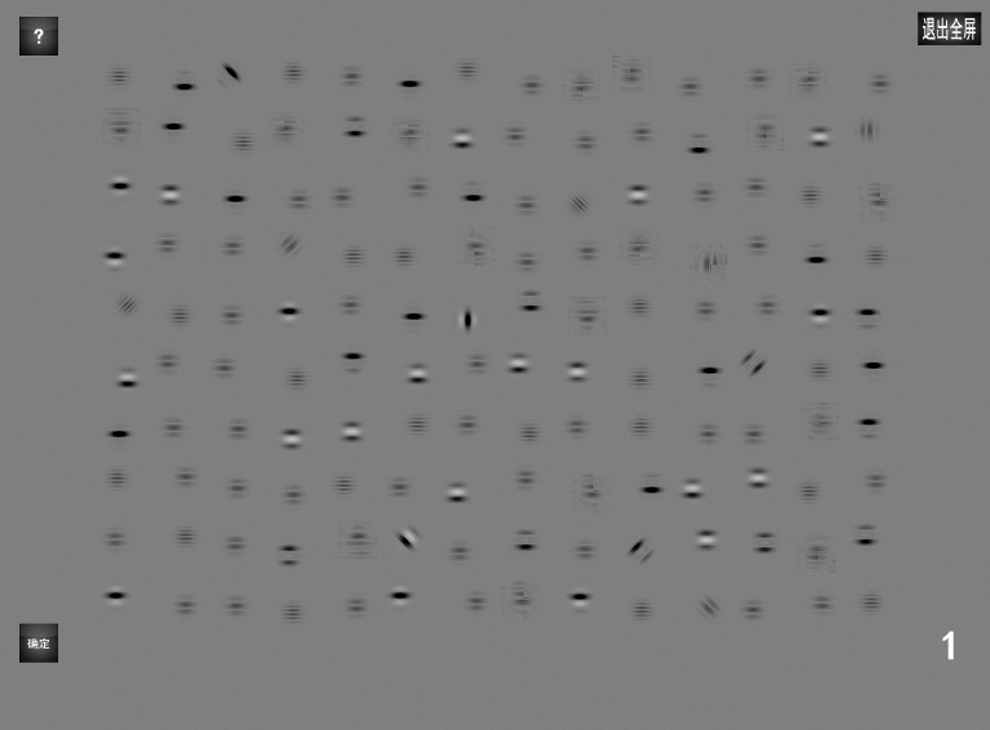
Binocular VR training and eye movement saccade training: Through the red and blue spectacles for visual separation, the red lens is put on the “bad” eye. The Gabor spot undergoes dynamic phase stimulation changes. Patient needs to determine the global orientation of the Gabor spot, and at the same time adjust other Gabor spots that are different from the global orientation to the same orientation as the global orientation through the eye movement saccade function.
In the training group, patients perform binocular VR training at home for 3 months, twice a day, 20 minutes for each training session. All training data (including daily training duration and daily training times) can be monitored in the computer background to ensure the integrity of training. The followup data of patients who cannot adhere to the training will be eliminated.
Statistical analysis method
Data are presented as mean ± standard deviation and analyzed with paired t-test or Wilcoxon test (SPSS 23.0 statistical software) wherever appropriate. p < 0.05 was considered to be a statistical significance.
Result
A total of 70 volunteers (140 eyes) participated in this study and were divided into training groups (n = 40; 80 eyes) and control (n = 30; 60 eyes) group. In the training group, five (10 eyes) patients were lost to followup, two (4 eyes) patients could not continue training due to changes in their condition (large fluctuations in intraocular pressure), and 6 eyes' data (false negative rate >15 percent in 3 eyes and false positive rate >15 percent in 3 eyes) were excluded due to poor reliability. In the control group, four (eight eyes) patients were lost to followup and four eyes' data (false negative rate >15 percent in 4 eyes) were excluded due to poor reliability. Finally, 108 eyes' data were analyzed and reported.
Changes in visual field examination: The VFI and MD value changes of volunteers in the first and third months are given in Table 2 and Figures 5 and 6. In the training group, compared with the baseline data before training, the VFI (Z = 3.277; p = 0.001) and MD values (Z = 3.913; p < 0.0001) were improved after 1 month training. The VFI (Z = 3.761; p < 0.0001) and MD values (Z = 3.133; p = 0.002) were improved after 3 months of training, the difference was statistically significant. There was no statistically significant change in VFI (p = 0.662) and MD (p = 0.936) values between 1 month training and 3 months training data. In the control group, the changes in VFI values and MD values at 1 and 3 months of followup were not statistically significant compared with baseline data.
