
Abstract
The current study aimed to identify specific feedback mechanics and psychological processes that may contribute to positive outcomes in biofeedback applications for anxiety regulation. Specifically, using a dismantling study design, the unique impact of visualizations that directly mirror users' breathing was examined in relation to anxiety regulation as well as locus of control and self-efficacy. Following an anxiety induction, participants (N = 67) were randomly assigned to play one of two variations of a biofeedback video game. In both versions, players' in-game movement was contingent on their breathing; however, the experimental condition additionally included visualizations that directly mirrored players' breathing. Changes in self-reported state anxiety and physiological arousal were measured as well as the level of internal control and self-efficacy participants experienced while playing the game. Results showed that all participants were able to effectively reduce their anxiety and arousal, but no condition differences were found. Implementing mirroring visualizations did not contribute to individuals' ability to self-regulate nor their self-efficacy or locus of control above and beyond receiving feedback based on their in-game movement. Overall, individuals who experienced higher self-efficacy and a stronger internal locus of control were better able to regulate their anxiety, but no clear links were found with changes in self-reported physiological arousal. In light of these results, we recommend the continued exploration of the role of specific design choices and intervention components as well as underlying mechanisms of change in biofeedback interventions, especially pertaining to how individuals perceive themselves and their ability to change.
Introduction
Biofeedback training has been effectively used to treat anxiety1–3 by facilitating interoceptive awareness (i.e., the ability to notice, monitor, and accurately interpret physiological signals) and self-regulation. 4 Biofeedback training works by measuring physiological changes (e.g., heartbeats per minute) and using visualizations such as interactive graphs or simple animations to mirror these changes. 4 In addition, conditioning and reinforcement are used to encourage participants to keep their physiological activity at an optimal level (e.g., by playing a pleasant sound when the desired heart rate has been reached).5,6
While biofeedback training has been shown to be an effective method to help people manage their anxiety, most studies solely focus on measuring outcomes such as changes in anxiety or physiological modalities (e.g., heart rate variability). As a result, the underlying mechanisms are still largely unknown, especially when it comes to psychological processes.3,7,8 Furthermore, fundamental design issues related to biofeedback have been largely overlooked, such as the specific ways in which feedback and reinforcement are provided.9,10 Various forms of physiology can be used as input for biofeedback such as breathing rate, muscle tension, or heart rate variability.
Moreover, there are various ways in which changes in physiology can be communicated or reinforced. For example, a change in breathing can be expressed numerically by continuously displaying the current breathing rate. Alternatively, a moving animation can be used (e.g., a bar that moves up and down) that mirrors when and how quickly someone inhales and exhales. These choices in feedback mechanics and input modalities in the design of biofeedback interventions may all influence participants in different ways. To address these knowledge gaps and to maximize the effectiveness of future biofeedback interventions for anxiety, the current study aimed to (a) identify what specific biofeedback mechanics could be linked to improvements in anxiety and (b) uncover what psychological processes may play a role.
Visualizing physiological change lies at the core of biofeedback training and is meant to enhance interoceptive awareness, 4 a core feature of emotion regulation. 11 However, the extent to which these visualizations increase interoceptive awareness and, in turn, positively influence anxiety regulation may depend on how these changes are appraised. Highly anxious individuals are often overly sensitive to physiological signals and tend to interpret them in an overly negative manner, which exacerbates their anxiety.12–14 Furthermore, they often are not capable of effectively regulating their emotions in stressful situations. In this study, we therefore examined several appraisal processes that may be tied to the effectiveness of biofeedback interventions.
Self-efficacy, which refers to someone's belief in their ability to deal with certain situations or to complete certain tasks, is strongly linked to psychosocial functioning. 15 In fact, low self-efficacy is linked to increased anxiety16–18 and the maintenance of affective disorders. 19 Self-efficacy is derived from performance indicators (e.g., successes and failures) as well as physiological indicators, 20 both of which are addressed in biofeedback training by continuously visualizing participants' ability to successfully regulate their physiology. Some evidence shows that biofeedback can influence self-efficacy21,22; however, which specific aspects of biofeedback interventions are linked to this change has not been explored.
