
Abstract
The study aimed to explore the potential effect of short-term visual perceptual training based on virtual reality (VR) and augmented reality (AR) platforms in postoperative strabismic patients. We enrolled 236 postoperative strabismic patients, among whom 111 patients received VR-based training, and 125 patients received AR-based training. The stereoacuity of 1.5 m and dynamic stereopsis were improved by VR training; meanwhile, AR training exhibited more improvement in stereoacuity of 0.8 and 1.5 m, dynamic and coarse stereopsis. It was suggested that the visual perceptual training based on VR and AR technology can be potentially applied in postoperative strabismus treatment to promote the recovery of binocular vision.
Introduction
Strabismus, also known as squint, refers to any misalignment of either eye, which not only affects the appearance but also damages binocular vision function.1–3 If left untreated in children, it may influence their academic performance and have a negative impact on their self-esteem and psychological development.4–6 The prevalence ranges from 0.1 percent to 8.57 percent in different regions and races, and the pooled prevalence is 1.93 percent in a systematic review in 2019. 2
The etiology of strabismus is not definite, and there are various factors proposed to explain its origin including muscular anatomy, reflexogenic factor, abnormal binocular fusion, and genetics. 1 The treatment of strabismus includes surgery, vision therapy, prism, and optical correction, among which surgery is the main therapy.3,7
According to previous study, many cases cannot regain normal binocular visual function even after receiving a successful surgical operation.8–12 Then, postoperative binocular vision training is beneficial for rebuilding of binocular visual function.8,13
Vision therapy aims to improve the control of deviation, which refers to training of sensory fusion, motor fusion, proprioceptive awareness, accommodation, and saccades. 7 Compliance is essential for success of vision therapy applied in strabismic children. However, traditional vision training such as synoptophoric training is generally repetitive and tedious, which reduces its compliance.
In this study, we conducted a preliminary study to explore the potential effect of short-term plastic visual perceptual training based on virtual reality (VR) platforms (VR training) and augmented reality (AR) platforms (AR training) in postoperative strabismic patients.
Patients and Methods
Patients
A total of 236 postoperative strabismic patients, in West China Hospital of Sichuan University from December 23, 2019, to December 28, 2020, were recruited in this prospective study. All postoperative strabismic patients had a perfect ocular alignment that were determined through prism plus cover test by one specialist (Y.C.L.). Subjects with any other ocular disease were excluded. And subjects were also excluded if they were unable to understand and follow the procedures of the VR or AR training. This study was performed in accordance with the Declaration of Helsinki, and all guardians or adult patients provided written informed consent. The study protocol was approved by the ethics committee of West China Hospital of Sichuan University.
A total 236 postoperative strabismic patients were randomly assigned into two groups: (1) VR group: each subject underwent a 20-minute short-term perceptual training based on the VR platform. (2) AR group: each subject underwent a 20-minute short-term perceptual training based on the AR platform.
Measurement of binocular function
Inspection equipment: LG2342p computer, 24-inch wide-screen polarized light display, and examination software developed by Guangzhou Medical Instrument Research Institute (Guangzhou, China). For each examination, the subject was seated, with both eyes equal in height to the midpoint of the screen, 80 cm apart, resolution 1920 × 1080, and wearing three-dimensional (3D) polarized glasses.
(a) Fine random dot stereoscopic inspection: a random dot distribution map (54 cd/m2) with a gray background (44 cd/m2), with a size of 5° × 5°, and an E optotype (3° × 3°) consisting of random dots in the central part of the map with nonzero disparity of 400, 300, 200, and 100, respectively, with peripheral dots as a reference and always relative zero disparity. Wearing the split viewing lens, each patient needs to judge the opening direction of E-word in the figure, and press the arrow keys of the keyboard, or click the corresponding button on the interface as confirmation. There were four pictures, which were divided into 400″, 300″, 200″, and 100″, and they were judged to have fine stereopsis as long as they could perceive between 400″ and 100″.
(b) Large-scale rough stereoscopic inspection: The subject judges whether the visual mark in the figure is at the crest (protruded) or trough (concave in) and clicks the corresponding button to confirm. The correct rate is 100 percent.
(c) Motion parallax stereo vision: background high-speed movement, the subject judges the opening direction of the E word in the diagram and clicks the corresponding button of the interface as the confirmation. Among them, the high-speed movement stereopsis inspection is relatively easier to detect, the low-speed movement stereopsis is more difficult to judge, and the correct rate is 100 percent.
