
Abstract
This international multicenter randomized controlled trial aimed to compare the effectiveness of virtual reality (VR) distraction with an identical non-VR game in reducing needle-related pain and anxiety in children undergoing venous blood draw. The study involved 304 children aged 5–9 years undergoing a blood draw procedure, randomly allocated to one of three groups: VR distraction, non-VR distraction, and control group (usual care). The distraction task was based on the Multiple Object Tracking (MOT) paradigm, and the game was identical in design and gameplay for both VR and non-VR distraction groups. The primary outcome was self-reported pain intensity using the Faces Pain Scale-Revised (FPS-R). Secondary outcomes included child distress, attention/distraction to the blood draw, and parent and medical staff satisfaction with procedure. Analyses were conducted using analysis of variance and multivariable linear regression models. The results showed that VR distraction and non-VR distraction performed similarly, showing large effect sizes compared with standard care. There was no significant difference between the two types of distraction. The study’s findings suggest that VR and non-VR distraction are similarly effective in reducing needle-related pain and anxiety in children undergoing venous blood draw. This is the first well-powered study comparing modern VR distraction with an identical task displayed on a smartphone or monitor screen. The study’s results have important implications for using VR in clinical settings and suggest that investing in expensive VR equipment for acute pain management may not be necessary. The study protocol was pre-registered on Open Science Framework at https://osf.io/frsyc.
Introduction
Venipuncture, more commonly called “blood draw,” is a routine pediatric medical procedure that is often painful and stressful for children, but distraction during such procedures can effectively reduce pain and stress.1–8 Addressing children’s stress and anxiety evoked during medical procedures is vitally important in order to ensure their continued engagement with health care. Various distraction methods have been described such as watching cartoons, blowing balloons, doing mental calculations, playing computer games, and use of virtual reality (VR). However, an optimal method has not yet been identified.
According to the neuromatrix theory of pain, sensory, cognitive, and affective inputs in addition to an individual’s attentional capacity can significantly alter an individual’s perception of pain and an individual’s response to it. 9 VR has the potential to be used for effectively reducing pain in children during blood draws as it offers visual and auditory stimulation simultaneously within a noninvasive, artificial, three-dimensional immersive environment. Several reviews have examined the effect of VR on pediatric procedural pain10–15 but have generally found large heterogeneity of effect sizes and relatively low quality studies, making it difficult to isolate the specific effects of VR as a distractor and to decide if VR is any better than simpler or cheaper solutions. This question is important, considering the ease of access and lower cost of many non-VR distraction methods such as mobile phones.
To date, the majority of studies have compared VR distraction with either standard care (SC) or in uncontrolled studies with traditional distraction methods.16–43 A smaller number of comparison studies were conducted between VR and specific distraction methods, such as distraction cards,44,45 local cold application and vibration,44,46 watching TV or tablet/iPad,47–49 computer games, 50 kaleidoscope, 51 or differing VR environments.52,53
Several of those studies did not show any significant difference between VR and other types of distraction,46,48,50,52,53 and in one study, other types of distraction were more effective than VR. 44 Significant differences favoring VR were observed in several studies although only in a subset of the measured outcome variables.45,47,49,51 However, given the substantial differences in distraction content, it is unclear whether the differences are due to the content or VR technology.
A limited amount of research has directly compared similar games displayed either in VR or non-VR.48,50 In a pilot randomized controlled trial (RCT) 48 during subcutaneous port access with 40 oncology patients (mean age 12 years), a VR group played an interactive game, whereas the control group passively watched a video on iPad showing similar graphics and sound stimuli. The difference between the two groups was not significant. Importantly, the control group differed from the VR group not only in terms of medium but also in degree of interaction (active in VR, passive on iPad).
Gershon et al. 50 published a pilot and feasibility study which examined the use of VR during port access with young cancer patients (aged 7–19). Participants played an educational program displayed in head mounted display or on a computer screen. There were no significant differences between VR (n = 22) and non-VR distraction (n = 15) groups. However, the game was created in 1997, and the authors of the study did not provide any information regarding the VR system that was used.
