
Abstract
Online hate speech has become a widespread problem in the daily life of adolescents. Despite growing societal and academic interest in this online risk, not much is known about the relationship between online hate speech victimization (OHSV) and adolescents' mental well-being. In addition, potential factors influencing the magnitude of this relationship remain unclear. To address these gaps in the literature, this study investigated the relationship between OHSV and depressive symptoms and the buffering effects of resilience in this relationship. The sample consists of 1,632 adolescents (49.1% girls) between 12 and 18 years old (Mage = 13.83, SDage = 1.23), recruited from nine schools across Spain. Self-report questionnaires were administered to assess OHSV, depressive symptoms, and resilience. Regression analyses revealed that OHSV was positively linked to depressive symptoms. In addition, victims of online hate speech were less likely to report depressive symptoms when they reported average or high levels of resilience (i.e., social competence, personal competence, structured style, social resources, and family cohesion) compared with those with low levels of resilience. Our findings highlight the need for the development of intervention programs and the relevance of focusing on internal and external developmental assets to mitigate negative outcomes for victims of online hate speech.
Introduction
The upsurge of online hate speech, a communicative form of expression that deliberately promotes, justifies, or disseminates exclusion, contempt, and devaluation of particular social groups (e.g., LGBTQIA+, people of color, people with Muslim and Jewish backgrounds, refugees)1–3 and its impact on people's well-being has become a growing concern.4–7 However, to date, little is known about the psychological outcomes of online hate speech victimization (OHSV) in adolescence. In the same line, little research has investigated the factors that might mitigate negative outcomes of OHSV. Resiliency theory provides a powerful framework for understanding why some young people develop positively despite traumatizing experiences. 8 And yet, this approach has not been empirically tested for OHSV among adolescents.
To address these gaps in the literature, this study investigated the relationship between OHSV and depressive symptoms and determined the moderating effects of resilience in this relationship. The findings could inform the design of strength-based approaches in anti-hate speech interventions.
OHSV and depressive symptoms
Hate speech offline or online includes insults, threats, and slurs through comments, images, or videos and is intended to incite hatred or violence against a specific social group. It undermines the sense of assurance, the social standing and equality, and dignity of people who identify as members of the target group.9,10 Through insults and humiliation targeted against one's social identity, adolescents may develop a biased view of themselves and mistrust the intention of others. Indeed, exposure to online hate speech has been shown to be associated with lower levels of psychological well-being and higher levels of emotional stress.4,11–13
According to the diathesis-stress model for depression, 14 OHSV can be understood as a salient stressor in adolescents' lives, which increases the odds of developing depressive symptoms. Indeed, empirical research conducted among young adults demonstrated that people who experience OHSV showed an increased risk of depression.11,15,16 Although research on psychological effects of OHSV among adolescents is a new research topic, there is a large body of cross-sectional research,17,18 longitudinal studies,19,20 and meta-analyses21–23 showing unequivocally that psychological distress and harm caused by online bullying victimization can increase adolescents' risk for depressive symptoms. Therefore, we hypothesized that
H1: OHSV is positively associated with depressive symptoms among adolescents.
Buffering effects of resilience in the relationship between OHSV and depressive symptoms
Not everybody victimized through online hate speech is equally affected by it. Initial research showed that adolescents' ability to cope productively with online hate speech is positively related to their mental well-being 24 and that family support is positively associated with adolescents' ability to cope productively with online hate speech. 25 These findings indicate that resilience might play a major role in understanding the relationship between OHSV and negative health outcomes among adolescents. Resilience refers to having positive adaptation even when faced with significant adversity or trauma. 26
Resilience can be understood as a multifaceted construct that is often operationalized by considering three overarching categories, namely individual factors (e.g., social competence [SoC], personal competence [PeC], structured style [StT]), familial factors (e.g., family cohesion [FaC]), and a supportive environment outside the family (e.g., social resources [SoR]).8,26,27 Resilience factors such as SoC, PeC, StT, FaC, and SoR have been shown to be negatively correlated with internalizing mental health problems (e.g., depressive symptoms, symptoms of anxiety, suicidal ideation, self-harm). 7 Furthermore, previous research showed that resilience mitigated the effect of bullying victimization on subjective well-being, 28 the effect of online bullying victimization on depression, 29 as well as the effect of peer victimization on depressive symptoms. 30 Hence, we hypothesized that:
H2: The relationship between OHSV and depressive symptoms is weaker when resilience is higher than when resilience is lower.