(d) Measurement of perceptual eye position (PEP): PEP was measured by the cross-into-circle test, which allowed the left eye to see a cross and the right eye to see a circle. The midpoint of the monitor was held 80 cm away and at the same height as the patients' eyes, with the average light source of 80 cd/m2 in white, attenuating to 50 cd/m2 when wearing 3D polarized glasses, and 30 cd/m2 in black, attenuating to 3 cd/m2 when wearing 3D polarized glasses. The size of the circle and the cross was 0.4° × 0.4° and 0.33° × 0.33° respectively (1° fixation test-object).
Patients used a computer mouse to place within what they perceived to be the circle's center, and were then instructed to click the mouse. The system automatically recorded vertical and horizontal bias by the 360° test object to observe any ocular misalignment. The minimum unit of ocular misalignment observed by this computer-controlled ocular misalignment system was 1 pixel, which equals 0.04 prism. To distinguish from the conventional eye position, we defined this bias pixel as PEP.
Methods of short-term perceptual training based on VR and AR
Perceptual training was performed by using the beta version of the computer game Diplopia Game (National Engineering Research Center for Healthcare Devices, Guangdong, China). In the VR group, the game was run in a simple VR helmet with smart phone (Fig. 1A). And in the AR group, the game was run in a simple AR helmet with a smart phone (Fig. 2A). The smart phone was equipped with an in-plane switching display (6,1″ diagonal, resolution of 896 × 828 pixels per eye), with a 90° field of view, mounted with an accelerometer, gyroscope, and magnetometer sensor for the positional tracking system. The smart phone used the Android mobile system.
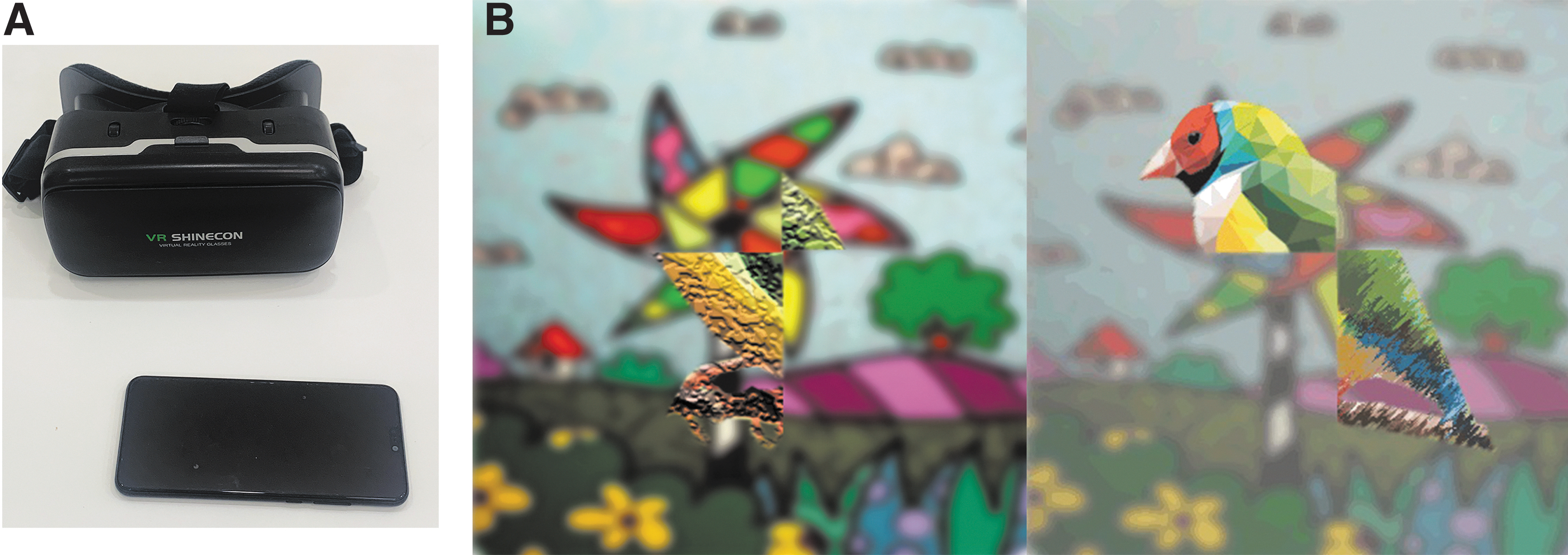
The exhibition of VR training.
