
Abstract
Parental technological immersion during parenting activities has been shown to alter parent–child interactions. This concept, referred to as parental technoference, has the potential to affect parent–child relationships and children's health and development. This scoping review utilized the Joanna Briggs Institute (JBI) methodology to identify, describe, and summarize: (a) evidence of parental technoference on parent–child relationships, and children's health and development; (b) definitions and measurements of parental technoference; (c) research designs and methodologies used to investigate parental technoference; and (d) literature gaps. We searched MEDLINE, APA PsycInfo, Cochrane Central Register of Controlled Trials, Cochrane Database for Systematic Reviews, JBI EBP Database, Embase, CINAHL, and Scopus, as well as the reference lists of included studies for literature on parental technology use during parenting and parent–child interactions and its effects on parent–child relationships, and children's health and development. Sixty-four studies, found in 61 publications, met the review criteria. The effect of parental technoference on parent–child relationships was most studied, and findings demonstrated that parents recognized, and researchers observed, changes in parents' and children's behaviors. Adolescent self-reported mental health concerns and maladaptive technological behaviors (e.g., cyberbullying) were associated with more parental technoference, and findings highlighted safety concerns for children. Other aspects of children's development, although less studied, were also negatively impacted by parental technoference. No significant associations were found between parental technoference and children's medical and physiological health, yet these associations were the least studied. Additional research is needed to understand these associations and evaluate interventions designed to mitigate technoference harms.
With the ubiquity of mobile phones, it is difficult to escape technology in everyday activities. Mobile phones are prevalent, and an estimated 70 percent of the global population will subscribe to them by 2025. 1 Fifty-six percent of Canadians say their smartphone is the last thing they check before sleeping 2 and 31 percent of United States (US) adults never turn off their cell phones. 3 This can lead to an “absent presence,” where one is so technologically absorbed that they appear absent, 4 which may threaten communication and relationship formation. 5 Conversely, technology offers parents benefits, such as relieving boredom, connecting with others, coping with stress, and receiving knowledge.6–9 However, in a sample of 3,640 US adults, 68 percent felt distracted by their smartphone while interacting with their children. 10 Although technology offers benefits, there is potential for negative parent–child relationship repercussions.
Technoference
Technoference refers to interruptions in communication, interactions, or time together due to technology. 11 Technoference can create feelings of intrusion and can cause individuals to feel less important than the digital “other.”12,13 Technoference was first described in reference to romantic relationships, where greater technoference predicted more conflict about technology use, and technology use conflict predicted lower relationship satisfaction. 11 This concept has also been described as phubbing, referring to “phone snubbing.” 14 Parental technoference refers to interruptions in interactions between parents and children due to parental technology use 15 during face-to-face interactions, such as mealtime and playtime. 12 Parental technoference can negatively affect caregivers' attention, sensitivity, and responsivity to children,16,17 and has been associated with low parent–child communication and children's behavioral (e.g., acting out) problems. 18
We searched eight databases and reference mined relevant articles for other reviews on parental technoference and technology usage. Previous literature reviews exploring parental mobile device use and parent–child interactions, 19 parental technoference and parent (e.g., parenting) and child (e.g., behavior) outcomes, 18 and parental technoference and children's health (e.g., accidental injuries), development, and behavioral outcomes 20 have lacked a systematic process. Researchers have also conducted a systematic 21 and scoping review 17 on parental phone use and parent–child interactions and relationship quality, as well as a systematic review on parental device use and caregiving along with children's behavioral outcomes. 16 The systematically conducted reviews, however, offered little investigation of parental technoference on children's health and development, with only one evaluating the effect on children's behavior. 16
Furthermore, parental device use and technoference are not synonymous as parents can utilize devices when their children are not around (e.g., child is sleeping) or not interacting with the parent (e.g., engaged with another adult). Therefore, a comprehensive rigorous review is needed to understand definitions of (and tools utilized to measure) parental technoference, and its effects on parent–child relationships and child health and development.
Scoping reviews are used to clarify concepts, determine how research is conducted, discover evidence, and analyze knowledge gaps. 22 In contrast, systematic reviews frequently address precise questions to inform the feasibility or effectiveness of a treatment. 22 As the construct of parental technoference is nascent, we conducted a scoping review using a rigorous systematic process to broadly identify and map existing research on parental technoference and parent–child relationships and/or children's health and development for children younger than 18 years.
Review Questions
Our primary research question is as follows: What are the impacts of parental technoference on parent–child relationships and children's health and development? Secondary research questions include the following: How is parental technoference: (a) defined and (b) measured? (c) What designs and methodologies are used to research parental technoference? (d) What are the research gaps?
Inclusion Criteria
Participants
We planned to include articles on parents (e.g., unmarried, divorced, biological, adoptive) with children <18 years of age. However, we also included studies with older adolescents when children's mean ages were <18 years.
Concept
Studies on parental technoference and parent–child relationships (e.g., behaviors, attachment), child health (e.g., mental, physical), and/or developmental (e.g., motor, cognitive) outcomes were considered. During the title and abstract review, we discovered literature on parental technoference and children's technology use (e.g., cyberbullying), and included these studies as a health-related outcome. Parental technoference was identified as parental technological device (e.g., tablet, smartphone) utilization, excluding television, during parent–child interactions.