Method
Participants
The study sample consisted of 1,632 Spanish adolescents between 12 and 18 years old (Mage = 13.83, SDage = 1.23). In terms of gender, 50.6 percent (n = 826) self-identified as girls, 49.1 percent (n = 801) as boys, 0.2 percent (n = 4) as gender diverse, and 0.06 percent (n = 1) did not indicate their gender.
Regarding sexual orientation, 89.8 percent (n = 1,465) self-identified as heterosexual, 1.7 percent (n = 28) as homosexual, 5.6 percent (n = 92) as bisexual, 2.1 percent (n = 34) as something else, and 2.1 percent (n = 34) did not indicate their sexual orientation. Concerning migration background, 85.1 percent (n = 1,439) were born in Spain and 11.8 percent (n = 193) in another country. The parents of most participants were married or living together (72.1 percent), whereas 23.3 percent were divorced or separated, 3.1 percent were single parents, 1.3 percent were widowed, and 0.2 percent did not answer this question.
Measures
Online hate speech victimization
To measure OHSV, participants were asked: “How often in the past 12 months have you personally been the target of hateful or degrading content online because of your sex, religious affiliation, race, or sexual orientation?” Participants rated the item on a response scale of “never,” “1 or 2 times,” “3 to 5 times,” “6 to 9 times,” and “more than 10 times.”
Resilience
We measured resilience by using the Resilience Scale for Adolescents, 8 which consisted of five subscales, namely SoC (four items, e.g., “I can easily make new friends,” Cronbach's α = 0.83), PeC (five items, e.g., “Self-confidence helps me overcome difficult moments,” Cronbach's α = 0.88), StT (three items, e.g., “I achieve my goals if I make a great effort,” Cronbach's α = 0.85), SoR (five items, e.g., “I always have somebody available when I need it,” Cronbach's α = 0.92), and FaC (six items, e.g., “I feel comfortable with my family,” Cronbach's α = 0.92). The response scale had 5-point Likert response options ranging from “strongly disagree” to “strongly agree” with higher scores indicating higher resilience.
Depressive symptoms
The Depression Subscale of the Brief Symptom Inventory 31 was used to measure symptoms of depression (e.g., “Feeling sad”) during the past 2 weeks. The response scale had 5-point Likert response options ranging from “not at all” to “extremely” with higher scores indicating higher levels of depressive symptoms. The Cronbach's α was 0.89.
Control variables
All analyses were controlled for participants age, dichotomized gender (girls vs. boys), dichotomized sexual orientation (heterosexual vs. homosexual, bisexual, and something else), and Internet use during the week and weekend. For both items measuring Internet use, the five response options ranked from “not at all” to “four hours or more.”
Procedure
This study was part of a larger research project on online risks among adolescents, which was approved by the Autonomous University of Madrid Ethics Committee (CEI-102-1943). Overall, seven public schools and two private schools in the community of Madrid participated in this study. As the adolescents were underage, parents had to sign a written consent form allowing them to participate. Approximately 65 percent of the parental permission slips were returned with a positive response.
Adolescents were informed that their participation was anonymous, their participation was optional, they could choose not to answer questions, and that participation could be stopped at any time without giving a reason and with no consequence. Data were collected by using paper-pencil questionnaires during one regular school hour. To prevent distress and further harm by participating in this study, participants were given written information about the researchers' contact details and helpful resources in the community.
Data analyses
First, descriptive statistics and bivariate correlations were computed to investigate the study variables. Then, we examined five regression-based moderated models with each resilience subscale, namely SoC, PeC, StT, SoR, and FaC, as moderators. All models controlled for participants' age, gender, sexual orientation, and Internet use during the week and weekend. The moderation models were computed with 5,000 bias-corrected bootstrap samples and 95% confidence intervals, using the PROCESS Macro version 3.5. 32 All variables that defined products were mean centered. Multicollinearity diagnostics were assessed and revealed correlations within an acceptable range (Table 1).
Means, Standard Deviations, and Correlations Between Online Hate Speech Victimization, Resilience, and Depressive Symptoms
p < 0.01; **p < 0.001; N = 1.588.
M, mean; SD, standard deviation.
Overall, between 0.4 percent (n = 4; Internet use during the week) and 2.5 percent (n = 40; StT) of data were missing. Little's missing completely at random (MCAR) test revealed that the data were missing completely at random (χ 2 = 63,23, df = 66; p = 0.574), indicating that a listwise deletion of missing data does not lead to biased parameters and standard errors (SEs). 33
Results
Means (M), standard deviations (SDs), and bivariate correlations between OHSV, the five resilience subscales, and depressive symptoms are given in Table 1. All correlations were in the expected direction.