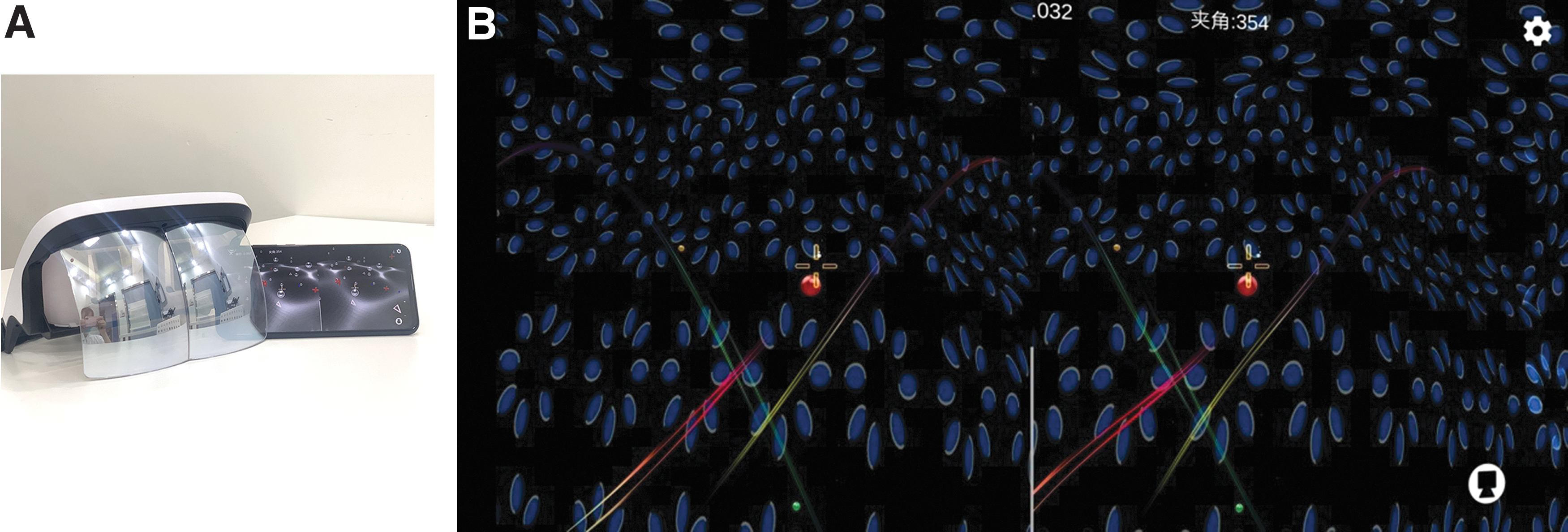
The exhibition of AR training.
In the VR group, under dichoptic viewing conditions, the central part of the picture shown was different. Some objects are seen with the dominant eye and others are seen with the nondominant eye, and the game forces the brain to use both eyes together to play. For example, in the flying bird game, the bird's upper part was visible only with the left eye, and the bird's lower part was only visible with the right eye (Fig. 1B). Every 3 seconds, the information of the left and right eyes undergoes a sinusoidal transformation. The patient can see an integrated flying bird by using both eyes.
In the AR group, under dichoptic viewing conditions, some 3D floating small balls appear randomly in the different quadrants of the visual field, and a bullet appears in the central visual field automatically. Patients wear an AR helmet and move their heads to control the bullet to break the moving 3D ball appearing in the visual field (Fig. 2B). During the training process, besides the training game, the patient with an AR helmet can also see the real-life information at the same time.
Statistical analysis
All data were represented as mean ± standard deviation. Comparisons between two independent groups were made by using a two-tailed paired samples t test (in the quantitative data including PEP and fine stereopsis) or Wilcoxon signed rank test (in the qualitative data including dynamic and coarse stereopsis). All data were analyzed with SPSS software (version 22.0; IBM, Armonk, NY), p values <0.05 were considered statistically significant.
Results
Demographics of patients
One hundred eleven patients (52 males, 59 females) were randomly assigned into the VR group, and 125 patients (62 males and 63 females) were randomly assigned into the AR group. There were no statistically significant differences in gender (p = 0.673) or age (p = 0.874) of the patients between the two groups. The demographic characteristics of the enrolled patients are described in Table 1.
Participant Characteristics
Values are means ± standard deviations for all subjects in each group.