Context
Articles on parental technology use in the context of when parent–child interactions are expected (e.g., during mealtime) and its impacts on the outcome measures listed above were included around the world, with no setting limitations.
Types of studies
Primary quantitative and qualitative studies, reviews (i.e., systematic, scoping), conference abstracts, and dissertations written in English were included with no publication date limitations. Gray literature, popular literature, letters, editorials, and opinions were excluded.
Methods
We utilized the Joanna Briggs Institute (JBI) scoping review methodology to guide our review,
23
registered the review (
Search strategy
From December 2020 to January 2021, we completed a comprehensive search with an academic health sciences librarian (K.A.H.) in eight databases (i.e., MEDLINE (R) and Epub Ahead of Print, In-Process and Other Non-Indexed Citations, APA PsycINFO, Cochrane Central Register of Controlled Trials, Cochrane Database for Systematic Reviews, JBI EBP Database, and Embase [OVID], CINAHL Plus with Full Text [Ebsco], Scopus). We identified relevant articles through a discovery search; key text words from titles, abstracts, and index terms informed the final search, which focused on three main concepts: parents, children, and technoference (Supplementary File S2). The search was finalized in APA PsycINFO and translated for other databases.
Study selection, data extraction, and analysis
The resulting articles were uploaded to Covidence (
Overall, 61 reports (4 articles included more than 1 study) were included; the inclusion criteria were met for study 1 and 2 in 3 reports26–28 and study 1 in the fourth report. 29 See Figure 1 for the study selection process. Frequency counts on study characteristics and methods are presented in Tables 1 and 2, and definitions and outcome measures are presented in Table 3.
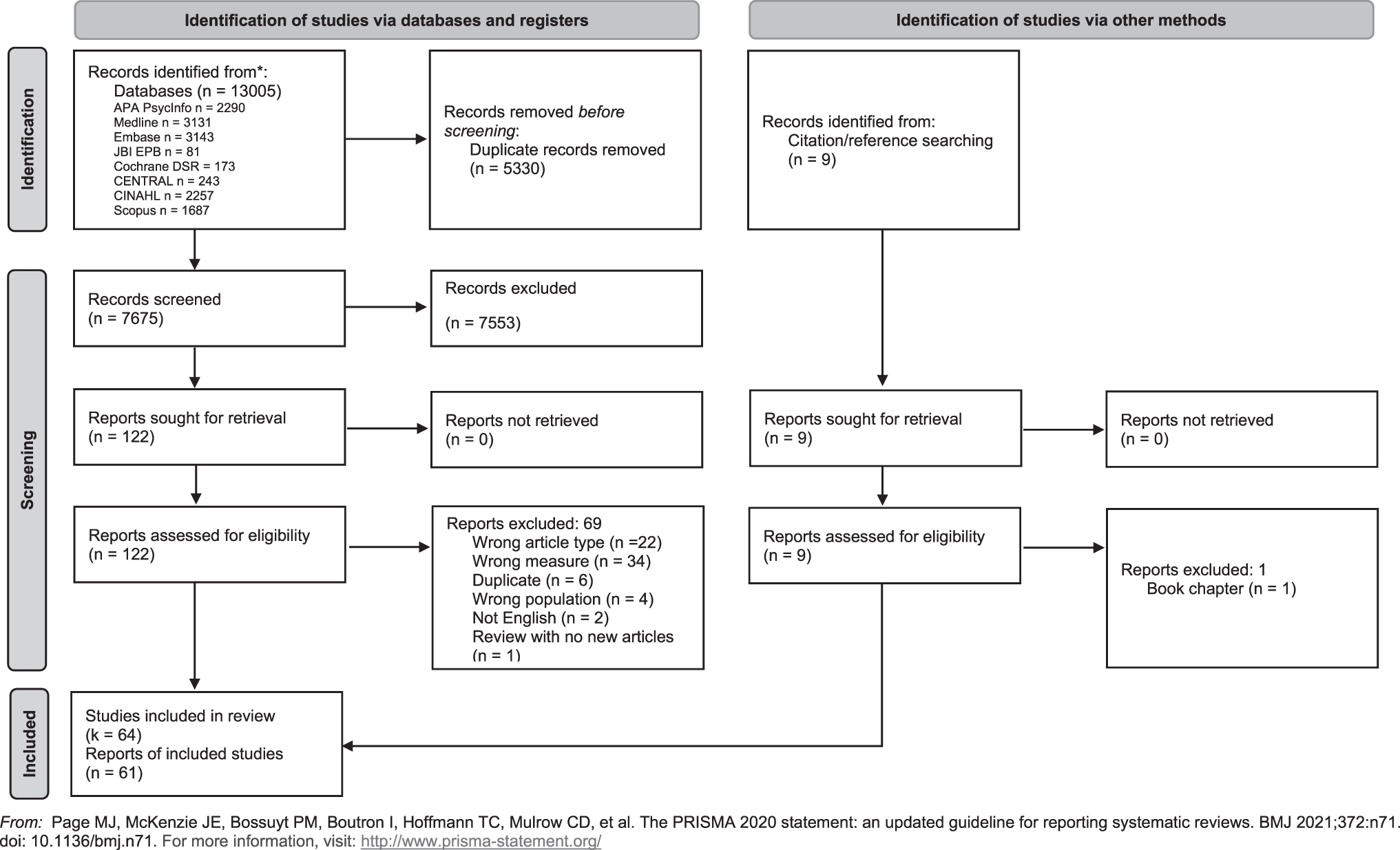
Preferred Reporting Items for Systematic Reviews (PRISMA) diagram.