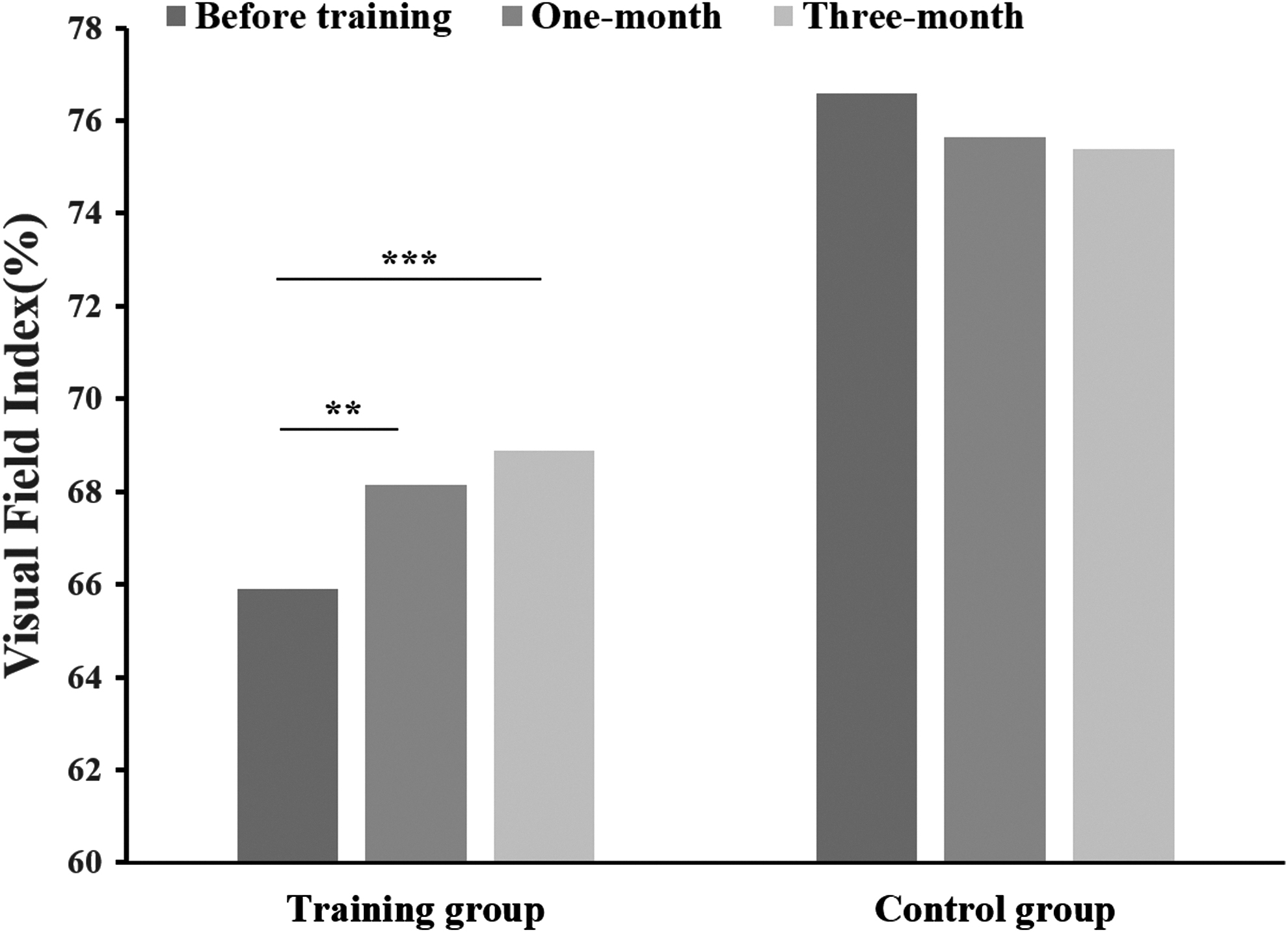
Comparison of patients' VFI during followup. In the training group, the VFI after 1 and 3 months of training were statistically significant when compared with the baselines (p < 0.05). In the control group, 1-month and 3-month data were not statistically significant compared with baseline data. (**p < 0.005, ***p < 0.0005) VFI, visual field index.

Comparison of patients' MD during followup. In the training group, the MD after 1 and 3 months of training were statistically significant when compared with the baselines (p < 0.05). In the control group, 1-month and 3-month data were not statistically significant compared with baseline data. MD, mean defect. **p < 0.005.
