
Abstract
In the increasing number of medical education topics taught with virtual reality (VR), the prehospital management of ST-segment elevation myocardial infarction (STEMI) had not been considered. This article proposes an implemented VR system for STEMI training and introduces it in an institutional course addressed to emergency nurses and case manager (CM) doctors. The system comprises three different applications to, respectively, allow (a) the course instructor to control the conditions of the virtual patient, (b) the CM to communicate with the nurse in the virtual field and receive from him/her the patient's parameters and electrocardiogram, and (c) the nurse to interact with the patient in the immersive VR scenario. We enrolled 17 course participants to collect their perceptions and opinions through a semistructured interview. The thematic analysis showed the system was appreciated (n = 17) and described as engaging (n = 4), challenging (n = 5), useful to improve self-confidence (n = 4), innovative (n = 5), and promising for training courses (n = 10). Realism was also appreciated (n = 13), although with some drawbacks (e.g., oversimplification; n = 5). Overall, participants described the course as an opportunity to share opinions (n = 8) and highlight issues (n = 4) and found it useful for novices (n = 5) and, as a refresh, for experienced personnel (n = 6). Some participants suggested improvements in the scenarios' type (n = 5) and variability (n = 5). Although most participants did not report usage difficulties with the VR system (n = 13), many described the need to get familiar with it (n = 13) and the specific gestures it requires (n = 10). Three suffered from cybersickness.
Introduction
ST-segment elevation myocardial infarction (STEMI) is an acute life-threatening coronary syndrome caused by a complete thrombotic occlusion of a coronary artery branch, characterized by a peculiar electrocardiographic presentation, and representing a time-dependent emergency. 1 Appropriate therapy (primary percutaneous coronary intervention, stenting, thrombolysis) should be administered as quickly as possible to achieve a better prognosis and minimize permanent damage. 2
Nurses and doctors in emergency medical services usually follow advanced life support courses, consisting of theoretical and practical content and a final exam. 3 These courses provide specific skills to deal with cardiac arrest and peri-arrest situations, manage resuscitated patients until their transfer to an intensive care setting, and communicate effectively with the other rescue team members and the patient's family. 3 However, specific training courses to teach how to deal with STEMI patients are rare and based on role-playing simulations where different team members pose as STEMI patients, family members, or health care providers. Unfortunately, training experiences conducted by instructors suffer from high variability, issues in replicability, and subjective evaluation.4–10
In this context, virtual reality (VR) can provide important advantages such as training standardization, objective evaluation criteria, and large-scale distribution of the educational method to medical schools, emergency medical services, and hospitals.7,11–13 In contrast to other digital media, VR allows the trainees to live a highly interactive experience that allows to learn by doing in a reproduction of the real-world context in which the learned concepts and procedures will be applied. This promotes a more effective learning, according to constructivist and situated learning theories. 14 Moreover, higher immersivity in terms of display and interaction can provide benefits in terms of presence in the virtual environment (VE) and engagement of trainees.15,16 Furthermore, VR training may improve postintervention knowledge and skills compared with traditional education. 17
In recent years, the medical field showed a growing interest in VR applications and produced flourishing scientific literature.13,18–24 Moreover, the COVID-19 pandemic encouraged the adoption of this technology in medical education and training with positive effects.25,26 In the context of cardiovascular medicine, VR is changing the training approach,27–29 with simulation-based training especially used in interventional cardiology. 24 Nevertheless, to the best of our knowledge, no VR system has been yet proposed to train nurses and doctors in the STEMI prehospital management.
Therefore, this article proposes a VR training system used to reproduce scenarios representing patients with out-of-hospital STEMI. The system engages two trainees simultaneously: an emergency nurse who manages the patient in the VE and a case manager (CM) doctor in the real world. The CM can either be a cardiologist working in a coronary care unit or an emergency room doctor: they evaluate the clinical information and electrocardiogram received by the nurse, managing the patient's pathway from diagnosis to treatment. The proposed VR system uses an audit and feedback strategy. 30 This aims to encourage health care professionals to improve clinical practice by correcting behaviors not meeting standards.