Study Characteristics
Included in two categories.
Infants <12 months only.
Technoference Measures
Technoference Definitions and Outcomes
MDU, mobile device use; PMPU, problematic mobile phone use; PSD, parental screen distraction.
Results
Study characteristics
This review includes 61 reports, comprising 64 studies. Articles were published between 2008 and 2021, with only two30,31 published before 2015. Most studies were conducted in the United States (k = 32) and China (k = 17), and sample sizes ranged from seven mother–infant dyads 32 to 4,213 high-school students. 33 Quantitative studies (k = 49) were most commonly conducted. Out of 43 studies that specified parental role/gender, only 1 included slightly more fathers (56 percent) than mothers. 34 Five studies included parents and nonparental caregivers, such as grandparents 6 and nannies. 35 Parental technology use while caring for or interacting with children was most frequently defined as technoference (k = 19), followed by phubbing, a portmanteau of “phone” and “snubbing” (k = 17). For consistency, we utilize parental technoference throughout this review. Parent–child relationships comprised the most studied outcome, followed by child health, technology use, and development (Fig. 2).
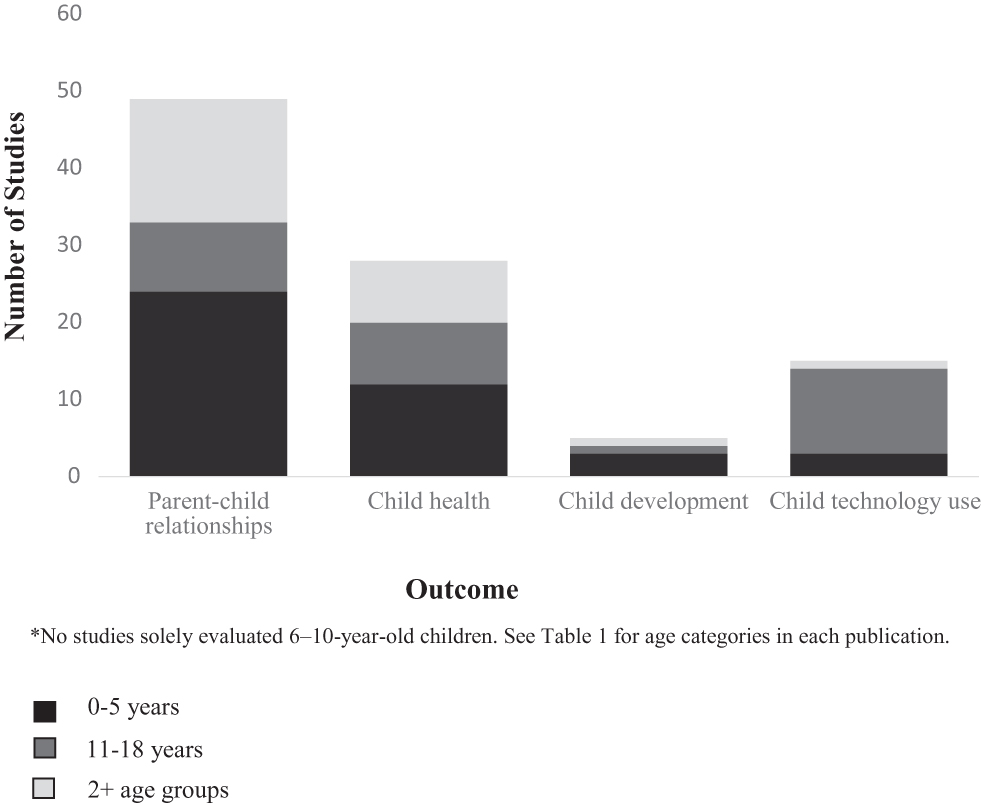
Outcomes measured by age.
Most studies evaluated parental technoference with smartphones, cell phones, or mobile phones; 19 studies evaluated more than 1 device, yet the devices (e.g., smartphone vs. tablet) were not differentiated in analyses. See Figure 3 for technological devices in these articles.

Technological devices reported in articles.