Associations between OHSV, resilience, and depressive symptoms
Social competence
Model 1 explained 20 percent of the variance in depressive symptoms, F(8, 1545) = 48.96, p < 0.001, R2 = 0.202 (Table 2). OHSV (B = 0.49, p < 0.001) was positively associated with depressive symptoms and SoC was negatively related to depressive symptoms (B = −0.11, p < 0.001). A significant interaction was found between OHSV and SoC when predicting depressive symptoms (B = −0.18, p = 0.033). Probing the significant interaction effect further revealed that the unstandardized simple slope coefficients were bsimple = 0.66 (SE = 0.10, p < 0.001, at −1 SD) for low, bsimple = 0.49 (SE = 0.08, p < 0.001, at 0 SD) for moderate, and bsimple = 0.31 (SE = 0.12, p < 0.001, at +1 SD) for high SoC, indicating that the positive relationship between victimization and depressive symptoms was weakened as SoC increased (Fig. 1).

Graphical representation of the moderation of social competence on the association between OHSV and depressive symptoms. OHSV, online hate speech victimization.
Five Regression Models Predicting Depressive Symptoms
Reference categories: gender = boys; sexual orientation = not heterosexual.
95% bias-corrected bootstrap confidence intervals based on 5,000 samples.
CI, confidence interval; FaC, family cohesion; HSV, hate speech victimization; OHSV, online hate speech victimization; PeC, personal competence; SE, standard error; SoC, social competence; SoR, social resources; StT, structured style.
Personal competence
Model 2 resulted in 28 percent explained variance in depressive symptoms, F(8, 1545) = 67.47, p < 0.001, R2 = 0.278 (Table 2). OHSV (B = 0.37, p < 0.001) was positively associated with depressive symptoms and PeC was negatively related to depressive symptoms (B = −0.28, p < 0.001). A significant moderation effect was found between OHSV and PeC when predicting depressive symptoms (B = −0.24, p < 0.001). Probing the significant interaction effect further revealed that the unstandardized simple slope coefficients were bsimple = 0.61 (SE = 0.09, p < 0.001, at −1 SD) for low, bsimple = 0.38 (SE = 0.08, p < 0.001, at 0 SD) for moderate, and bsimple = 0.16 (SE = 0.13, p = 0.216, at +1 SD) for PeC, indicating that the positive relationship between victimization and depressive symptoms was weakened as PeC increased from low to average levels (Fig. 2).

Graphical representation of the moderation of personal competence on the association between OHSV and depressive symptoms.
Structured style
Model 3 resulted in 22 percent explained variance in depressive symptoms, F(8, 1543) = 54.17, p < 0.001, R2 = 0.219 (Table 2). OHSV (B = 0.50, p < 0.001) was positively associated with depressive symptoms and StT was negatively related to depressive symptoms (B = −0.17, p < 0.001). A significant moderation effect was found between OHSV and PeC when predicting depressive symptoms (B = −0.21, p = 0.014). Probing the significant interaction effect further revealed that the unstandardized simple slope coefficients were bsimple = 0.72 (SE = 0.11, p < 0.001, at −1 SD) for low, bsimple = 0.50 (SE = 0.08, p < 0.001, at 0 SD) for moderate, and bsimple = 0.29 (SE = 0.12, p = 0.014, at +1 SD) for StT, indicating that the positive relationship between victimization and depressive symptoms was weakened as StT increased (Fig. 3).