Moreover, the implemented VR system is used in an institutional Continuing Medical Education (CME) accredited training course, making it a blended learning course, where, at the end of each simulation, an instructor (cardiologist) conducts a debriefing and encourages discussion among participants. The qualitative evaluation in this article concerns six editions of the course that took place between October 2022 and January 2023, in the Azienda Sanitaria Universitaria Friuli Centrale, Northeastern Italy. Among the 48 emergency nurses and 15 CM doctors who attended one of these editions, 17 participants volunteered to be interviewed about their experience with the VR system and the blended learning course. This article presents the thematic analysis of their replies.
The Proposed VR System for STEMI Training
The proposed system simulates the rescue operation of a STEMI patient in several scenarios characterized by different anamnestic data and vital parameters. The system comprises three applications used by one instructor and two trainees simultaneously:
- The course instructor uses a tablet-based Instructor Application (IA) to control different aspects of the simulation in real time (e.g., changing vital parameters) (Figs. 1 and 5B, D; Supplementary Material S1 contains a detailed description). - The case manager doctor uses a tablet-based Case manager Application (CA) that provides a phone call communication with the nurse, and displays the data sent by the nurse during the simulation (e.g., patient's electrocardiogram) (Fig. 2; Supplementary Material S1 for a detailed description). - The nurse wears a VR headset (Meta Quest 2)
31
in which a Nurse Application (NA) displays the VEs. The three VEs included in the NA and the interactions they support are illustrated in Figures 3 and 4.
VEs in the NA
The three VEs (Fig. 3) represent the sequence of real-world environments encountered during a STEMI rescue: (a) the crew room, (b) the ambulance, and (c) the patient's house.

The user interface of the Instructor Application, localized in the language of course instructors.
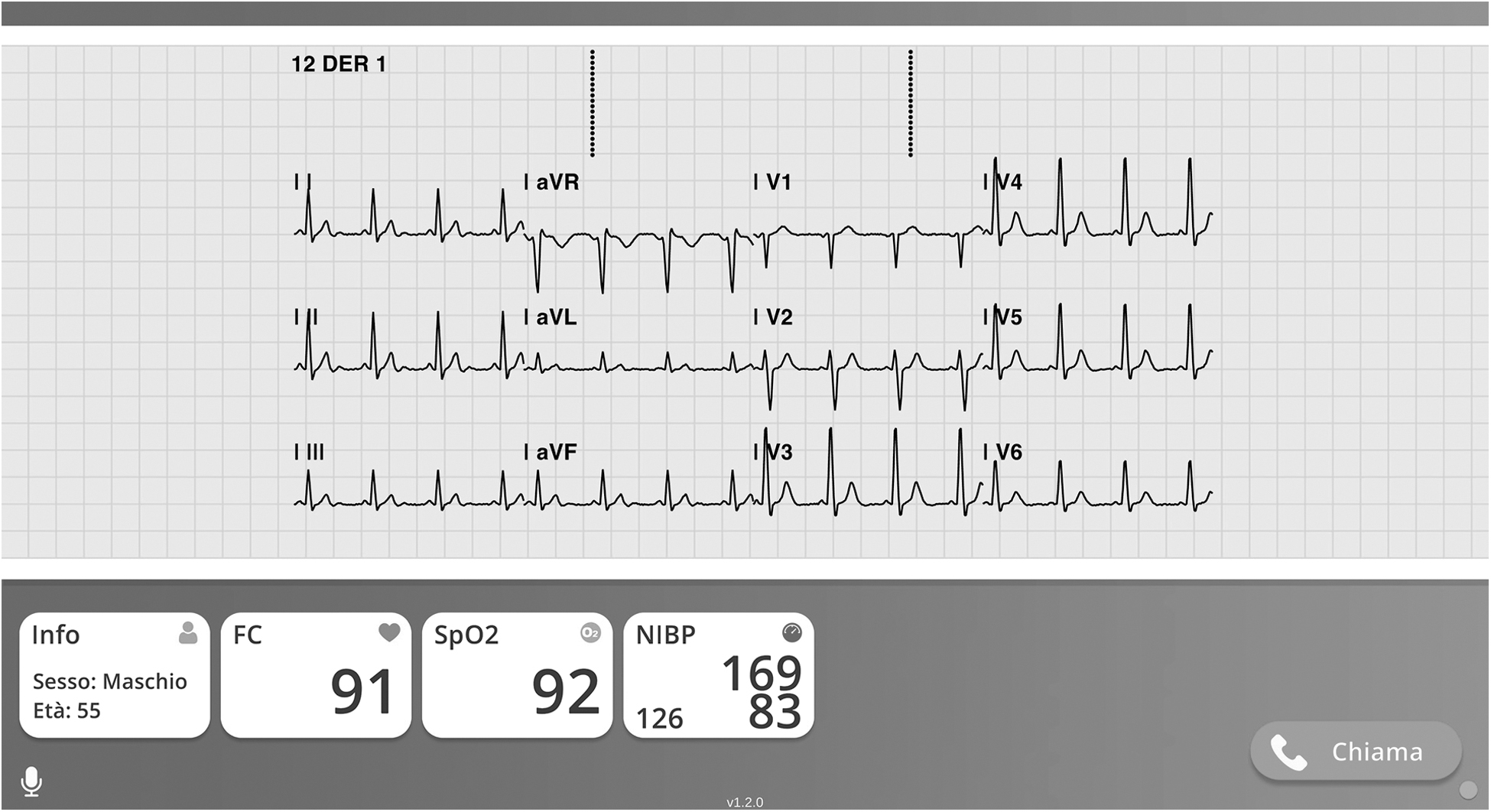
The user interface of the Case manager Application, localized in the language of case manager doctors who attended the course.

The virtual environments for nurse's training:
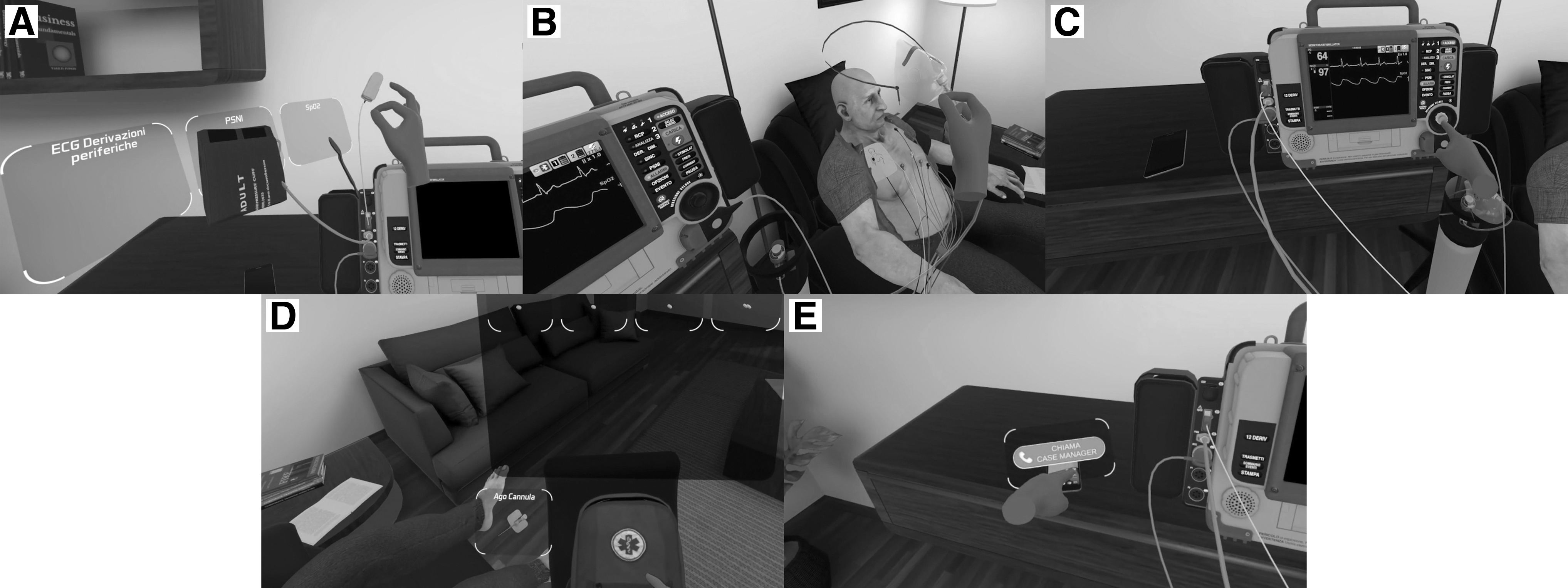
Different interactions in the Nurse Application:

Changes in patients' appearance and monitor
In the first VE (Fig. 3A), the nurse can become familiar with the VR headset and hand tracking. The VE includes a table with the medical equipment to be used in the training scenarios (monitor with defibrillator, medication bag, smartphone, oxygen tank). In this scenario, the trainee does not use yet the equipment.