Methodological quality
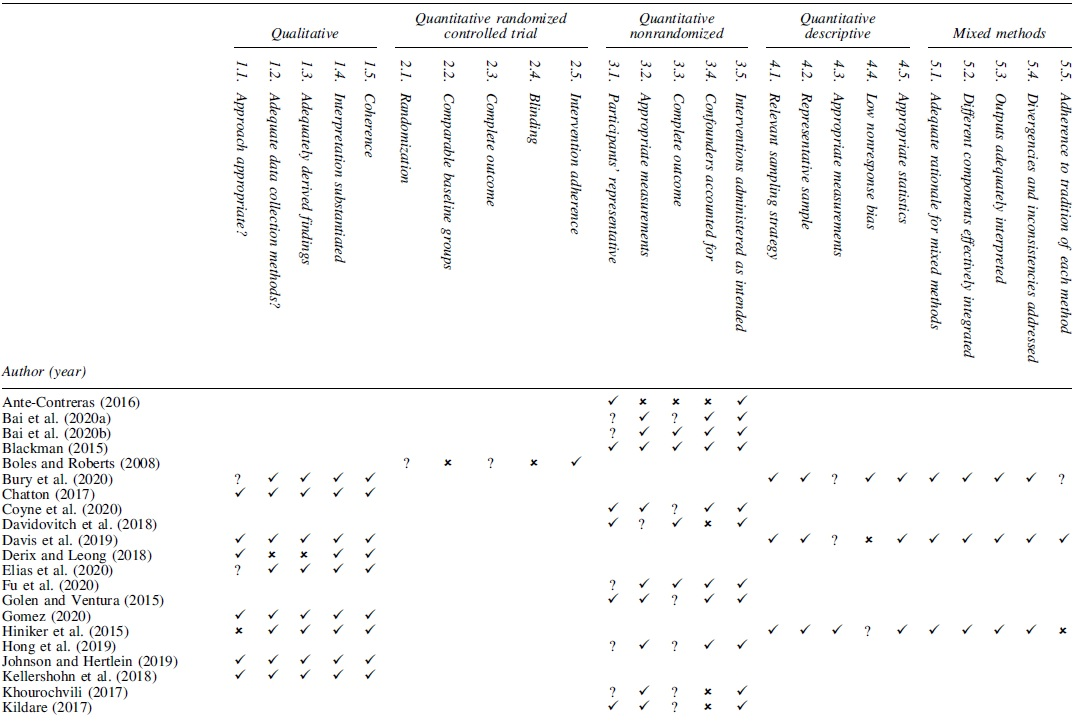
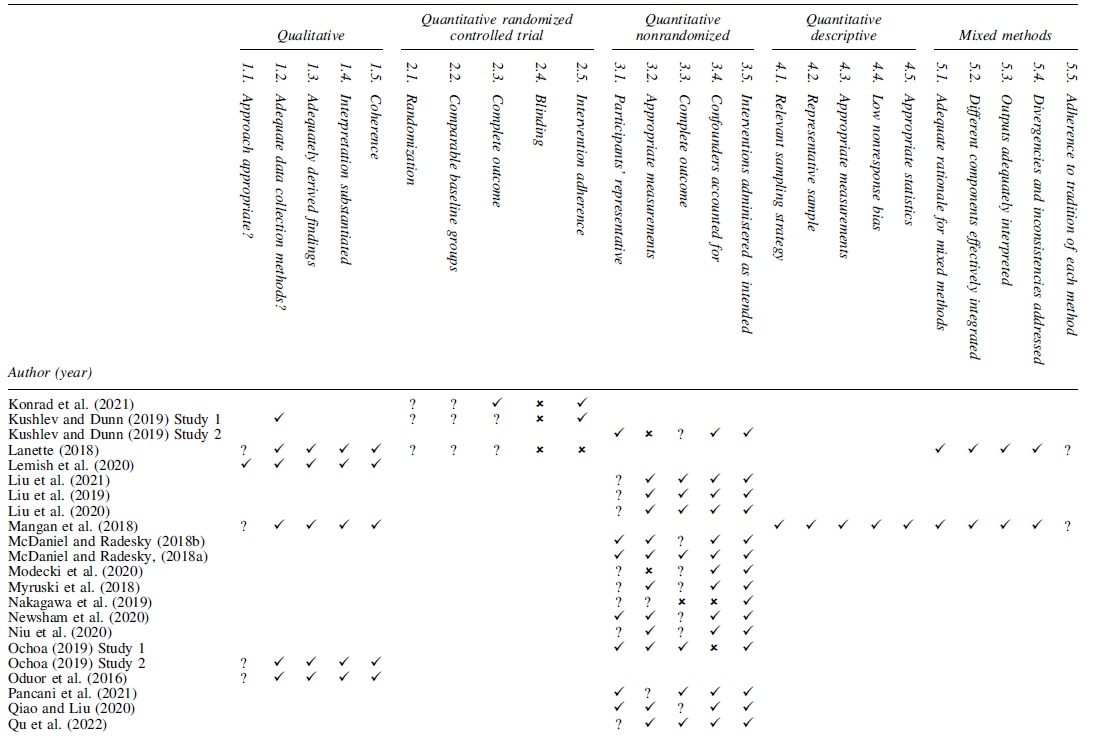
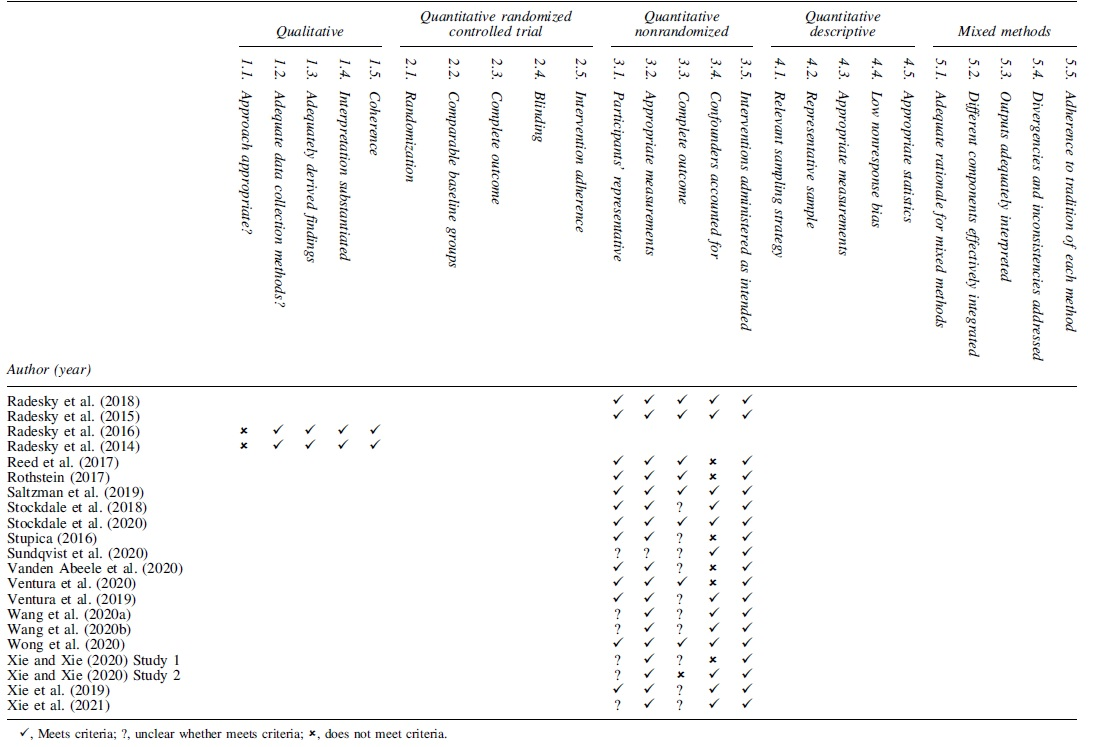
Quality appraisals are presented in Table 4. Of 11 qualitative studies and 5 qualitative components in mixed-methods studies, 6 fulfilled all MMAT criteria; 6 studies did not indicate the methodology used and 3 utilized a methodology (i.e., Grounded Theory) that did not align with its aims (e.g., theory not established). No randomized controlled trials met 100 percent of the criteria. Seven of 45 nonrandomized studies met all the criteria; 33 of these studies accounted for confounders (e.g., mediation). One-fifth of the mixed-methods studies met all the criteria. A.J.T. and S.M. appraised half and J.K. independently assessed each study. J.K. attained 95 percent inter-rater reliability with A.J.T. and 89 percent with S.M. Disagreements were discussed between J.K., A.J.T. and S.M. to reach a consensus.
Critical Appraisal with Mixed-Methods Appraisal Tool
Parental technoference measurements
Researchers observed parental technoference in playgrounds27Study1,35–40 and restaurants,27Study1,31,37,41 during medical40,42 and laboratory visits,43–45 and at home.44,46 In public settings (e.g., playground, waiting room), 42 percent 40 to 84 percent 42 of parents used their phones with their child present. Two studies reported low phone use duration at playgrounds, with almost 30 percent of parents using their phone for <10 seconds 35 and 58 percent for <5 minutes. 39 In contrast, 31 percent utilized their phone for ≥50 percent of the time in a waiting room 42 and for 40–100 percent of the time in restaurants and playgrounds. 37 Parental technology use occurred less frequently (23–34 percent)44,45 and for minimal duration 46 during recorded home and laboratory meals.