In the present study, we aimed to address the following objectives: (1) to test if VR-based distraction is more effective than an identical non-VR game in diminishing needle-related pain and anxiety in children undergoing venipuncture, (2) to obtain a precise estimate of the effect size for VR distraction compared with a control group who received SC, and (3) to assess parent and medical staff satisfaction after using VR distraction during the blood draw.
Materials and Methods
Design
This study is an international multicenter randomized controlled trial with three participating centers: University of Wroclaw, Poland—coordinator; University of Galway, Ireland; and University of Malaga, Spain. The study protocol was preregistered on Open Science Framework at https://osf.io/frsyc. Data collection took place in pediatric phlebotomy clinics (Clinical Hospital No.1 in Wroclaw; Children’s Health Ireland at Crumlin in Dublin; Hospital Materno-Infantil del Complejo Hospitalario Regional Universitario de Málaga). Children aged 5–9 years were randomly allocated within their respective hospitals to one of the three groups: VR distraction, non-VR distraction, and control group (usual care). Measures were collected at each site by a trained research assistant.
The sample size requirement of 91 participants per group (n = 273) was estimated from a recent meta-analysis of VR intervention during pediatric needle-related procedures. 11 The authors reported an effect size of d = −0.48, 95% confidence interval [CI −0.67, −0.28]. This was computed from 20 studies, representing 1,366 participants, and comparing VR and control groups. We assumed statistical power of 95% and alpha 5%. Power calculations were performed using G*Power software, and in order to compensate for possible missing data, we recruited an additional 15%, leaving a total target sample of 312. The expected 15% attrition rate was based on the authors’ previous similar research. 53
Participants
Three hundred and eighteen children and their parents were recruited, but 14 were excluded for various reasons (see Fig. 1), leaving 304 participants: 105 in VR distraction group, 102 in non-VR distraction group, and 97 in control group. There were no differences in the three conditions in age (F = 0.794, p = 0.453) or sex composition (χ2 = 4.653, df = 2, p = 0.098)—see Table 1 for sample characteristics and Figure 1 for participant flow through the study based on CONSORT.
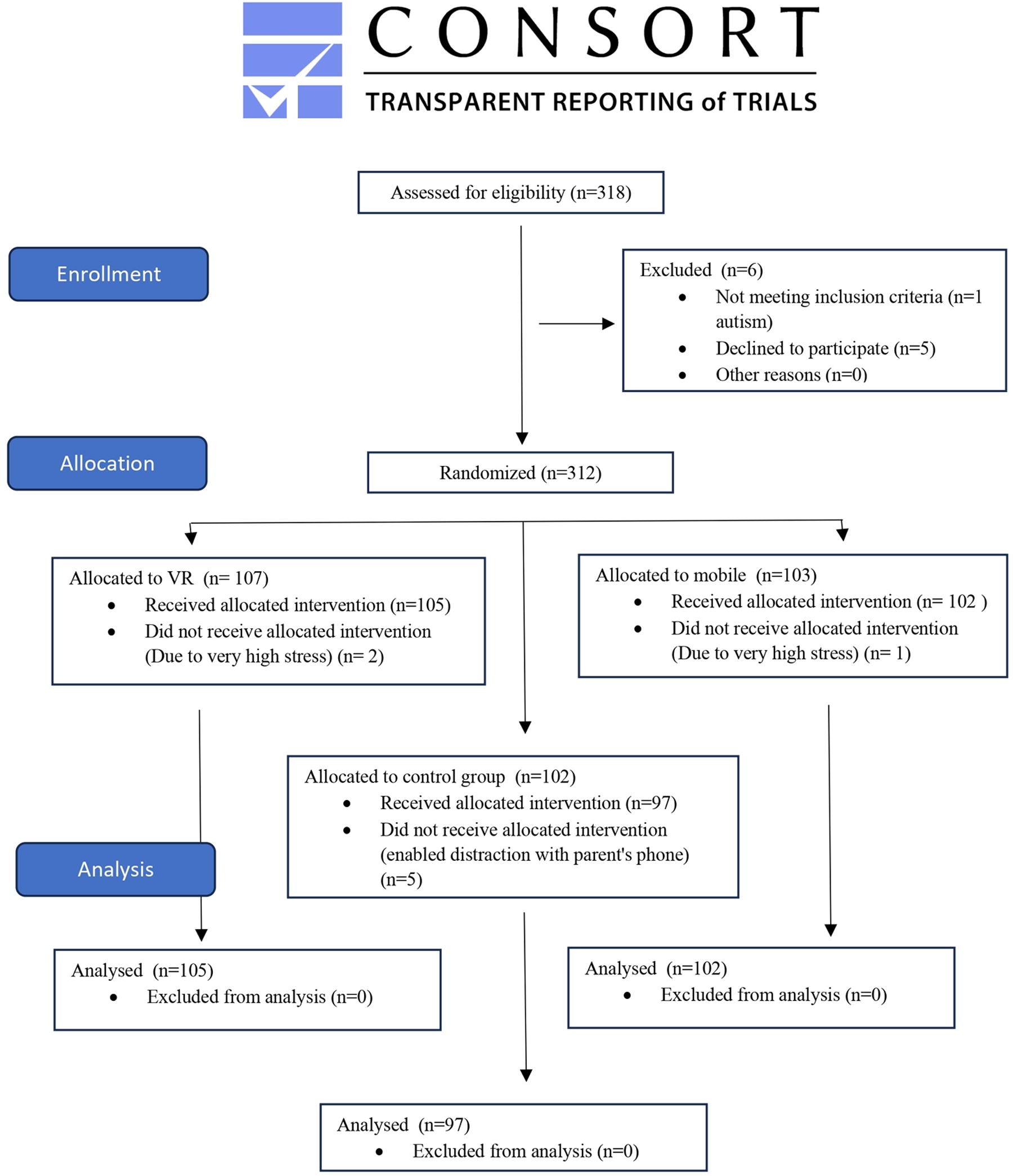
CONSORT diagram of the trial flow.
Sample Descriptive Statistics
VR, virtual reality.