Comparison of Visual Field Parameters Before and After Training
Asterisks indicate statistical significance in paired t-test or Wilcoxon test; *p < 0.05, **p < 0.005, ***p < 0.0005; in the training group, compared with the baseline data before training, the VFI (p = 0.001) and MD values (p < 0.0001) were improved 1 month after training. The VFI (p < 0.0001) and MD values (p = 0.002) were improved after 3 months of training, the difference was statistically significant. In the control group, the changes in VFI and MD values at 1 and 3 months of followup were not statistically significant compared with baseline data.
Changes in RNFL and GCL average thickness: As given in Table 3, in training group, there was no significant difference in mean thickness of RNFL (p = 0.350) and GCL (p = 0.383) after 3 months training. In the control group, the change in RNFL average thickness (p = 0.108) was not statistically significant, however, the GCL average thickness (Z = 3.158; p = 0.002) was further reduced, which was statistically significant.
Comparison of Optic Nerve Parameters Before and After Training
In the training group, there was no significant difference in mean thickness of RNFL and GCL after 3 months training. In the control group, the change in RNFL average thickness was not statistically significant. The GCL average thickness (p = 0.002) was further reduced, which was statistically significant. **p < 0.005.
Discussion
Traditionally, visual field damage was considered to be irreversible because the retina and optic nerve cannot regenerate. However, the recent discovery of neuroplasticity and residual visual activation indicated that the brain processes visual signals by improving the efficiency of processing, enhancing the prominent efficacy, amplifying the residual signal, and finally activating and synchronizing the brain functional network, improving visual function, and repairing the damaged visual field.9,10
The following strategies are currently available to stimulate residual visual areas (a) visual experience, (b) active behavioral training, and (c) electrical brain stimulation. Training (practice) of visual functions is currently the most widely used method to alter visual system plasticity and induce vision restoration. This includes the vision restoration training (VRT developed by Kasten and Sabel), 11 which suggests that repeated testing at the boundaries of the field of view may cause boundary shifts. Other laboratories have used different kinds of training paradigms including different orientations to train patients.12,13 Only very few studies suggested that training has no significant effect, 14 but no study found that visual training had a negative effect on patients.
Our study showed that after binocular VR training, the visual field defect of patients was improved after 1 month of training compared with the baseline data, and the visual field defect was significantly improved after 3 months of training. MD is a sensitive indicator of diffuse visual field damage in response to glaucoma. In line with our pilot study 8 and the previous study from others,11,13,15–18 visual training activated residual visual function, improved visual field defects, and enlarged the visual field in patients. We have an interesting example of this. As is shown in his perimetry report (Fig 7), the black area represents the absolute field defect, the white area represents the normal, and the gray area represents the partial survival of neurons or neuronal function, that is, the residual visual acuity area. 5 After 3 months of VR training, the visual field defects in the superior nasal and superior temporal regions of this patient were significantly improved. Interestingly, the absolute defect area (the black part) of visual field was also improved in this patient after 3 months of training. Our results suggest that VR enlarges the visual field by stimulating the visual residual area and “amplifying” the function of the residual neural tissue, and finally repair the glaucomatous visual field damage.