Self-efficacy is closely related to the concept of locus of control, 23 which concerns the extent to which someone believes that outcomes are determined by one's own actions (internal locus) or by external factors (external locus). 24 Whereas self-efficacy is a judgment of capability, locus of control focuses more on outcome contingencies. Highly anxious individuals often have a low internal locus of control, 25 but this is hypothesized to change as a result of biofeedback training. Observing their physiology changing and recognizing that they themselves can exert control over their physiological state may lead to an increased internal locus of control, which, in turn, may decrease their anxiety as feelings of control have been linked to better outcomes in anxiety treatment.26,27
Visualizations that mirror the users' physiology are commonly implemented to facilitate learning and self-regulation in biofeedback interventions as well as certain phone-based relaxation applications.28,29 However, whether these mirroring visualizations influence self-efficacy and locus of control, and whether these appraisals relate to anxiety regulation in the context of biofeedback interventions has yet to be empirically examined.
In the current study, we examined the role of mirroring visualizations in the context of DEEP, a biofeedback video game designed to facilitate anxiety regulation.30,31 DEEP uses a combination of virtual reality (VR) and biofeedback to encourage deep diaphragmatic breathing, an effective anxiety regulation technique. 32 Players control their movement in the game with their breathing, which is measured by a belt that records the expansion of their diaphragm.
In the game environment, visualizations are implemented that mirror the players' breathing, such as a circle in the player's line of sight that increases in size when the player inhales (and the diaphragm expands) and shrinks when the player exhales. In addition, diaphragmatic breathing is reinforced by encouraging deeper and slower breaths through their diaphragm, which directly influences the ease with which players move and explore the game's immersive virtual underwater environment.
The main aim of the current study was to investigate the extent to which the mirroring visualizations in DEEP increase players' ability to regulate their anxiety and whether the presence of these visualizations would result in higher levels of internal locus of control and self-efficacy. In addition, we assessed how these appraisals related to players' anxiety and arousal. In contrast to most biofeedback intervention studies, the choice of our study design was less focused on answering whether the game would be effective in decreasing anxiety. Instead, our primary aim was to test the specific influence of mirroring visualizations as a feedback mechanic.
Therefore, instead of comparing DEEP with another intervention or a passive control group, we used a dismantling study design 33 to test the added effectiveness of using mirroring visualizations as a feedback mechanic. Specifically, we compared two prototypes of DEEP: one where players' movement was contingent on their ability to use diaphragmatic breathing, and another prototype where mirroring visualizations were implemented on top of the movement feedback.
Our first expectation was that all participants, after being exposed to a potent social stressor, would subsequently be able to successfully downregulate their anxiety and physiological arousal by playing DEEP. Second, we hypothesized that playing the prototype with additional mirroring visualizations would result in a stronger decrease in anxiety and arousal compared with playing the prototype without mirroring visualizations. Third, we expected that participants playing the mirroring visualization prototype would report higher self-efficacy and a stronger internal locus of control. Finally, we hypothesized that higher self-efficacy and internal control would be related to lower anxiety and arousal.
Methods
Participants
A total of 78 participants were recruited through the research participation system from the Radboud University. The final analyzed sample included 67 undergraduates (mean age = 21.27 years, standard deviation [SD] = 2.84) (refer Table 1 for participant descriptives and Fig. 1 for a flow diagram of the study). Participants were excluded if they did not meet the age criterium (<17 or >30 years old) or if they had participated in a previous pilot study involving DEEP. The latter criterium was automatically detected by the research participation system. Participants were compensated with one study credit or gift certificate (10 euros) for their participation. The study was approved by the Ethics Committee Social Science (id: ECSW2016-2208-412) of the Radboud University.

Flow chart depicting the study procedure.
Characteristics and Baseline Differences of Participants Allocated to the Two Conditions
Note: Table represents number (percentage) or mean (standard deviation) for each variable. Gaming frequency = average time (in hours) per week spent playing video games.
p < 0.05.
n = 31.
n = 36.
Power analysis
An a priori power calculation indicated that a sample of N = 34 would be needed to detect a medium (f = 0.25) effect with a mixed repeated-measures analysis of variance, given α = 0.05 and 80 percent power. For a two-tailed t test, a sample of N = 128 was needed for a medium effect (d = 0.5) given α = 0.05 and 80 percent power (calculated with G*Power 34 ). With our achieved sample of N = 67, medium to large between-group effects (≥d = 0.7) could be reliably detected (calculated with the pwr package in R 35 ) within our analyses.