Exclusion criteria were as follows: preexisting medical conditions that preclude VR use or mobile screen use, epileptic seizures, vision problems, hand/finger mobility issues (the non-VR distraction game is played with a hand/finger), conditions that prevent the ability to give answers on outcome measures, and inability to obtain consent from a caregiver and assent from a child.
Conditions
VR distraction
Participants randomized to the VR distraction played Magic Spheres game using Samsung Gear VR system with a Galaxy S8 phone. The game was created by the authors of this study (University of Wroclaw) and consisted of memorizing and later pointing to several elements that earlier were briefly flashing on the screen. For each level of the game, the flying objects were blinking for 15 seconds and then moving for an additional 16 seconds. Each level of the game lasted between 40 and 50 seconds. The duration of the task was dependent on the length of blood draw procedure and number of completed game levels. The game logic was based on the Multiple Object Tracking (MOT) paradigm and was chosen because it demands continuous and uninterrupted attention over time, as well as simultaneous attention to multiple objects. MOT is an inherently active and dynamic attentional task paradigm that can be directly manipulated by the number of objects to be tracked. 54 It has been used in many studies of visual cognition such as working memory,55,56 task switching, 57 and dual-task interference55,58 and in varied populations, including young children. 59 A short video of the game can be found here: https://youtu.be/q3kA7lMnAGQ.
Non-VR distraction
Participants played a two-dimensional version of the Magic Spheres game on a mobile phone screen. The game was identical in design and gameplay logic as the VR version; the only difference was the method of presentation and the interface.
Control
Children in the control group underwent blood draw without any prescribed means of distracting their attention away from the procedure. However, for ethical reasons, neither parents nor clinicians were instructed to refrain from using distraction techniques. If any distraction methods were used, the method of distraction was recorded. Children who spontaneously used their phones or tablets for distraction were excluded from the analysis.
Outcome variables
Self-reported pain intensity—measured with the Faces Pain Scale-Revised (FPS-R). The FPS-R has previously been shown to be appropriate for measuring acute pain in children from age four onward, with good validity and a close correlation to the linear interval numeric rating scale (NRS). 60 It is also widely used in similar studies,16,43 thus allowing more direct comparisons of effect sizes. FPS-R consists of a series of faces ranging from smiling to crying, allowing individuals to indicate their pain level by selecting the face that best represents their experience.