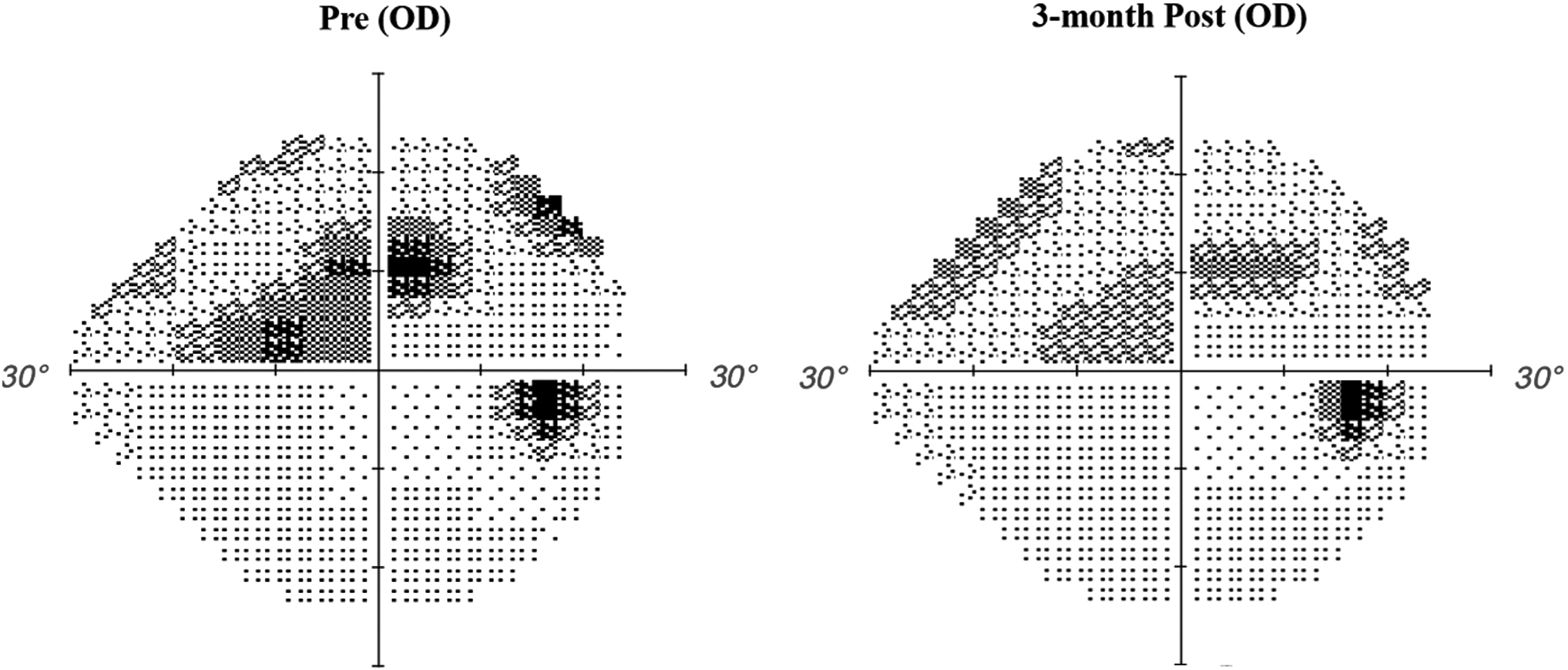
Visual fields change of one patient during followup. Patients were assessed for visual field loss using the Humphrey perimeter. Different gray levels represent different degrees of damage to the visual field. Black, blind areas; gray, areas of relative defects, (zones with residual vision); white, intact areas. No. 22, male, 48 years old, POAG (primary open angle glaucoma), the VFI was 84 percent and MD value was −6.73 dB before training. After 3 months of binocular visual training, the VFI is 87 percent and MD value is −6.26 dB. As is shown in the figure, the patient's visual field defect above the nose and the temporal side were improved than before training.
In addition, our study found that there were no statistically significant changes in retinal anatomy-related parameters (average thickness of RNFL and GCL) compared with the baseline data, which may be due to the following reasons: (a) the small sample size and the short training time (only 3 months) and (b) the optic nerve injury was irreversible and necrotic optic nerve occurred.
The possible mechanisms of binocular VR training are as follows: (a) neuroplasticity of the retina 7 ; (b) residual visual activation5,6; (c) reorganization of the brain functional network, increased synaptic efficacy, and “amplification” of visual signals. 9 Indeed, a previous study suggested 19 that after training, functional magnetic resonance imaging of the patient's brain showing the visual cortex was activated and the connection of the attention network was strengthened, indicating that reorganization and brain plasticity may be one of the mechanisms of visual training. However, the specific mechanism of the VR training in activating residual vision remains unclear and further studies are needed.
Compared with the traditional electric stimulation of optic nerve 20 and computer-based VRT training (which is monocular visual training), the binocular VR training system was used in this study. Patients use the binocular VR push-pull training system to perform the training at home, and it is an uninvasive therapy. At present, activating neuroplasticity by visual training has been widely used in amblyopia and strabismus treatment,16,21,22 but there are no relevant reports on the application of binocular VR training in the field of glaucoma and our study is the first of a few of this type. However, our study has the following limitations: (a) the visual field data change was not statistically significant at 3 months of training compared with 1 month of training. The optimistic training duration was unknown, which needed further study. (b) The sample size was relatively small.
Conclusion
In summary, our study indicated that binocular VR training can repair visual field damage in glaucoma patients, which is helpful to improve the life ability and provide a new therapeutic strategy for the rehabilitation of glaucoma patients.
Footnotes
Authors' Contributions
Conception of the study was carried out by Y.L. and J.H.F.; experiments were carried out by J.H.F., H.C., and L.Y.; data were analyzed by J.H.F. and H.C.; article preparation was done by J.H.F.; and review and editing were carried out by Y.L., M.W., and B.W.
Author Disclosure Statement
The named authors have no conflict of interest, financial or otherwise. All authors declare that (a) no support, financial or otherwise, has been received from any organization that may have an interest in the submitted study and (b) there are no other relationships or activities that could appear to have influenced the submitted study. Informed consent was obtained from all patients included in this study.
Funding Information
This study was funded by Beijing Municipal Administration of Hospitals Clinical Technology Innovation Project (XMLX201808) and Beijing Municipal Administration of Hospitals Incubating Program (PX2020029).