Materials
State–Trait Anxiety
The Dutch State–Trait Anxiety Inventory (STAI-DY36,37) was used to measure participants' trait and state anxiety (both 20 items). State items (e.g., “I feel jittery”) were answered on a scale from 1 = “not at all” to 4 = “very much so.” Trait items (e.g., “I am calm, cool and collected”) were answered on a scale from 1 = “almost never” to 4 = “almost always.”
Physiological arousal
Self-reported physiological arousal was measured using the Physiological Arousal Questionnaire (PAQ 38 ) including seven questions (e.g., “Do you feel your heart beating?”), which were answered on a 9-point scale (0 = “not at all” to 8 = “very much”).
Self-efficacy
Self-efficacy was assessed with the competence subscale of the Player Experience of Need Satisfaction (PENS39,40) questionnaire consisting of three statements (e.g., “I felt very capable and effective when playing”), which were translated to Dutch using back translation and rated on a 7-point scale (1 = “do not agree” to 7 = “strongly agree”).
Locus of control
Participants' internal locus of control was measured using the self-agency subscale from the Appraisal Questionnaire (AQ 41 ). All questions (e.g., “To what extent did you feel that you could influence what was happening in this situation?”) were translated to Dutch and were answered on an 11-point scale (1 = “not at all” to 11 = “extremely”). Participants were asked to answer all questions with regard to their experience in the game.
Procedure
Participants first completed an online questionnaire with demographic questions and the trait anxiety assessment after which they were invited to the laboratory (refer Fig. 1 for full procedure). Participants were randomly assigned to the experimental or control condition by using an online research randomizer, 42 which provided a list of participant numbers with assigned conditions. In the laboratory, participants were told that they would only have a couple of minutes to prepare a presentation. This instruction and preparation phase of the public speaking task of the Trier Social Stress Test 43 has been shown to reliably increase self-reported arousal. 44
Before and after the stress induction, participants reported their state anxiety and physiological arousal. Subsequently, they were told that for practical reasons their presentation would follow instead of precede their game play session. This allowed us to observe whether anxiety in anticipation of public speaking could be regulated by playing DEEP. Participants in both conditions then played DEEP for 10 minutes after which they rated their anxiety and arousal and indicated how much self-efficacy and internal control they had experienced while playing. To play DEEP, participants wore a HTC Vive VR headset, headphones, and the DEEP controller belt, which measured the expansion (Fig. 2A) and contraction (Fig. 2B) of their diaphragm.
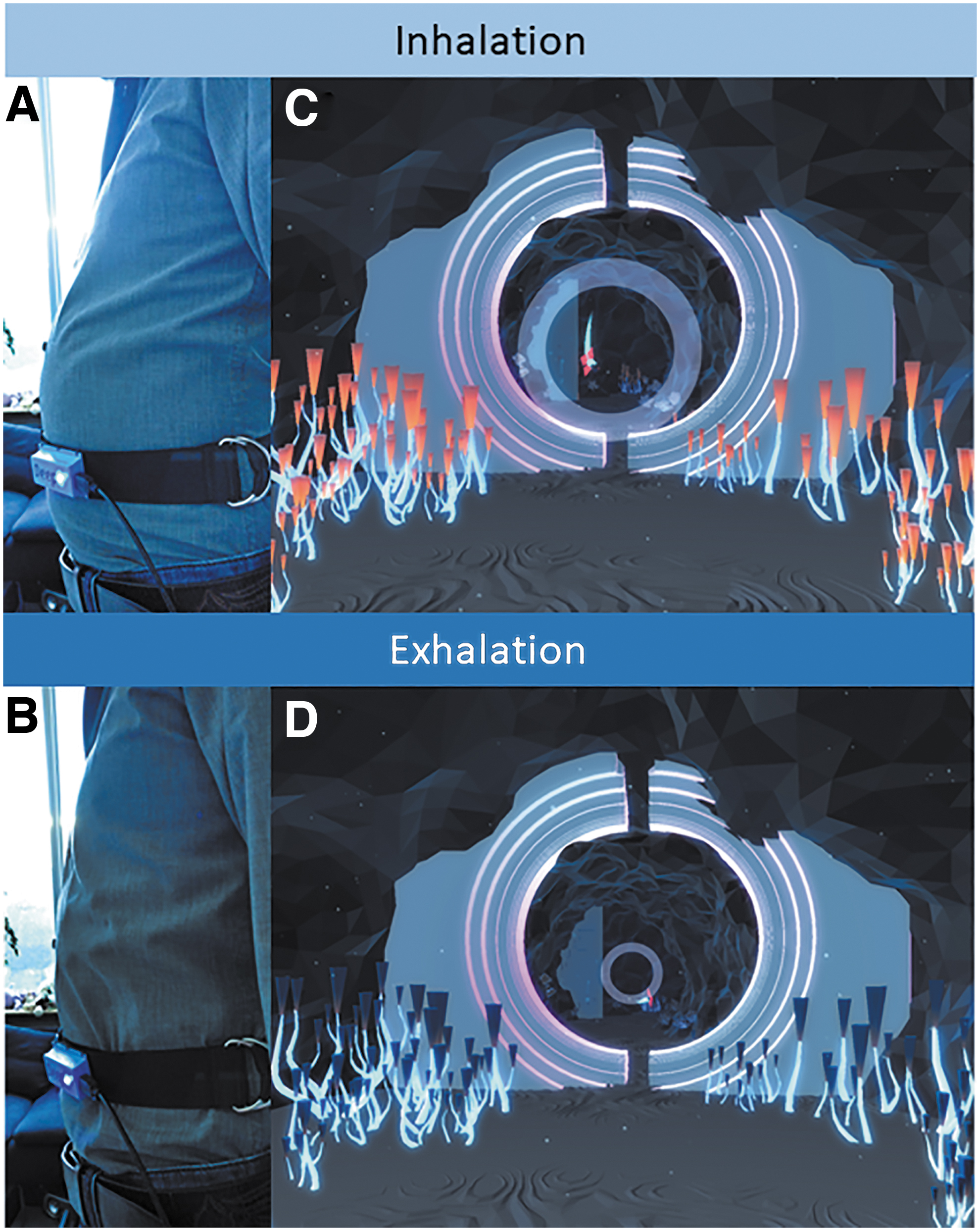
DEEP controller belt