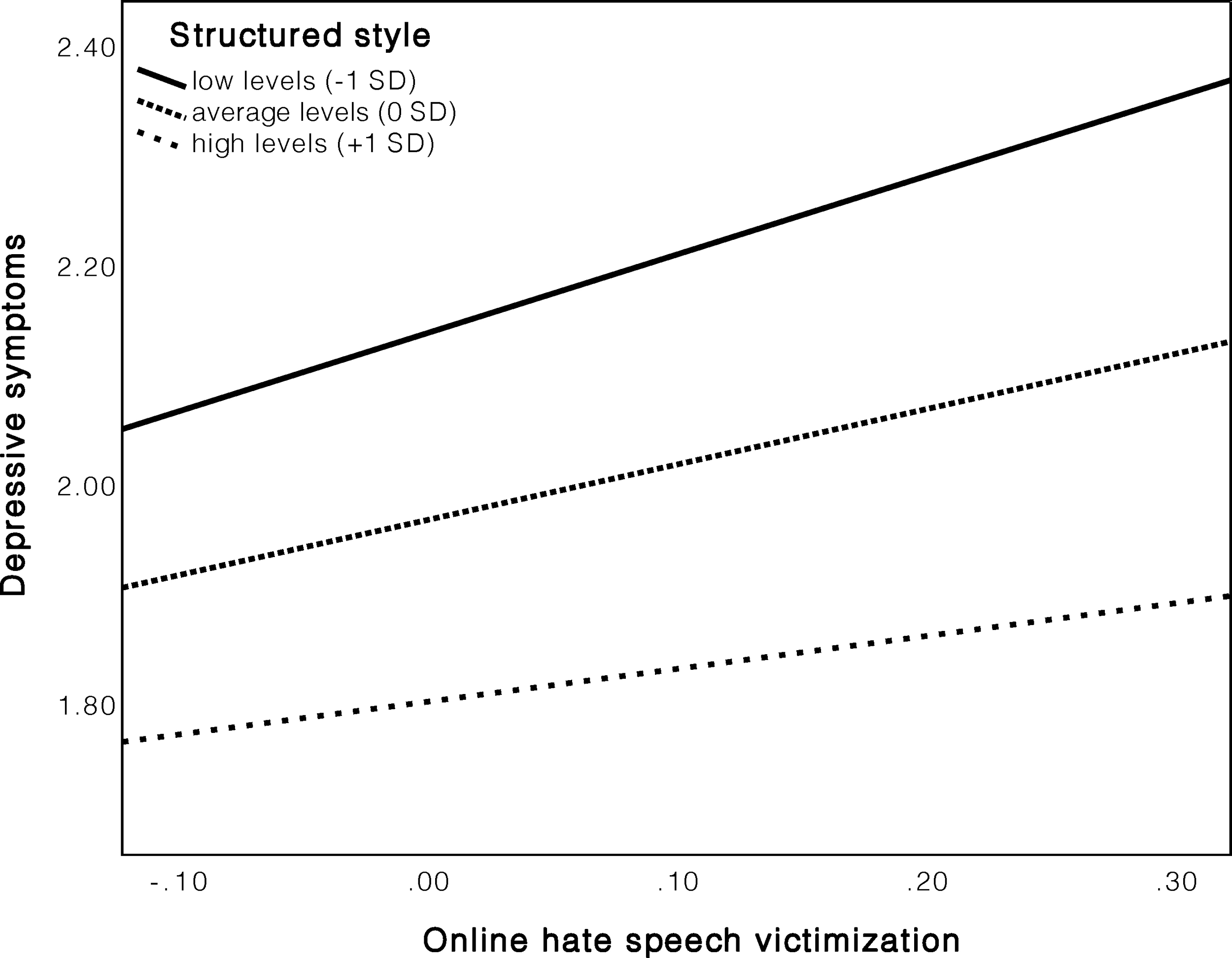
Graphical representation of the moderation of structured style on the association between OHSV and depressive symptoms.
Social resources
Model 4 resulted in 22 percent explained variance in depressive symptoms, F(8, 1544) = 51.54, p < 0.001, R2 = 0.211 (Table 2). OHSV (B = 0.42, p < 0.001) was positively associated with depressive symptoms and SoR was negatively related to depressive symptoms (B = −0.16, p < 0.001). A significant moderation effect was found between OHSV and SoR when predicting depressive symptoms (B = −0.20, p = 0.007). Probing the significant interaction effect further revealed that the unstandardized simple slope coefficients were bsimple = 0.63 (SE = 0.09, p < 0.001, at −1 SD) for low, bsimple = 0.40 (SE = 0.09, p < 0.001, at 0 SD) for moderate, and bsimple = 0.24 (SE = 0.12, p = 0.036, at +1 SD) for SoR, indicating that the positive relationship between victimization and depressive symptoms was weakened as SoR increased (Fig. 4).

Graphical representation of the moderation of social resources on the association between OHSV and depressive symptoms.
Family cohesion
Model 5 resulted in 25 percent explained variance in depressive symptoms, F(8, 1544) = 57.79, p < 0.001, R2 = 0.248 (Table 2). OHSV (B = 0.41, p < 0.001) was positively associated with depressive symptoms and FaC was negatively related to depressive symptoms (B = −0.22, p < 0.001). A significant moderation effect was found between OHSV and FaC when predicting depressive symptoms (B = −0.20, p = 0.005). Probing the significant interaction effect further revealed that the unstandardized simple slope coefficients were bsimple = 0.62 (SE = 0.09, p < 0.001, at −1 SD) for low, bsimple = 0.42 (SE = 0.08, p < 0.001, at 0 SD) for moderate, and bsimple = 0.21 (SE = 0.13, p = 0.101, at +1 SD) for FaC, indicating that the positive relationship between victimization and depressive symptoms was weakened as FaC increased from low to moderate levels (Fig. 5).