In the second VE (Fig. 3B), the nurse receives briefing information while reaching the emergency scene.
In the third VE (Fig. 3C), the nurse acts on the patient. Emergency equipment is placed near the nurse to minimize the need for walking around.
Interaction
The interactions (Fig. 4) supported by the NA exploit both head and hands tracking. The simulation was designed to allow for a natural interaction with the VE. The nurse can interact with the patient and the objects in the living room VE in four different ways:
Movement. The nurse can move freely by walking directly to the desired location. We minimized the need for movement, ensuring that a simple rotation allows to reach objects and interact with them.
Proximity. Some objects are automatically activated when the nurse's hand is close (e.g., when it approaches the pouches at the side of the monitor, they display their contents as in Fig. 4A) to simplify interaction with objects, allowing the nurse to focus on reasoning and learning about the medical procedures.
Grasping. Objects can be grasped and moved by approaching them with the hand and performing the pinch gesture. Regardless of the object's size, when the fingers come in contact, the object is grasped and can be moved to the desired position. When the nurse moves the two fingers apart, the object is released. Some objects are automatically released if they are moved close to specific interaction points (e.g., the face mask in Fig. 4B automatically sticks to the patient's face).
Press. The monitor buttons can be pressed using the forefinger, as in the real world. The button lights up when the finger is sufficiently close (Fig. 4C), indicating that continuing the movement will complete the interaction.
Interactions with objects
The nurse can use all the tools typically used during a rescue:
- Monitor with defibrillator (LIFEPAK 15) 32 to monitor the patient's vital parameters. Several sensors (SpO2, band for noninvasive pressure measurement, peripheral and precordial leads and electrodes for electrocardiogram measurement, plates for external electrostimulation) are available in two side pouches attached to the monitor and must be applied to the patient to display his vital parameters. To allow for proper functionality during the rescue, the relevant monitor's functions are reproduced during the simulation: manual pressure measurement and setting automatic pressure measurement in preset time intervals; calculation of the 12-lead electrocardiogram and printing of the paper report; sending the electrocardiogram to the CM; administration of resuscitation discharges; and activation of external pacing. Figure 4A and C shows examples of interaction with the monitor.
- Oxygen cylinder and mask. A mask connected to an oxygen cylinder can be attached to the patient's mouth to administer oxygen (Fig. 4B), regulating its flow through an interface appearing at the cylinder's regulating valve.
- Medication bag. Pills, intravenous drugs, and intravenous bags can be administered to the patient during the simulation. All medications are contained in the medication bag (Fig. 4D) and can be accessed through an interface that opens as the user's hand approaches the bag.
- Smartphone. This device manages the communications between the nurse and the CM. When the nurse's hand approaches the smartphone in the scene, an interface appears to make, terminate, or answer a call (Fig. 4E).
Interactions with the patient
The nurse can interact with the patient by applying sensors, oxygen masks, and administering medications. During the simulation, the instructor impersonates the patient, responding directly to questions the nurse asks.
The patient's representation in the VE adapts according to the vital parameters set by the instructor via the IA. The patient's state is visualized through facial animation, body animation, and skin characteristics, which change according to vital parameters (Fig. 5):
- When events that are painful to the patient occur, his face takes on increasingly pronounced suffering expressions. In case of fainting or deep sedation, eyelids are lowered.
- To give more direct visual feedback, the animations the patient performs change according to his consciousness, respiratory rate, and pain.
- The parameters representing the patient's skin are changed according to vital parameters, to simulate decreased perfusion or sweating.