AR, augmented reality; Number, the number in each group; VR, virtual reality.
Comparison of PEP between pre- and post-training
As given in Table 2, in the VR group, there was no statistically significant difference between pre- and post-training in horizontal PEP (p = 0.676) or vertical PEP (p = 0.783). The same happened in the AR group (in horizontal PEP, p = 0.983; and in vertical PEP, p = 0.310).
The Binocular Visual Functions Before and After Training
Values are expressed as means ± standard deviations for all subjects in each group. The asterisk represents p < 0.05.
CS, coarse stereopsis; DS, dynamic stereopsis; FS, fine stereopsis; PEP, perceptual eye position.
Comparison of fine stereopsis between pre- and post-training
As given in Table 2 and Figure 3, in the VR group, there existed a significant difference of 1.5 m fine stereoacuity between pre- and post-training. (p < 0.05). However, there was no significant difference of 0.8 m fine stereoacuity between pre- and post-training in the VR group (p = 0.184). The fine stereoacuity of 0.8 m and that of 1.5 m both statistically decreased after training in the AR group (p < 0.05).
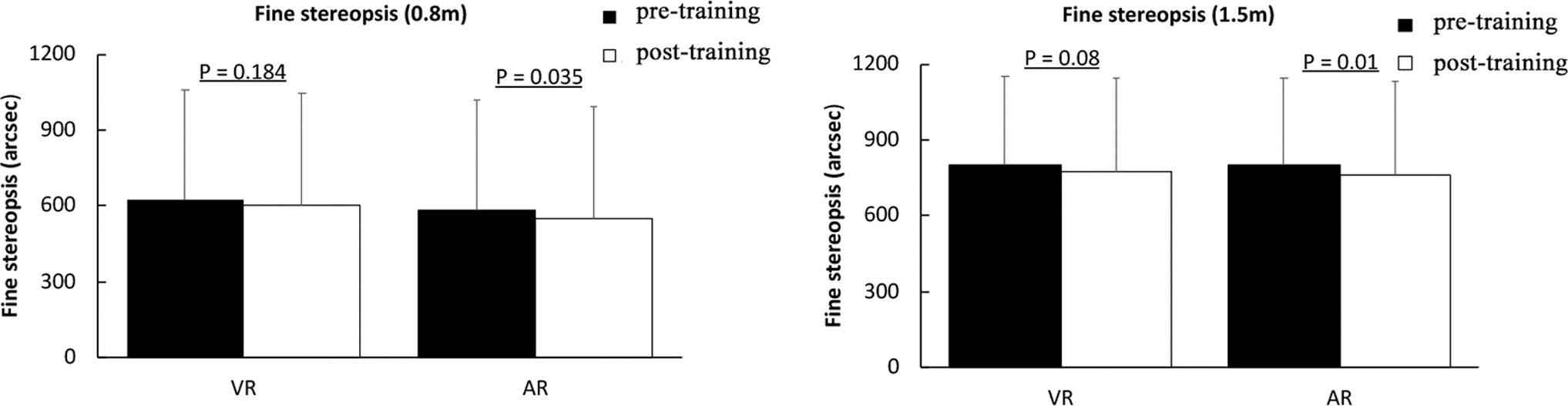
Comparison of fine stereopsis between pre- and post-training.
Comparison of coarse and dynamic stereopsis between pre- and post-training
In the VR group, only the dynamic stereopsis statistically improved after training (p < 0.05), and there was no significant difference of coarse stereopsis between pre- and post-training (p = 0.125). However, in the AR group, both the coarse stereopsis and the dynamic stereopsis statistically improved after training (p < 0.05; Table 2; Fig. 4).

Comparison of dynamic and coarse stereopsis between pre- and post-training.
Discussion
The previous studies have shown that the binocular visual function is still abnormal in postoperative strabismic patients even with successful surgical alignment. Traditionally, synoptophore and stereogram are most often used to evaluate the binocular visual function on a macro-level but not sufficient in providing a quantitative measurement of the sensory eye balance. In our study, the fine, coarse, and dynamic stereopsis as well as PEP, measured by the computer-controlling perceptual examination evaluation system under a dichoptic vision condition, were used to verify the binocular visual function of postoperative strabismic patients quantitatively. PEP is closer to the physiological state and more accurate, which is recorded by using pixel values other than traditional methods.8,14,15
Different from fine stereopsis, the coarse system serves as a type of backup mechanism, which is relied upon when the images in the two eyes have different luminance, are ambiguous, or are presented at disparities that are well beyond the fusion limit. 16 Dynamic stereopsis is more complicated and advanced than static stereopsis, and the main processing is the dorsal channel, whereas the static stereopsis is biased toward the processing of the ventral channel. 17 Thus, compared with the traditional method, our testing parameters of binocular function can provide additional information and reveal the perceptual state of both eyes in the real world.