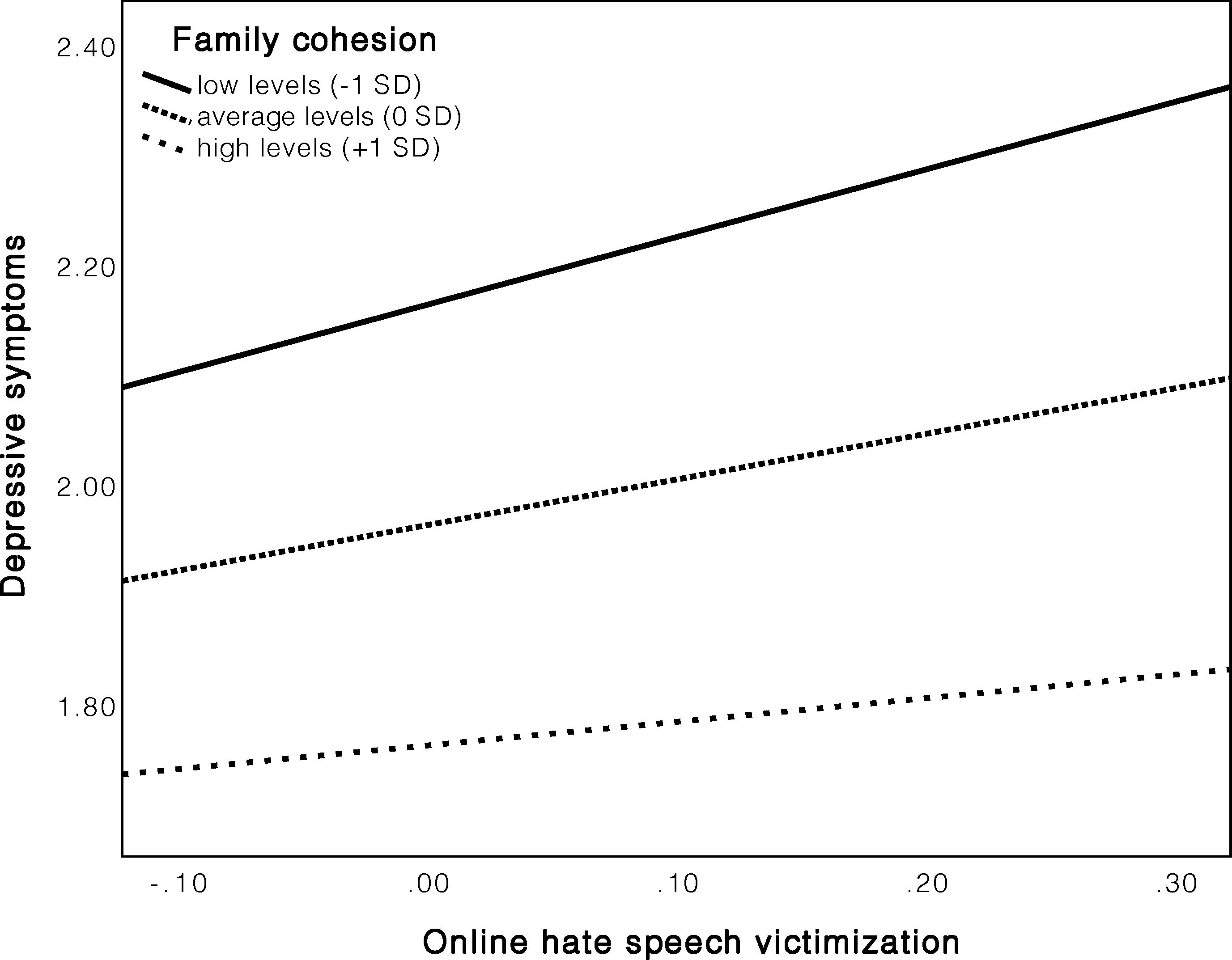
Graphical representation of the moderation of family cohesion on the association between OHSV and depressive symptoms. FaC, family cohesion.