Use in the course
Each nurse tried one scenario using the NA during a 10- to 15-minute session. Since there were less CM doctors than nurses, each doctor used the CA for one or more scenarios. While a nurse and a CM doctor tried a scenario, all the other participants watched the simulation on a projected screen displaying the VE as seen by the nurse and vital parameters of the patient as set in the IA. Therefore, although only nurses wore the VR headset during the simulations, all participants watched all the simulations they were not involved in. This participatory course approach was meant to allow nurses and doctors to gain the most from the experience.
Methods
The study's goal was to evaluate the perceptions and opinions of nurses and doctors attending the CME blended learning course with the VR system to train participants in rescuing STEMI patients. To this purpose, we conducted an interview consisting of a sequence of structured open-ended questions (Fig. 6). Questions were intentionally general and allowed to collect information from the point of view of both nurses and doctors. Data were analyzed using thematic analysis, as described by Braun and Clarke. 33 The study was approved by the Institutional Review Board of the University of Udine.
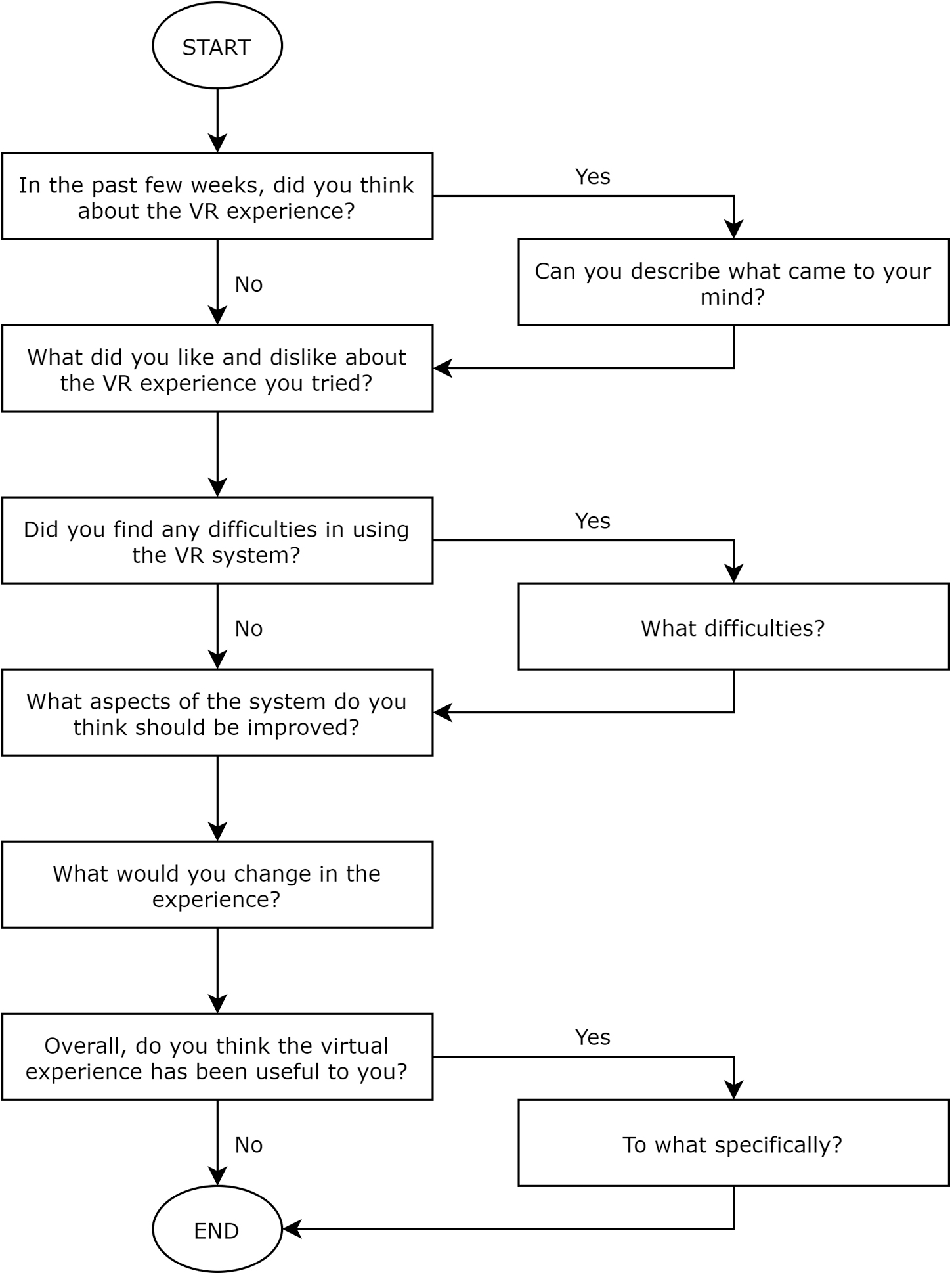
Flow diagram of questions in the interview. The interview was conducted in the language of participants. Sentences have been translated here for readers' convenience.