Participants played one of two DEEP prototypes: one where players' movement was contingent on their ability to use diaphragmatic breathing or another prototype in which mirroring visualizations were added to the first prototype design. In both prototypes, deep, calm diaphragmatic breaths allowed players to stay afloat and move smoothly through the virtual underwater world, whereas shallow breathing, especially located in the upper-chest, limited their progression. In the mirroring visualization prototype, players were additionally shown a circle that grew bigger with their inhale (Fig. 2C) and smaller with their exhale (Fig. 2D) and plants which changed in size or illumination.
Data analysis
The data were analyzed using IBM SPSS Statistics (version 25). The originally achieved sample consisted of 78 participants; however, 11 participants were left out of the analyses. For six participants, this was due to a technical error resulting in the game being played on autopilot, two participants did not meet the age criteria (>30 years), and three had outliers in gaming frequency (>14 hours). This resulted in a final sample of N = 67 with n = 31 in the control and n = 36 in the experimental condition (Fig. 1). Baseline differences in participant characteristics were assessed with t tests and chi-square tests (Table 1). No significant baseline condition differences were found, except for age (Table 1), which was subsequently mean-centered and added as a covariate in all main analyses.
To establish the success of the stress induction and the change in anxiety from before to after playing DEEP, two repeated-measures analyses of covariance (ANCOVA) were performed with state anxiety and physiological arousal scores as dependent variables, time (before stress/after stress/after game play) as within-subject variable, condition (mirroring visualization prototype/control prototype) as the between-subject variable, and age as covariate.
To test group differences in appraisals, two ANCOVAs were performed with locus of control and self-efficacy as dependent variables, condition as independent variable, and age as covariate. Finally, Pearson's bivariate correlations were calculated for the relations between post-play scores and difference scores (post-play minus pre-play) of state anxiety and physiological arousal with self-efficacy and locus of control.
Results
Changes in anxiety and arousal between conditions
A significant main effect of time was found for state anxiety, F(2, 118) = 43.49, p < 0.001, ηp 2 = 0.42, as well as for physiological arousal, F(2, 118) = 24.74, p < 0.001, ηp 2 = 0.30. As expected, the within-subject contrasts revealed a significant quadratic effect of time for both state anxiety, F(1, 59) = 75.89, p < 0.001, ηp 2 = 0.56, and physiological arousal, F(1, 59) = 51.31, p < 0.001, ηp 2 = 0.47, showing an increase in anxiety and physiological arousal from before to after the stress induction, followed by a decrease in anxiety and arousal from before to after playing DEEP.