Twelve studies quantified parental technoference (e.g., hours)12,28Study2,29,32,47–53 and guilt regarding technoference. 54 Parental daily technoference ranged from 0–1 to 5 hours,48,49,55 and ≥75 percent of parents utilized devices during parent–child interactions, according to parents12,32,47,51 and adolescents. 53 In contrast, only 15 percent of parents reported being likely/very likely to use their phone while playing with their child in one study, 50 yet another found that parental device use occurred often during playtime and mealtimes. 52
Parental technoference was assessed with surveys. Adaptations to the Partner Phubbing Scale, 56 often named the Parental Phubbing Scale,14,57–61 were utilized in 11 articles; mean scores ranged from 2.42 to 2.97 on a 5-point Likert scale (higher scores = higher technoference).14,26Studies1 and 2,57,58,60–65 Of note, Pancani et al.'s 59 Parental Phubbing Scale appears slightly different than the other Parental Phubbing Scales. A modified Generic Scale of Being Phubbed 66 was utilized in three studies; mean scores ranged from 2.27 to 2.35 on a 7-point Likert scale (higher scores = higher technoference).33,67,68 Four tools by McDaniel and Coyne11,69 were integrated to measure parental technoference,12,15,51–53,70,71 McDaniel and Radesky's tools 12 were revised to create the Distracted Parenting Scale, 72 and Kildare 73 modified the Media and Technology Usage and Attitudes Scale. 74 Others developed the Maternal Distraction Questionnaire 29 and questions to assess parental phubbing. 75
In five studies, minimal questions assessed parental technoference.32,47,48,76,77 Although Cronbach's alphas were frequently provided, other reliability measures (e.g., test–retest) were lacking. Two reports focused on the development and validation of parental technoference tools,29,59 and validity (primarily confirmatory factor analysis) was assessed in seven other reports.15,26,58,61,63–65
Parent–child relationship
Still-face findings
Parent–child interactions were evaluated through modified still-face exercises, 78 with mobile devices used to create parental technoference.50,55,73,79,80 Parents demonstrated high disengagement cues. 79 Infants demonstrated high disengagement, distress, 79 self-comforting, object orientation, and escape behaviors,73,80 and a low-positive55,73,80 and high-negative affect during parental technoference.50,55,73,80
Parent–child interactions
Parent–child interactions were observed covertly in naturalistic settings (e.g., playgrounds, restaurants); themes were derived from observations31,35,37,38,41 and parent–child interaction coding schemes were created27Study1,40 or adapted.36,39 Only three studies included children older than 6 years,31,35 with children up to 12 years included in one study. 41 During parental technoference, parents demonstrated low parent–child play 36 and engagement, 30 minimal attentiveness and responsivity to their children's bids for attention and emotional needs, little eye contact with their child, and some ignored27Study1,31,35,37,38,40,41 or responded harshly to their child.31,37,38 In contrast, one study observed infrequent occurrences (4 percent) where parents ignored their child's bids for attention. 39
Children's responses to parental technoference were also observed in covert studies27Study1,31,36,37,40; children exhibited limit-testing behaviors (e.g., hitting),31,37 withdrew/occupied themselves, 37 did not make 31 or increase bids for attention, 40 and showed limited positive emotions.27Study1 In one study, similar parent–child verbal interactions occurred during parental technoference compared with no device use, 36 and another reported more frequent parent–child communication when parents were not distracted with technology.27Study1
Feeding interactions
Feeding interactions were evaluated in consented mealtime observations in laboratory or community settings,32,43–45,81 at home,44,46 and with parental interviews 49 and a survey.29Study1 Most studies focused on infants and toddlers, 46 with two assessing children at ∼6 years of age.44,45 In studies with infants, lower maternal sensitivity 43 and lower cognitive growth fostering 81 were observed during maternal technoference. Maternal technoference was associated with certain parenting feeding styles (e.g., pressuring) and lower infant food enjoyment.29Study1 In contrast, no significant relationship was found between parental technoference and maternal feeding responsiveness in 18- to 24-month-old children. 46 Parents also reported infant responses (e.g., pinching breast, stopping feed) to technoference 49 and believed changes occurred in their baby from smartphone use while breastfeeding. 32
At ∼6 years of age, fewer child-directed encouragements and verbal interactions were observed during parental technoference versus no device use, 45 and lower sensitivity, richness of perceptions, and parenting reflectivity were observed in mothers who engaged in technoference (vs. those who did not actively use their phones) in a laboratory observation. 44
Caregiver and child perceptions of parental technoference
Parent–child relationship qualities33,57,63,64,75 and social connection were evaluated28Study1,54,59 with surveys. These studies primarily focused on children ≥10 years of age; however, one study included children with a median age of 5 years.28Study1 In the younger sample, parents reported significantly lower social connection during parental technoference compared with no technological distractions.28Study1 Parental technoference was associated with poorer reported parent–child relationship quality by adolescents,57,63,64 lower feelings of maternal acceptance, 33 and increased feelings of social disconnection among adolescents. 59 Adolescents reported feeling in competition with their parent's phone 54 ; however, parent–adolescent conversation quality was not affected when cell phones were present, but unused. 75
Parents reported technoference experiences in seven studies with diverse age groups. Parents perceived benefits to using technology (e.g., breaks), but they also identified risks, such as feeling low empathy for their child during technoference. 82 Parents felt like their phone interrupted parent–child interactions,27Study2 encouraged strong reactions to their child, 6 and reported internal conflict regarding phone use. 83 Parents also reported disengagement behaviors in themselves during phone use 84 and felt like their phone distracted and delayed their responses to their children.54,85
Attachment and bonding
Parental technoference and parent–child attachment57,60,68,76 and bonding 48 were measured with surveys. Two studies included children with varied ages (preschool, school-age, adolescence),48,76 while the others focused on adolescents. A significant association was not found between parental technoference and parent-reported value in “bonding” activities (e.g., playing with child). 48 While controlling for adolescent age, parental technoference was associated with less optimal parent–adolescent attachment. 60 Adolescents with low attachment avoidance were most likely to experience depressive symptoms with high parental technoference. 68 Higher parental technoference predicted lower parent–child relationship satisfaction by adolescents with preoccupied and fearful attachment styles. 57