Participants
Twelve nurses and five doctors (9M, 8F) among the course participants volunteered to be interviewed. All but one also provided information about their age, years of experience in the role and in the emergency area, and previous use of VR (Table 1).
Participants' Gender, Age Range, Professional Role, Years of Experience in the Role and in the Emergency Area, and Previous use of Virtual Reality
VR, virtual reality.
Procedure
At the end of the CME course, we asked participants if they would like to volunteer for a subsequent interview about the experience. The volunteers left their e-mail and phone number to be contacted and book an interview time slot. After the interviewer defined the available time slots and assigned an online meeting link for each of them, two other team members contacted the volunteers and sent them the privacy policy and the consent module. After receiving the signed consent, the team members recontacted each volunteer, arranged a time slot and then confirmed it via e-mail, also including an anonymous code and the instructions to blind their identity to the interviewer (i.e., join the meeting without using a personal account, use the anonymous code and not the real name, do not use a webcam, possibly apply a filter to change the voice).
Participants were also informed that the interview would be audio recorded and then deleted after transcription. At the defined time slot, the interviewer met the participant online and started the audio recording. After briefly introducing the interview and inviting the participant to freely express opinions, taking the time needed to reason about them, the interviewer asked the open-ended questions as given in the flow diagram in Figure 6. When needed, the interviewer also asked some additional questions (e.g., what, when, how?) to clarify participants answers.
Each audio recording was saved with the participant's anonymous code and then verbatim transcribed. Two members of the research team, with different background (one in medicine and one in computer science), performed the thematic analysis by repeatedly listening to the interviews, checking the transcripts back against the original audio recording, actively reading the transcripts many times, generating initial codes using a data-driven approach to include all potentially interesting content, collating them into potential themes and subthemes, and finally reviewing and refining them to create a codebook.33,34 The final themes and subthemes were chosen to describe the entire blended learning course (ReflectOnExperience, PositiveAspect, Critique) and the VR system (Realism, UsageDifficulty), and to acquire useful information for improvement (Proposal, Opinions).
After agreeing on the codebook with the supervision of a third team member (a senior medical doctor), each of the coders independently assigned subthemes to chunks of data extracted from the interviews using the Taguette software. 35 Then, the two coders discussed on the disagreements. In case of assignments for which no agreement was found, the third team member was involved to break the tie.
Results
The coders identified 7 themes and 31 subthemes in the interviews (Table 2; Supplementary Material S2 contains examples of participants' quotes).
Identified Themes and Subthemes with Their Description and Participants Who Talked About Them
After the independent assignment of the codes, Cohen's kappa intercoder reliability was 0.76 (95% confidence interval, 0.71–0.82). After discussion, the two coders reached an agreement on all but six assignments, which were decided by the third team member.
Discussion
The methodological article by Pedram et al. recommends that VR systems should “provide motivation through enjoyment, satisfaction, engagement, attention and challenge” 36 and in other studies a positive experience was reported in terms of enjoyment,26,37 satisfaction,20,38,39 attentiveness,20,26 motivation, 20 and acceptability and feasibility. 19 The results of our study confirm those of the literature in the context of STEMI: all participants appreciated the course and the use of the VR system, and 14 of 17 said they thought about the experience in the weeks following the course (Reflect on Experience theme).