Post hoc comparisons confirmed that all time points differed significantly (p < 0.001), except the moments before the stress induction and after DEEP (p > 0.05), showing that participants' anxiety and arousal returned to baseline values. Contrary to our expectation, participants who played the mirroring visualization prototype did not show a stronger decrease in anxiety, F(2, 118) = 0.46, p = 0.63, ηp 2 = 0.01, nor physiological arousal, F(2, 118) = 0.19, p = 0.83, ηp 2 = 0.00, compared with those in the control condition (Table 2).
Anxiety, Physiological Arousal, and Appraisals Across Time Points and Conditions
n = 31.
n = 36.
Differences in self-efficacy and locus of control
Contrary to expectations, participants who played the mirroring visualization prototype did not experience higher self-efficacy, F(1, 59) = 0.02, p = 0.90, ηp 2 = 0.00, nor a higher internal locus of control compared with those in the control condition, F(1, 59) = 0.02, p = 0.88, ηp 2 = 0.00 (Table 2).
Relationships between self-efficacy, locus of control, anxiety, and physiological arousal
As hypothesized, the more self-efficacy participants experienced while playing DEEP, the lower their post-play state anxiety (r = −0.48, p < 0.001) was, and the stronger their decrease in anxiety was from before to after playing (r = −0.28, p = 0.027). Moreover, the more self-efficacy players experienced, the lower their self-reported post-play arousal scores were (r = −0.25, p = 0.041). However, unlike expected, players' self-efficacy was not significantly related to pre–post changes in arousal (r = −0.22, p = 0.076).
As for locus of control, as expected the more internal control was experienced, the lower participants' post-play anxiety was (r = −0.27, p = 0.032). Moreover, higher internal control scores were marginally related to a stronger decrease in anxiety from before to after playing (r = −0.24, p = 0.055). Contrary to expectations, however, no relationship was found between locus of control and post-play physiological arousal, (r = −0.11, p = 0.392), nor pre–post differences in arousal (r = −0.18, p = 0.145).
Discussion
The main aim of the current study was to investigate whether the inclusion of visualizations that directly mirror changes in breathing would increase individuals' ability to regulate their anxiety in the context of a biofeedback video game intervention. In addition, we examined whether the presence of these visualizations would result in higher levels of internal locus of control and self-efficacy. Finally, we assessed how these appraisals related to participants' anxiety and arousal.
To assess participants' ability to regulate their arousal, participants were led to believe that they would have to give a presentation at some point during the experiment, 43 which was meant to evoke anticipatory anxiety. As expected, participants' self-reported anxiety and physiological arousal increased as a result of this stress induction, which is consistent with previous research. 44 Furthermore, as hypothesized, participants' anxiety and arousal decreased from before to after playing DEEP, which is consistent with previous studies on DEEP.30,31 In contrast to our expectation, participants who played a prototype where feedback was given in the form of visualizations that mirrored their breathing did not show stronger decreases in anxiety and arousal compared with participants who did not receive this additional visual feedback.
Our results seemingly indicate that the presence of mirroring visualizations did not contribute to participants' ability to self-regulate above and beyond the shared aspects of both prototypes such as the fact that movement through the environment was contingent on deep diaphragmatic breathing, the relaxing music, and visual environment of the game. The reinforcement technique, which was tied to players' movement and focused on facilitating the use of deep diaphragmatic breathing in particular, may have been sufficient to help players regulate their anxiety and arousal. 32
Previous findings by Parnandi and Gutierrez-Osuna 45 found that adapting internal parameters of a biofeedback game (e.g., adapting firing speed) was more effective compared with using visualizations of players' breathing performance. However, they found that a combination of both forms of feedback outperformed either in isolation, whereas in our study, feedback based on in-game movement was just as effective as providing visual feedback in addition. This discrepancy might be explained by the difference in the specific form of feedback that was provided.