Child health
Mental, emotional, and behavioral health
Parental technoference and preschool children's externalizing (e.g., temper tantrums, hyperactivity) and internalizing (e.g., sulking, peer problems) behaviors were reported with surveys.12,51,72,77 Parental technoference predicted greater externalizing and internalizing behaviors in two studies with the same sample.12,51 Parental technoference was also correlated with higher total difficulty scores on the Strengths and Difficulties Questionnaire, which measures children's externalizing and internalizing scores, 86 in two studies.72,77 In addition, parental technoference was associated with lower prosocial behaviors in preschool children. 77
Parental technoference and adolescent mental and emotional health was evaluated in 11 studies with surveys. Parental technoference was correlated with increased depressive symptoms,14,26Studies1 and 2,53,61,68 anxiety, 53 poorer general mental health, 67 and lower self-esteem 63 and life satisfaction 57 in adolescents. Parental technoference predicted greater adolescent loneliness, social sensitivity, 70 academic burnout, 67 moral disengagement, 58 civic engagement, and prosocial behaviors. 53
Physical/physiological health and safety
Parental technoference and supervision/child safety was reported in eight studies with themes derived from observational data,35,37,38 a developed coding scheme,30,87 observational checklist, 36 and surveys.47,48 All studies included preschool-aged children, and three also included school-aged children35,48,87 and adolescents. 48 At playgrounds 38 and during a baseball game, children experienced more safety risks 87 and parents did not observe safety risks 37 or supervise their child as frequently during technoference compared with not using their device. 36 In a laboratory, children's risk-taking behaviors increased when parents were distracted (i.e., computer) compared with no distractions, yet this did not reach statistical significance. 30 Parental technoference was not significantly related to parental-reported importance of child protection and general welfare, 48 yet 10 percent of parents believed their social media usage presented a safety/supervision risk for their child. 47 Parents believed brief (vs. long) device use would be less likely to affect child supervision quality 36 and that parenting practices (e.g., quick use or avoids use, waits until child is preoccupied/safe) mitigated phone use concerns at the park. 35
The impact of technoference on medical diagnoses and physiological health was evaluated in two studies with nonsignificant findings. During a technoference “still-face” procedure, no significant changes in cortisol occurred in infants. 73 No significant differences were observed in parental phone use during medical assessments for parents of preschool-aged children with autism spectrum disorder and attention-deficit/hyperactivity disorder compared with parents of children with congenital disorders. 42
Infant nutrition was evaluated in two studies. In one small study (N = 7), mothers required less time to recognize breastfeeding satiety while not using their phone compared with when phones were used 32 ; however, the study findings were not evaluated for statistical significance. In another study, infants with low orienting/regulation capacity and low surgency/extraversion consumed significantly more formula with distracted mothers (e.g., those utilizing technology or sleeping) than infants without distracted mothers. 43
Child development
Parental technoference and child development was evaluated in five studies. During a teaching episode, toddlers were less likely to learn a word if the parent was interrupted with a phone call, 88 but learning was not affected by parental texting. 50 Parents of preschool-aged children with language and motor delays engaged with their phones significantly more during medical assessments than parents with children born prematurely or with congenital abnormalities. 42 Children ran 3.66 seconds faster while playing baseball when their parents were attentive and responsive, compared with when parents were instructed to immerse themselves in their mobile device. 87 Parental technoference predicted decreases in adolescent attention control. 15
Children's technology use
Fifteen studies assessed parental technoference and children's technology use with surveys. These studies primarily focused on adolescents, with only two reporting preschool children's outcomes.51,72 In three51,53,72 out of four studies, 71 parental technoference was associated with higher media use/screen time for children and adolescents. Statistically significant positive associations were reported between parental technoference and adolescents' technoference,53,68 cyberbullying,33,53,58 and Internet gaming disorder. 61 Parental technoference also predicted increases in adolescent's mobile phone dependency,62,65 smartphone addiction,15,60,70 and problematic mobile phone use while controlling for age and gender.63,64
Discussion
The primary aim of this scoping review was to determine the effects of parental technoference on parent–child relationships and children's health and development. Of 64 included studies, 49 evaluated parent–child relationships. Findings demonstrated that parental technoference can negatively affect parent's and children's behaviors, such as infants demonstrating a negative affect during technoference still-face episodes50,55,73,80 and parents responding harshly to children during covert observations.31,37,38 Adolescent surveys highlighted negative parental technoference implications on parent–child relationships57,63,64 and attachment.60,68
Twenty-eight studies evaluated parental technoference and children's health, with adolescent mental and emotional health (k = 11) and child supervision/safety (k = 9) most studied. Parental technoference was associated with negative mental, emotional, and behavioral health outcomes, such as depression in adolescence and externalizing behaviors in preschool children. However, parental technoference was associated with greater social sensitivity, 70 civic engagement, and prosocial behaviors in adolescence. 53 As theorized by Stockdale et al., 53 it is possible that adolescents who experience high parental technoference attempt to gain their parents attention with positive (e.g., prosocial) behaviors. While supervision/safety risks were observed during parental technoference,36–38,87 Hiniker et al. 35 reported parenting practices that minimized technoference concerns. Limited research on physiological 73 and medical outcomes 42 did not reveal significant associations with technoference, possibly due to small sample sizes (N = 34 and 111, respectively).