All participants contributed to at least three subthemes of the broad Positive Aspect theme and six did not find any negative aspects; the VR system was considered engaging (n = 4), as reported in other studies,19,20,40,41 innovative (n = 5) and promising for training courses (n = 10). For example, N2 reported “I think it gives you many extra things in specific courses. Because you really drop into the actual situation, and so you get yourself involved” and D3 declared “[I appreciated] the quality of the experience itself, the technique, and my experience. Moreover, the fact that I had not tried [something like that] before left me pleasantly surprised.”
In addition, some participants would have liked to try more simulations (n = 2) or more course sessions (n = 3), as reported in other studies where the willingness to use a VR system again was described.29,41
The VR system was also described as an opportunity to test knowledge and skills in a safe environment (n = 3), as positively described in previous work.21,29 Some trainees described the blended learning course as an opportunity to discuss and exchange opinions (n = 8) and to point out issues (n = 4); for example, N11 reported: “There's a big gap between those who work on the ground and those who work in the hospital. They don't understand our situation, so they don't help us when requests are made.” The presence of experienced instructors was also appreciated (n = 2), consistently with other studies, where a supervisor and peer interaction were positively considered.20,40
Moreover, most participants reported that the VR experience was highly similar to what happens during actual emergency interventions (n = 13), as in other studies. 26 For example, N5 reported: “It very much reflects reality. Of course, you emphasize a little bit more, in the sense that when you talk to the cardiologist, you lose a bit more time. However, it's a course that allows you to relate to the patient as you relate to them in the real world. And the treatments you do are the real ones, whether it's the ECG, administering the medications, or contacting the cardiologist, which is an important thing anyway” and it is interesting to note that realism was appreciated both by doctors and nurses, although only nurses lived the VR experience using the VR headset, while all participants watched it on the projected screen.
However, some participants complained about the procedures' oversimplification (n = 5) and missing actions (n = 2) and suggested to improve realism (n = 7), as in Hood et al. 41 For example, under the Realism theme, N10 reported: “Instead, the difficulty and the time to do those tasks in the real world are not like that. That is, the fact that I touched the wires and brought them to the patient was instantaneous. In a real situation, it takes me several seconds in which more questions can be processed, and I take more time to think about what I need to do. It was too fast.”
Participants also showed their interest (Proposal and Opinion themes) suggesting to modify scenarios to increase their variability (n = 5; e.g., D2: “Maybe trivially change the structure of the room or the patient lying down or finding them in bed or on the stairs”), like requested in another study, 41 and to describe infrequent situations (n = 5). Five participants reported it could be beneficial to naive health personnel (N1: “I would have done them very gladly at the beginning of my career”), whereas six reported that experienced personnel could benefit from it as a refresher training.
Nine participants contributed to the Critique theme, seven of them describing the blended learning course as not useful for them because they already knew the topics and five reporting discomfort and embarrassment because of the presence of other people (e.g., D4: “There were still many people, and somehow [I had] the feeling of being a little bit under examination).
However, four found the course beneficial to improve self-confidence and five said that they liked the challenge. For example, D2 reported: “Well, let's say [the system also helps] to understand the difficulties in interfacing with practitioners who are not your colleagues. I'm used to being a case manager for my nurses who, in short, I know off the top of my head, so I know what I [expect] when someone tells me something, and [I understand] what they mean. When I give directives, I know what is received. Doing it instead with people I don't know is definitely something that, let's say, is very helpful.” Challenge was indeed one of the aims suggested by Pedram et al. 36 and the trainee confidence following the VR training was already described as an advantage in previous studies.19,26
The Usage Difficulty theme revealed that 10 did not mention any but a few participants thought the virtual patient was too static, finding it difficult to appreciate clinical signs such as paleness or sweating (n = 3), or felt the interaction limited by the only use of sight and hearing (n = 4). Moreover, 13 reported the need to get familiar with the system and 10 to learn specific interaction gestures (e.g., N8: “I found myself not performing things that I have performed, as if my intervention was not detected by the instrument”). This happened despite all participants were invited to watch a video tutorial before attending the course. These results are consistent with those described by other authors25,40,41 and explain the recommendation for VR knowledge or practice before approaching VR systems for medical education. 40
Finally, three participants suffered dizziness or nausea; this was expected, because cybersickness represents a known drawback of VR systems.40,42
There are different positive aspects to notice about the system and the course. We implemented a VR system that supports all control requirements recommended by Pedram et al. 36 (a) including “gesture recognition,” (b) providing “motion sensitivity of controls,” (c) meeting “minimum position tracking thresholds,” (d) enabling “kinesthetic manipulation of virtual objects of interest,” (e) providing “efficient movement controls,” (f) providing “control element granularity commensurate with the virtual layout needed.” Moreover, it provides “effective feedback to the user”, 36 both during the simulation (when the patient reacts to the user's actions) and at the end, through a description of the steps and their correctness. Participants in Hood et al. 41 appreciated feedback on timing and decision-making and asked for more specific feedback, such as more information on mistakes. In our study, further feedback was provided by the instructor, a senior cardiologist complementing VR simulation.