For example, in our study, players' breathing was mirrored by elements in the environment (i.e., the circle and plants reflecting players' expansion and contraction of their diaphragm), whereas Parnandi and Gutierrez-Osuna 45 showed participants a numerical expression of their breathing performance and an arrow reflecting an increase or decrease in breathing rate. This illustrates the different ways in which changes in physiology and performance can be represented in biofeedback games and can lead to varying outcomes. Moreover, it underlines the importance of examining how specific feedback mechanics and design aspects contribute to effective self-regulation in the design and validation of future biofeedback interventions.
Our third expectation that adding mirroring visualizations would result in stronger feelings of self-efficacy and internal control was not confirmed by our results. Instead, providing feedback on players' movement may be more strongly linked to these appraisals. Players could gauge how well they controlled their breathing as failure to do so resulted in their progress being halted. This more implicit feedback on control, performance, and mastery may already influence players' locus of control 24 and self-efficacy20,46,47 without explicit visual feedback being needed on top of that.
Moreover, it may be important to go beyond single-session tests and examine changes over the course of multiple sessions. In this initial session, players were still getting used to the controls and the environment. It is possible, however, that with further sessions the desire for players to receive explicit visual confirmation of their attempts to deepen and slow their breathing (e.g., as is reflected by the mirroring visualizations) would increase.
While no differences between the conditions were observed in terms of self-efficacy and locus of control, our results for the sample as a whole did indicate that the more self-efficacy participants experienced while playing DEEP, the lower their anxiety was immediately after playing and the stronger their pre- to post-play decrease in anxiety was. Locus of control was also found to be related to participants' anxiety, although less pronounced compared with self-efficacy. Specifically, a stronger experience of internal control was linked to lower post-play anxiety. In addition, a stronger internal locus of control was related to a stronger pre- to post-play decrease in arousal; however, this latter relationship was only marginally significant.
The found relationships between participants' cognitive appraisals and their experienced anxiety are in line with research indicating that self-efficacy is positively related to psychosocial functioning15,23 and that internal control is linked to better outcomes in anxiety treatment.26,27 Moreover, these findings show that it may be beneficial to explore other ways in which cognitive appraisals can be directly targeted and strengthened in the design future biofeedback interventions.
For example, as self-efficacy is mostly derived from mastery experiences and indications of progress,47,48 we suggest that dynamically adapting the intervention's difficulty to users' current level of mastery and showing occasional progress reports may further facilitate self-efficacy. 8 Moreover, creating this optimal balance between challenge and difficulty can also influence players' locus of control as it increases the likelihood of achieving a state of flow, which coincides with a strong sense of control. 49
Contrary to our expectations, while self-efficacy and locus of control were related to participants' anxiety, these relationships were less pronounced for players' self-reported physiological arousal. Higher self-efficacy was found to be related to lower post-play arousal, which is in line with a previous pilot study with DEEP where the same relationship was found. 31 However, self-efficacy was only marginally related to pre- to post-play changes in arousal. Furthermore, no relationship was found between locus of control and (changes in) self-reported arousal. It may be that cognitive appraisals are more strongly related to the emotional experience of anxiety as opposed to physiological aspects of distress.
Alternatively, in the context of a breath-based biofeedback game such as DEEP, it may be that participants' self-efficacy and locus of control are primarily linked to observed changes in breathing. However, the PAQ, 38 which was used in the current study, has only one item that focuses on breathing, thus looking at the total score may have diminished the strength of the observed correlations. Thus, we recommend for future studies to continue examining how specific cognitive appraisals are linked to specific psychological as well as physiological expressions of anxiety (e.g., breathing rate or decreased heart rate variability 2 ) within biofeedback interventions.
Limitations
There were some limitations to our study. First, as no additional passive control group was included, it is unclear whether the observed decrease in anxiety and physiological can be wholly attributed to playing DEEP. The decrease in arousal from after the stress induction to after playing DEEP was stronger compared with the arousal decrease resulting from a passive recovery period employed by Dieleman et al. 50 This provides some indication that playing DEEP would have resulted in a stronger arousal decrease if compared with a passive control condition.
For future research, we therefore recommend comparing applications like DEEP with a passive control condition. However, we also recommend the inclusion of an active control group (e.g., a different relaxation intervention or a different video game) to control for expectations and attention. A second limitation was that anxiety and arousal were assessed via self-report. Thus, we cannot exclude that there may have been physiological differences (e.g., in breathing or heart rate) between the two conditions.