Parental technoference affected children's technology use and development. Overall, 14/15 of the included studies found links between parental technoference and children's problematic technological behaviors. The impact of parental technoference on children's development was less clear, given the limited studies (k = 5), diverse outcomes (e.g., learning, running speed), and conflicting (e.g., toddler learning affected by calls but not texting) results.
We sought to determine how technoference was studied, defined, and measured. Authors commonly defined parental technology use during parent–child interactions as parental technoference or phubbing. Diverse measurement methods (e.g., covert and consented observations, surveys) provided knowledge breadth. However, various surveys were utilized, which limits comparisons between studies. Given that the concept of technoference is nascent, it is not surprising that questions were developed to measure technoference in some studies. However, some measures were developed without assessing their reliability or validity.
Technoference assessments may have also influenced the results. For example, lower phone use was observed in parents who provided a priori compared with post hoc observational consent 40 ; the Hawthorne effect (i.e., behaviors change with knowledge of being studied 89 ) could explain disparities between higher technoference observed in covert versus consented observations. Parental technoference was primarily attained with surveys in samples of adolescents, while observations were utilized more often with infants and young children. Although surveys offer numerous benefits (e.g., cost effective, convenient), they have drawbacks, such as the potential for recall or social desirability bias.89,90
Research has shown discrepancies between parent-reported smartphone usage and usage recorded with a smartphone application, with many parents underreporting (but some overreporting) their usage. 91 Therefore, this body of literature would be strengthened by future research comparing technoference measures (e.g., surveys to surveys, surveys to observations) to determine their convergent validity, highlight tool differences, and potentially determine gold standard measures.
We also identified knowledge gaps. Despite several observations of young children, none evaluated parent–child attachment as an outcome. We found minimal research on children's nutritional, physiological, and medical health, or development. Consistent with other literature,92,93 fathers were less represented than mothers. A consistently used, standardized observational tool to assess parental technoference and its effects on parent–child interactions was lacking, and we did not find evaluations of interventions to decrease parental technoference. In one study, parental texting and swiping were associated with lower quality parent–child interactions than simply looking at a phone screen or taking a photograph.27Study1
Future analyses could explore whether device type (e.g., smartphone, tablet) affects parental technoference behaviors or associations between parental technoference and parent–child relationships and children's health and development. Furthermore, many studies focused on white samples with highly educated (e.g., postsecondary) parents; it is important that future evaluations include diverse (e.g., income, education) demographics to aid in the generalizability of these findings.
Another noteworthy knowledge gap is related to a lack of temporality (i.e., technoference preceded outcomes) within this body of literature; of five longitudinal evaluations, only three conducted analyses with parental technoference measured before the outcome (e.g., child health).26Study2,51,63 In the other two longitudinal evaluations, parental technoference was measured at the same time as parent–child relationship or child outcomes (e.g., technology use), and other variables (e.g., demographics) were collected at another time.46,71 Additional research with evidence of temporality would assist with demonstrating causality 89 and with illuminating long-term implications of parental technoference.
Strengths and limitations
A strength of our study is that we used rigorous methods to systematically conduct this scoping review. Furthermore, we only included literature on parental technoference, as parental technology use measures do not indicate if the child is present. Although our review is broad, given the high number of studies and heterogeneity of outcomes and technoference assessments, our review is limited in depth. Future reviews could synthesize evidence of factors predictive of high parental technoference and mediating/moderating variables (e.g., child age) on parents and children's outcomes. For example, in a longitudinal study of infants, increases in maternal technoference were observed as infants grew older. 94 Furthermore, articles published after completing our search, in languages other than English, and gray literature could contribute to our findings.
Conclusion
This scoping review summarizes knowledge on the effects of parental technoference on parent–child relationships and children's health and development. Findings underscored negative behavioral changes for parents (e.g., ignored children's bids, harsh responses) and children (e.g., withdrawing, acting out), parental and adolescent perceptions of parental technoference, and children's safety risks. Studies highlighted associations between parental technoference and adolescent mental health concerns and problematic technological behaviors (e.g., cyberbullying), yet additional research is needed to understand the association between parental technoference and other aspects of children's health and development. Furthermore, all quasi/experimental studies focused on simulating technoference. Given the ubiquity of technological devices and technological benefits for families, supportive, nonjudgmental educational programs are needed to minimize the effects of parental technoference on parent–child relationships and children's health and development.
Footnotes
Authors' Contributions
J.K.: methodology, investigation, analysis, visualization, project administration, and writing—original draft. A.J.T.: investigation, visualization, and writing—original draft. S.M.: investigation, visualization, and writing—original draft. L.J.M.: conceptualization, methodology, investigation, and writing—review and editing. K.A.H.: methodology and writing—review and editing. J.L.C.: writing—review and editing and supervision. L.D.-L.: writing—review and editing. N.L.: conceptualization, funding acquisition, methodology, writing—review and editing, and supervision.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The authors acknowledge funding from an anonymous donor.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.