Self-reported pain intensity—measured with a numeric rating scale (NRS). NRS was used in addition to FPS-R as it is considered to be less influenced by factors other than pain intensity. 61 NRS involves asking individuals to rate their pain on a scale from 0 to 10, with 0 indicating no pain and 10 indicating the worst possible pain.
Self-rated distractedness—level of attending to the blood draw, assessed by the child on a 0–10 Likert scale where 0 was “not at all” and 10 was “very much.”
Child anxiety/stress level—assessed by a parent prior to procedure on a 0–10 scale, where 0 was “not distressed” and 10 was “very distressed.”
Child anxiety/stress level—assessed by the nurse/phlebotomist after procedure on a 0–10 scale, where 0 was “not distressed” and 10 was “very distressed.”
Self-reported medical staff and parent satisfaction—assessed after the procedure on a 0–10 scale, where 0 was “not satisfied” and 10 was “very, very satisfied.”
Procedure Behavior Checklist (PBCL)—parent/caregiver ratings of pain/anxiety related behaviors of the child. 62 The scale assesses eight behaviors scored on the basis of occurrence and observed intensity. The scale has previously been used to assess children undergoing venipuncture and has good reliability (Cronbach’s α = 0.85) and test–retest stability (0.8, 2–3 weeks apart). 63
Ethics
The study was approved by the Ethics Committee at the Institute of Psychology, University of Wroclaw, and Bioethics Committee at Medical University, Wroclaw, and in each participating center. The research conforms to “Declaration of Helsinki” requirements, and informed consent was obtained from parents (written) and children (verbal).
Procedure
Parents and children were approached and invited to participate. A general description of the study was given at this initial stage, and detailed instructions were provided only after revealing group allocation. Each center performed a block randomization (using computerized number generator www.randomizer.org). Allocations for each participant were concealed in separate, opaque envelopes; this was done in advance by a person who was not involved in data collection. After initial recruitment, the allocation for a given participant was revealed. However, clinicians were not blinded to the participant allocation, as it is not possible to conceal the type of distraction used during the blood draw procedure.
After group allocation and providing instructions specific to the relevant group, informed consent was given by the parent/caregiver and verbal assent by the child. Questionnaires and their order of administration were identical for all groups. Participants in the VR distraction and non-VR distraction groups practiced a tutorial game before the procedure and then played the game during the blood draw.
Before the blood draw, parents completed a questionnaire about (1) age and sex of child, (2) how frequently the child undergoes blood draws, and (3) degree of distress observed in the child at that moment, using a Likert scale. Then, parents received the PBCL and were instructed on how to fill it in so as to gather information about child behavior during the blood draw. After the participants were seated for the blood draw, they received either VR equipment or a mobile phone and began to play. Participants in the control group were not provided any equipment or given any particular instructions in relation to distraction. Then, the blood draw itself was initiated by the nurse/phlebotomist. During that time, parents filled in the behavior checklist. Immediately after the blood draw procedure, a pain intensity measure was obtained from the child, and all other measures were obtained from parents and nurses/phlebotomists. The postvenipuncture outcomes were collected in the following order: (1) Child: FPS-R immediately after removing the VR goggles, or stopping the mobile game; (2) Child: NRS; (3) Child: attention/distraction to the blood draw; (4) Parent: satisfaction with procedure; (5) Nurse/Phlebotomist: observed stress, medical staff satisfaction.
Statistical Analysis
The preregistered plan for the analysis included a one-way analysis of covariance with FPS-R pain score as the dependent variable and group (VR distraction, non-VR distraction, and control) as the independent variable. Geographical locations (centers) were planned to be coded as dummy variables and included as covariates.
An exploratory analysis was planned with multivariable linear regression models, using predictors of age, sex, self-rated distractedness, prior needle exposure, and group (VR/non-VR/control).
However, because of large differences in sample sizes between countries and heterogeneity of variance, we decided to include country as a variable in the regression model and conducted the confirmatory analysis with Welch analysis of variance (ANOVA). For descriptive statistics, see Table 2.