VR presents an artificial computer-generated 3D environment, in which users become completely immersed and can readily explore and interact through multiple sensory channels: visual, auditory, or haptic.18–20 Compared with the traditional display, the 3D VR display can provide the users with more verisimilitude, which may strengthen the compliance of visual training. Different from VR, AR technology can integrate 3D virtual objects into the real world simultaneously, and also provide multiple sensory input.21–23 Besides high immersion and interaction, users can perceive the real-world environment and the digital objects in combination.
Similar to electrical or magnetic stimulation of brain areas, visual stimulation can lead to changes in the strength of synaptic connections, which is referred to as visual neuroplasticity.18,24 Temporal enhancement of synaptic connections contributes to the short-term plasticity (STP), which quickly attenuates to its initial state. Moreover, repeated visual training brings longstanding positive changes relevant to the long-term plasticity. 24 In our preliminary study, we used a series of novel methods based on the computer-controlling perceptual examination evaluation system to evaluate the binocular functions in postoperative strabismic patients. After one short-term visual perceptual training, the fine stereoacuity of 1.5 m and the dynamic stereopsis in the VR group were improved.
Meanwhile, in the AR group, more parameters including fine stereoacuity of both 0.8 and 1.5 m, as well as the dynamic and the coarse stereopsis, exhibited a significant improvement. The temporal visual feedback from VR and AR both proved the STP of binocular visual function in postoperative strabismic patients, which might predict the final training effect of AR and VR, and provided a potential alternative method of recovering binocular function after surgery for strabismus.
That AR may improve more binocular visual parameters than VR is probably the result of the added real-world visual tasks, which will be verified further in our future study. Bao and Engel believe that subjects can perform daily tasks in an environment combining real world with the laboratory world. Thus, this training can overcome the limitation of traditional perceptual training. 21
Amblyopia and strabismus are both good models for investigating neuroplasticity. With the development of VR technology, several attempts have been made to treat amblyopia through playing interactive computer games or watching 3D videos, and the treatments demonstrated various improvements in visual acuity.25–31 Compared with the study on VR-based treatment, the study on AR-based treatment was rare. In 2018, Bao et al. investigated ocular-dominance plasticity and treated amblyopic patients by an AR technique. They found the most important advantage of AR-based treatment was that it can eventually be used by amblyopic patients at home. This advantage also brought an improvement of interocular balance of patients. 32
As for strabismus, traditional vision therapy is not engaging and has low compliance. A new training method based on an intelligent VR platform was applied to strabismus treatment. In intermittent exotropic patients, with VR training, the misalignment was decreased and the stereopsis was improved. 33 In our former study, the VR technique was also used to recover the binocular function in postoperative intermittent exotropies. 8
In this preliminary study, we explored the possibility of AR and VR training for improvement of binocular vision in postoperative strabismic patients and provided a potential alternative choice of vision therapy through a short-term perceptual training. Perceptual training can reduce the suppression/noise of visual processing channels, amplify the vision signal of the strabismic eye, enhance central control, and thus remove the obstacle in the visual processing channel and repair the defect of binocular function. 33
Besides the treatment of amblyopia and strabismus, VR and AR were also applied in other aspects in vision fields, such as low vision,23,34 glaucoma,35–37 diagnosing strabismus,38,39 and testing binocular imbalance.40,41
Though the long-term perceptual training with VR or AR could improve PEP in intermittent exotropes or postoperative intermittent exotropes,8,33 one short-term training based on VR or AR had no effect on PEP of postoperative strabismic patients in this study. This seems to suggest that more time and repetitive training may enhance synaptic strength and thus improve PEP.
In conclusion, although the two eyes attain a clinically normal alignment after strabismic surgery, binocular vision has not completely recovered. The visual perceptual training based on VR and AR technology can be potentially applied in postoperative strabismus treatment to promote the recovery of binocular vision, thus enhancing the quality of life. And short-term training may predict the effect of long-term perceptual learning, which will be verified further in our future study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the program of the Health Commission of Sichuan Province (Grant No. 20PJ032).