Discussion
Given the rise of online hate speech, it has become increasingly important to examine whether OHSV is associated with adolescents' psychological adjustment and which factors mitigate the negative effects of OHSV. Addressing these gaps in the literature, we investigated the relationship between OHSV and depressive symptoms, and the role of resilience in buffering the deleterious effects of OHSV on depressive symptoms in a large sample of Spanish adolescents.
Regarding our first hypothesis, we found that OHSV was positively correlated with depressive symptoms. This finding extends previous research on negative impacts of OHSV on adults' mental well-being11,15,16 This finding is also in line with the extant literature on the positive relationship between online bullying victimization and depressive symptoms.17–23 The relationship between OHSV and depressive symptoms was moderate, similar to the effect of online bullying victimization on depressive symptoms found in a current meta-analysis. 22 We conclude, therefore, that OHSV should be considered as severe as online bullying victimization. Parents and professionals who work with young people (e.g., social workers, teachers, school psychologists) should be made aware about the potential damage that OHSV can cause and offer victims the help they need to overcome such experiences.
Consistent with our second hypothesis, we found that resilience moderated the relationship between OHSV and depressive symptoms. More specifically, our findings suggest that the positive relationship between OHSV and depressive symptoms becomes weaker when resilience increased. This finding is aligned with research showing that adolescents' ability to cope with online hate is related to their mental well-being 24 and research revealing that family support was related to adolescents' ability to cope productively with OHSV. 25 In addition, this result is in line with the resilience framework 27 and with empirical research on online bullying victimization.28–30
This study adds to the literature by showing that all three resilience factors, namely individual factors (i.e., SoC, PeC, StT), familial factors (i.e., FaC), and a supportive environment outside the family (i.e., SoR) play an important role in understanding the relationship between OHSV and depressive symptoms.
All five moderation effects were small in magnitude, ranging between −0.18 and −0.24, indicating that all five variables had the same buffering effect. Consequently, anti-hate speech intervention strategies should be holistic and should not only focus on increasing personal strengths of adolescents but also on creating social environments in which adolescents find warm, nurturing relationships within and outside their family. Comprehensive, school-based programs directed at online hate speech prevention should not only include lessons on the harmful impacts of online hate speech for the victims but also contribute to adolescents' competences and SoR by, for example, strengthening social relationships among peers or teacher–student relationships.
Limitations and future directions
Although this study contributes to our understanding of OHSV among adolescents, some limitations of the study need to be acknowledged. The sample used in this study was large, but it cannot be considered as representative. Therefore, followup research should investigate the present research questions with representative samples to increase the generalizability of the findings.
Although it appears plausible that depressive symptoms are a consequence of OHSV, we cannot proof the temporal ordering of this relationship with our cross-sectional data. Therefore, longitudinal research is needed to understand whether depressive symptoms are a consequence or a risk factor of OHSV, or even both. Previous meta-analyses on the relationship of online bullying victimization and depression yielded support for a bidirectional relationship.21,23 Hence, similar findings can be expected for OHSV and depressive symptoms.
Another limitation of this study refers to the use of single items for measuring OHSV. Single-item measures are often accompanied by typical measurement problems (e.g., low content validity, sensitivity, and lack a measure of internal consistency reliability). Furthermore, the use of multi-item measures would allow to investigate various facets of OHSV (e.g., covert/overt; private/public attacks) in relation to depressive symptoms. Therefore, future research should deepen our understanding by developing such instruments for measuring OHSV.
Finally, initial research indicated that online hate speech and online bullying co-occur. 34 Hence, follow-up research should investigate whether similar findings can be found between OHSV, depressive symptoms, and resilience after controlling for online bullying victimization. In addition, follow-up research could investigate if victims of both forms of online victimization show a higher probability of depressive symptoms than exclusive online hate speech or online bullying victims.
Conclusion
This study investigated the relationship between OHSV and depressive symptoms as well as the buffering effect of resilience in this relationship. Findings showed that OHSV and depressive symptoms were positively associated, and that all five resilience factors (i.e., SoC, PeC, StT, SoR, and FaC) moderated this relationship. It thus appears crucial to include interventions that encompass both individual and contextual developmental assets when attempting to tackle online hate speech. Although our correlational study is an important first step to understanding the detrimental effects of OHSV on adolescents' mental well-being, longitudinal studies are needed to understand how OHSV impacts adolescents over time and which role resilience might play in this temporal order.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for this study was provided to Manuel Gámez-Guadix by the Ministerio de Ciencia e Innovación (Spanish Government), grant RTI2018-101167-B-100.