Descriptive Statistics of Variables (Mean ± Standard Deviation)
VR, virtual reality.
Data were analyzed in R Statistical Software (v4.2.1; R Core Team 2022) and JASP (JASP Team, 2022).
Results
Groups did not have equal variances (Hartley’s Fmax = 3.16, which is above the critical value)—the control group had larger variance than the VR and non-VR distraction groups; therefore, Welch ANOVA was used for homogeneity correction. There was a significant effect of experimental group on pain FPS-R scores, F (2,187) = 20.27, p < 0.001, η2 = 0.151. Bootstrapped post hoc comparisons (from 1,000 replicates) showed that pain scores were significantly different between VR and the control group and between non-VR distraction and the control group. There was no statistically significant difference between VR and non-VR distraction groups on pain scores (see Table 3).
Bootstrapped Post Hoc Comparisons Based on Group (FPS-R)
Bootstrapping based on 1,000 successful replicates. Mean difference estimate is based on the median of the bootstrap distribution. p-Value and confidence intervals adjusted for comparing a family of three estimates (confidence intervals corrected using the Tukey method).
BCa, bias corrected accelerated; CI, confidence interval; SE, standard error; FPS-R, Faces Pain Scale-Revised; VR, virtual reality.
As the difference between VR and non-VR distraction group was not significant, a Bayesian independent samples t test 64 performed in JASP was used to test the null hypothesis that there is no difference in the effect of VR and mobile phone distraction. Between-group difference was assigned a Cauchy prior distribution (scale = 0.707). The resulting Bayes factor of BF01 = 4.33 can be interpreted as moderate evidence favoring the null hypothesis, meaning that the data are about 4.33 times more likely under null hypothesis than under the alternative hypothesis. The error percentage was 0.052, which shows good stability of the used numerical algorithm.
FPS-R results were highly correlated with NRS scores (Pearson’s r = 0.699, p < 0.001). Between-group differences were similar to those obtained with FPS-R, both for ANOVA and post hoc tests. This supports the interpretation that main results obtained in this study were not affected by the choice of pain measurement scale.
An exploratory analysis was conducted with a multivariable linear regression model, using predictors of group (VR/non-VR/control), country (Spain/Ireland/Poland), self-rated distractedness, age, sex, and prior needle exposure, and FPS-R scores as the criterion variable. Those variables were preregistered and chosen based on their possible influence on the dependent variable. Age and sex might influence how much a child would engage with the game. Similarly, prior needle exposure and self-rated distractedness may influence the effectiveness of distraction. Most other variables can be considered outcome variables and not predictors (i.e., stress level assessed by medical staff or PBCL). Because of heteroscedasticity of residuals, we used weighted least squares regression. Predictors were added hierarchically, and subsequent models were compared using the likelihood ratio test.
Model 3 with group, country, and self-rated distractedness outperformed Model 1 (with only group as predictor) and Model 2 (group and country). Adding the interaction between group and country or predictors of age, sex, and prior needle exposure did not further improve the model fit, and those predictors were not statistically significant. Results for Model 3 are presented in Table 4 (control group and Spain were used as reference variables). FPS-R scores were lower for participants in VR and non-VR groups, higher for Polish and Irish participants, and higher for those who reported attention to the blood draw procedure. Experimental groups did not differ regarding age. However, there was a significant difference in age between countries: Welch ANOVA F (2,57) = 5.16, p < 0.01.
Linear Regression Results (FPS-R) with Group, Country, and Self-Rated Distractedness as Predictors
Residual standard error: 1.508 on 296 degrees of freedom.
Multiple R-squared: 0.2408, Adjusted R-squared: 0.228.
F-statistic: 18.78 on 5 and 296 DF, p < 0.00000001.
FPS-R, Faces Pain Scale-Revised; SE, standard error; VR, virtual reality.
A one-way Welch ANOVA was performed to compare the effect of group on parent satisfaction scores. There was a small but significant effect of group, F (2,188) = 3.28, p < 0.05, η2 = 0.018, but after correcting for multiple comparisons, none of the post hoc tests were significant.