As recommended by Pedram et al., 36 visual and auditory cues (e.g., monitor's display contents and sounds) are also provided, whereas haptic cues are currently missing. As for the course, training was performed in small groups (from 6 to 13 participants), and this is described as a facilitator aspect. 40 Moreover, in contrast to another study, where the roles of distinct health workers were not differentiated, resulting in the disappointment of participants, 41 nurses and doctors played their own roles in our system and their collaboration was accurately reproduced, as also reported by some participants. This partnership is essential in the STEMI patient rescue, because the emergency nurse on the field and the doctor in the hospital need to work together to save the patient's life.
Costs are traditionally mentioned among the limitations of VR systems,20,25 of which users are also aware. 40 However, we specifically implemented our system to run on the low-cost Meta Quest 2 VR headset. 31 Moreover, cost-effectiveness may improve if economic costs are analyzed in the long-term and counterbalanced by potential risks and medical errors that could be avoided, thanks to a training conducted in a safe environment. 29
Conclusions
This is the first proposal and study of a VR system to train nurses and doctors in the prehospital management of STEMI patients. The system was embedded in a CME course, making it a blended learning course. We performed a thematic analysis of the answers of course participants who volunteered to be interviewed. This possibly led to a self-selection of those more interested and satisfied and to a consequent overestimation of the blended learning course and VR system. An additional limitation was the small sample size, although representative of the highly specialized health care personnel who deal with prehospital STEMI emergencies. In addition, the interviews did not take place immediately after the course and this allowed participants to reflect on the course, but it could also have caused memory fading and detail loss.
The analysis showed that all participants perceived the VR system and the blended learning course as a positive experience and provided interesting feedback on positive aspects and possible areas of improvement.
Following the advice, we worked on additional scenarios to increase variety. Moreover, we plan to improve the VR system as an evaluation tool and use it to compare the performance of participants of the course with the performance of nurses and doctors who had not yet attended the course, to quantitatively measure the effectiveness of the proposed form of VR-based medical education.
As the main implication for practice, this study highlighted that a VR system integrated in a blended learning course with a strong collaborative approach is much appreciated by all participants and could be inspiring when designing novel medical education programs for nurses and doctors. Of interest, the training course also received a positive reaction at the regional level and was included in the current Training Plan of the Friuli Venezia Giulia Region, thus allowing nurses and doctors to receive a consistent education, smoothing possible geographical differences.
Footnotes
Acknowledgments
The authors gratefully thank nurses and doctors who enthusiastically volunteered to share their perceptions and opinions about the VR system and the entire training course.
Authors' Contributions
F.A.: Writing—original draft (equal); writing—review and editing (supporting); visualization (lead). D.L.: Writing—original draft (equal); formal analysis; investigation (lead); methodology (equal); project administration (lead); writing—review and editing (supporting). B.F.: Writing—original draft (equal); methodology (equal); review and editing (supporting). Z.N.: Investigation (supporting); software. L.S.: Investigation (supporting). V.F.: Funding. C.L.: Conceptualization (equal); writing—review and editing (lead). D.C.A.: Conceptualization (equal); project administration (supporting); resources.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Italian Ministry of Health (NET-2016-02364191) and by the Friuli Venezia Giulia Region, in the framework of the EASY-NET research program. Part of F.A.'s work was supported by a PhD grant from the Italian Ministry of University and Research (PNRR M4C1 Inv. 4.1 D.M. 351/2022).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.