A third limitation was our sample size. Our sample was sufficient to reliably detect medium within and within–between interaction effects and medium to large (≥d = 0.70) between-group effects. Thus, while our sample was sufficiently powered for the large effects, which were found for changes in arousal and anxiety, it was likely underpowered for the small effects that were found for the group-comparisons. We can therefore not exclude the possibility that group-differences in appraisal, anxiety, or arousal as a result of additional mirroring visualizations in the experimental group could have been found with a larger sample.
We recommend that future studies investigating the effect of specific biofeedback mechanics use a larger sample with more practice sessions. Alternatively, a multiple baseline design 51 could be used, which can be performed with smaller samples or a design with repeated randomizations such as the Micro-Randomized Trial, 52 which is commonly used to study multicomponent smartphone-based interventions.
A fourth limitation is that while we measured whether the addition of mirroring visualizations resulted in different outcomes in terms of anxiety as well as participants' self-efficacy and locus of control, it was not explicitly measured how this feedback mechanic was experienced by players. This information could have potentially helped us further explain the additional effect of including mirroring visualizations or the lack thereof. For future research and development of new biofeedback interventions, we therefore recommend investigating how useful and reinforcing prospective users find different forms of feedback. For this purpose, we suggest using within-subject designs so users can make direct comparisons.
A final limitation is that our study design did not allow us to fully establish the causal relationship between self-efficacy, locus of control, and anxiety. The questions about locus of control and self-efficacy were asked retrospectively to capture how participants felt during the game. However, there is a possibility that the way participants reported these appraisals were influenced by how anxious they felt after playing. For future research, we recommend using study designs that can establish causality between (changes in) cognitive appraisals and anxiety in the context of biofeedback interventions, for example, by measuring anxiety as well as cognitive appraisals multiple times over the course of a more extensive training.
Conclusions
Our study was able to provide important insights for the research and the development of biofeedback interventions for anxiety regulation, specifically regarding the influence of specific choices in feedback mechanics and the role of cognitive appraisals. Specifically, our findings show that game-based biofeedback interventions such as DEEP may help individuals to regulate their anxiety.
Moreover, individuals who experience more self-efficacy and control while playing these game-based interventions seem to experience less anxiety. Furthermore, implementing visualizations that directly mirror changes in diaphragmatic breathing in a short biofeedback session does not seem to contribute to individuals' ability to self-regulate nor their sense of self-efficacy or locus of control above and beyond using feedback mechanics based on adapting internal game parameters (i.e., linking player movement to their breathing), which are meant to reinforce diaphragmatic breathing.
Based on our findings, we recommended to explore the potential causal interplay between anxiety and cognitive appraisals in biofeedback interventions by repeatedly measuring these variables over the course of multiple sessions. If it is confirmed that appraisals such as self-efficacy mediate effective anxiety regulation, then they can be targeted in the design of future biofeedback interventions. Additionally, as we only examined the use of mirroring visualizations, we recommended to establish the influence of various other feedback mechanics by using a dismantling design or methods with multiple baselines or repeated randomizations.
In closing, we argue that expanding the knowledge about the influence of specific intervention aspects and psychological mechanisms is vital to guide the design of new biofeedback interventions that can more effectively support people's physical and mental well-being.
Footnotes
Acknowledgments
We would like to thank Owen Harris, Niki Smit (Monobanda), Andy Mooney, and Bryan Duggan for sharing the prototypes of DEEP that were tested in the current study. Furthermore, we thank Liesbeth van den Berg for piloting part of the procedure and measures. Finally, we gratefully acknowledge the assistance of Britta Suykerbuyk, Ayke Tamminga, Lisa van Heeringen, and Hiromitsu Morita during the data collection phase.
Authors' Contributions
We declare that all authors significantly contributed to the conception of the work as well as the critical revision of earlier drafts. All authors approve of the final version that has been submitted for publication and agree to be accountable for all aspects related to the accuracy and integrity of the work.
Author Disclosure Statement
During this period of research, the authors assessed early prototypes of the video game DEEP in the absence of financial incentives. However, it is not certain that this will remain to be the case in future collaborations with the DEEP development team after the public release of the game.
Funding Information
This work was supported by the Netherlands Organisation of Scientific Research (NWO) Creative Industry grant [314-99-115] as well as the as the Creative Industries Fund NL (Stimuleringsfonds).