A one-way Welch ANOVA was performed to compare the effect of group on self-reported medical staff satisfaction. There was a significant effect of group, F (2,185) = 12.65, p < 0.001, η2 = 0.116. Bootstrapped post hoc comparisons (from 1,000 replicates) showed that medical staff satisfaction was significantly lower in VR group compared with the control group and in non-VR group compared with control group. There was no difference between VR and non-VR groups (Table 5).
Rating of Medical Staff Satisfaction Between Groups
Bootstrapping based on 1,000 successful replicates. Mean difference estimate is based on the median of the bootstrap distribution. p-Value and confidence intervals adjusted for comparing a family of three estimates (confidence intervals corrected using the Tukey method).
BCa, bias corrected accelerated; CI, confidence interval; SE, standard error; VR, virtual reality.
A similar pattern of results was obtained on the Behavior Checklist filled out by the parents. A one-way Welch ANOVA was performed to compare the effect of group on Behavior Checklist scores. There was a significant effect of group, F (2,197) = 38.185, p < 0.001, η2 = 0.224; post hoc comparisons showed that PBCL scores were significantly different and lower in the VR and non-VR groups compared with the control group but no difference between VR and non-VR groups (Table 6).
Parent Rating of Child Distress (Behavior Checklist) Between Groups
Bootstrapping based on 1,000 successful replicates. Mean difference estimate is based on the median of the bootstrap distribution. p-Value and confidence intervals adjusted for comparing a family of three estimates (confidence intervals corrected using the Tukey method).
BCa, bias corrected accelerated; CI, confidence interval; SE, standard error; VR, virtual reality.
Discussion
To the best of our knowledge, this is the first well-powered study comparing modern VR distraction with an identical task displayed on a mobile phone. Both modes of distraction performed similarly, showing large effect sizes when compared with SC. We therefore concluded that VR was no more effective as a distractor than a mobile phone game, where there was identical content of the game. This is consistent with two previously published studies comparing VR and Non-VR distraction using similar tasks. In Hundert’s study, 48 the iPad group was passively watching a video, and Gershon et al. 50 conducted a study using VR equipment that differs a lot from modern standards. In both of those studies, there were no significant differences between the non-VR and VR distraction groups. Self-reported level of distractedness was also a significant predictor of pain intensity, whereas age, sex, and prior needle exposure were not. This suggests that attention distraction was behind the observed analgesic effects of VR and mobile phone games.
Our results may help to determine expected effect sizes of VR and mobile phone distraction; in our study, the treatment effect size was d = 0.95 and d = 0.84, for VR and phone, respectively. This means that 83% of participants in the control group reported higher pain than the VR group. These findings are consistent with those obtained in Turkish participants,8,10,11 but we found a larger effect than was obtained by Caruso et al., 16 although we used an identical or very similar VR headset as the aforementioned studies. In addition, pain was measured on an identical (FPS-R) or comparable Wong–Baker Faces Pain Scale.
VR technology has unique features that distinguish it from other forms of distraction. One such feature is the ability to induce spatial presence, creating a subjective “sense of being there” in the virtual environment. Related to this is the ability to cut off external visual stimuli from the real world, which may lead to greater engagement and immersion. VR can also engage multiple sensory modalities (including touch and proprioception) and can be used to create an illusion of embodiment, providing the user with the experience of having a virtual body. All those aspects open the possibility of creating more effective VR solutions for pain treatment, and possibly using a high end multisensory VR system would show a different pattern of results compared with those obtained in our study.
Data in our study come from three separate locations, although the majority of participants were Spanish. An exploratory regression analysis showed a significant effect of location (while holding group effect constant). Both Irish and Polish participants reported significantly higher pain than Spanish participants. This may signal either cultural differences in pain reporting or differences related to particular hospital and blood draw procedures.
Experimental pain research may be susceptible to sampling bias. 65 However, in our study, the potential for selection bias was low—from 318 children approached, only 5 declined to participate, and a further 8 did not receive allocated intervention, either because of high stress (3 participants) or using other means of distraction in the control group (5 participants).
The game difficulty level was adjusted for age, which may explain lack of significant effect of age. Similar results were obtained by Caruso et al., 16 Althumairi et al., 28 and Wolitzky et al. 41 In those studies, children’s age and sex had no effect on the level of pain. Similarly, in our study, age and sex were not found to be significant predictors of pain. In addition, in Wolitzky et al., 41 the number of previous needle procedures did not affect the level of pain. However, in the study by Chan et al., 43 older children (4–11 years old) experienced less pain, independent of the treatment condition they were assigned to, but this result was obtained only in one of the hospital settings. In Gershon et al., 50 age was a significant factor for VR and non-VR distraction but not for the control group.
If unaddressed, repeated exposure to anxiety-provoking procedures could progress to needle phobia, especially in children, resulting in avoidance of treatment and low compliance. 66 Therefore, effective distraction may have long-term positive effects beyond immediate pain alleviation. The effectiveness of VR distraction in pediatrics is well documented and studied during several medical procedures. 67 It is possible that findings from our study can be generalized to other painful medical interventions.
Limitations
The study had some limitations. Despite our efforts, we were not able to collect equal numbers of participants across countries. It is also known that venipuncture pain scores in children are related to age—both pain intensity and unpleasantness decrease with increasing age. 68 Therefore, any between-country differences in our study could be confounded by age differences, and conclusions regarding cross-site differences are only preliminary. In addition, all three hospitals were in European countries, which limits generalizability beyond Europe. The evidence from research concerning culture and medical procedural pain in children indicates that cultural elements might play a role in how children experience pain during medical procedures, particularly in their pain-related behavior. 69 In future studies addressing cross-cultural differences, it is recommended to use physiological pain indicators in addition to self-report or behavioral measures. We believe that large multicenter trials are needed for understanding the variability of effect sizes obtained from single site research. We collected only one measure from the medical staff in order to simplify the procedure for them. For the same reason we did not measure satisfaction with the procedure from the children. The research assistants on-site were not included as sources of data but it is of interest to note that they considered the VR to be more engaging than the non-VR. VR-based levels of cybersickness were not assessed. However, a very similar game was used in two previous studies without any reported negative symptoms. In addition, the game was designed to diminish any occurrence of simulator sickness. We ensured high frame rate, short VR exposure, and fixed point of view in the virtual space (no vection). 70 Further studies should include more varied samples—both in terms of geographical location and to address the specifics of needle procedure (e.g., vaccination, blood draw, port access).
Footnotes
Acknowledgment
Authors’ Contributions
M.C.: Writing—original draft (lead), formal analysis (lead), conceptualization (equal), writing—reviewing and editing (equal), software (lead), methodology (equal), project administration (equal), visualization (equal), and data curation (equal). E.R.S.-I.: Investigation (equal), project administration (equal), supervision, and writing—reviewing and editing (equal). J.P.: Writing—original draft (equal), conceptualization (equal), investigation (equal), writing—reviewing and editing (equal), software (equal), methodology (equal), project administration (equal), visualization (equal), and data curation (equal). R.E.: Conceptualization (equal), project administration (equal), supervision (equal), and writing—reviewing and editing (equal). H.K.L.: Conceptualization (equal), writing—reviewing and editing (equal), project administration (equal), methodology (supporting), and data curation (supporting). A.E.L.-M.: Conceptualization (equal) and writing—reviewing and editing (equal). B.M.: Investigation (equal) and data curation (supporting). C.R.-M.: Conceptualization (equal), and writing—reviewing editing (equal). C.H.: Investigation (equal) and writing—reviewing and editing (equal). C.O.N.: Investigation (equal) and data curation (supporting). G.S.: Investigation (equal) and writing—reviewing and editing (equal). J.F.R.E.: Resources (equal) and writing—reviewing and editing (equal). L.C.: Investigation (equal) and writing—reviewing and editing (equal). S.M.M.: Investigation (equal), resources, and writing—reviewing and editing (equal). V.M.: Investigation (equal) and data curation (supporting). B.E.M.: Writing—original draft (equal), conceptualization (equal), writing—reviewing and editing (equal), supervision (equal), methodology (supporting), investigation (supporting), and data curation (supporting).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.