
Abstract
Medication reconciliation, the process of documenting a patient’s medication, is currently a time-consuming and labor-intensive process. To make medication reconciliation more efficient, digital assistants (DAs) offer a promising solution. Especially since human-like digital interfaces tend to be appreciated by more vulnerable populations such as patients in a low socioeconomic position (SEP). Despite the potential of DAs for low-SEP populations in particular, these groups are often not involved during the development and design phase of such digital health interventions. This exclusion may explain the lower adoption rates of digital interventions among low-SEP patients and exacerbate the so-called digital divide. We explored the perceptions and needs of patients across the SEP gradient using a participatory design approach. Patients of low-, middle-, and high-SEP backgrounds were asked to interact with a DA developed for this study and were interviewed afterward. A thematic analysis revealed seven themes regarding design, input method, comprehensibility, privacy concerns, benefits, the intention to use, and reassurance. Overall, patients were afraid to make mistakes in their medication entries and therefore valued feedback from the system or caregivers. Low-SEP patients specifically seemed to value more structured input methods when using the DA, while high-SEP patients emphasized the importance of a secure environment for the DA and sought clarity about its functionalities. Our study demonstrates the importance of involving patients across the socioeconomic gradient when developing a digital health tool and offers concrete recommendations for inclusive DA design for researchers and developers.
Introduction
Patients’ medication information stored in their personal electronic health records (PEHRs) is often incomplete, outdated, or does not accurately represent the medications patients are actually taking. 1 Discrepancies between actual medication use and reported medication in the PEHR may lead to medical errors and adverse consequences when patients are treated at a hospital.2,3 To limit these errors, medication reconciliation has become a standard practice of care at admission. 4 Medication reconciliation is a process in which a health care provider and patient interact to obtain and document an accurate list of medications used by the patient, at every point of transition in care. 2 This process, however, can be highly time-consuming and labor-intensive.5,6
To make medication reconciliation more efficient, various (digital) intervention tools have been developed in the past.7,8 For instance, by collecting medical information at a kiosk in the hospital, 9 or by integrating a web-based reconciliation application in PEHRs. 1 Literature reviews have shown that such interventions, if properly designed, are generally received favorably by patients. 7 Most of these interventions, however, use one-way input methods that may hamper engagement. 9 The back-and-forth interactional process between patient and caretaker to check and verify medication use is crucial for patient understanding, engagement, and trust. 10 Therefore, incorporating conversational aspects into the digitalized medication reconciliation process seems warranted. 9
Digital interfaces that simulate human-like interactions have increased in popularity. 10 They have been evaluated as more user-friendly than regular health applications and have been accepted by a wider range of populations, including more vulnerable ones.10,11 Moreover, they result in high satisfaction levels regardless of users’ literacy levels. 12 Digital assistants (DAs) have therefore been suggested as an effective solution to the medication reconciliation process. A DA is a text-based system that is capable of interacting with users using natural language, mimicking human interaction. 13 Similar to other medication reconciliation interventions, DAs have the potential to make medication reconciliation more efficient, give the patient more flexibility in terms of time and space, and result in more up-to-date medication lists. 12 Furthermore, DAs have specific design benefits, such as showing a log of what has been discussed and allowing for asking questions by the patient to enhance understanding and solve confusion. 11
Despite these benefits, most digital (health) interventions, including DAs, struggle with adoption in low socioeconomic position (SEP) patient groups.14,15 SEP describes an individual’s position within society relative to others. 16 People in a low SEP typically have a lower education level, income, and health literacy. 17 Research has shown that low-SEP patients often have more unfavorable and less confident attitudes toward using digital health interventions.14,18 This might be attributed to low-SEP patients often having lower technological skills and health literacy compared with high-SEP patients,11,14 but could also be because, during the design of such digital interventions, the opinions and experiences of marginalized populations are often overlooked and/or not inquired. 12
As such, fundamental knowledge on how digital interventions, such as DAs, are perceived by low-SEP populations is currently lacking. Only a few (digital) intervention studies have considered low-SEP patients’ attitudes from the outset, 14 and, to our knowledge, none has specifically focused on medication reconciliation DAs. To ensure acceptance and adoption of the medication reconciliation DA by the general population, including people with low-SEP who struggle with poor health in general, 19 it is essential to consider the attitudes and perceptions of low-SEP patients from the start. 14
Therefore, this study conducts interviews with patients across the SEP gradient to evaluate the first prototype of a medication reconciliation DA. Our first research question (RQ) concerns exploring the experiences with- and perceptions of the medication reconciliation DA of all patients, regardless of their SEP level (RQ1). Our second RQ relates to exploring whether these experiences and perceptions differ across low- and high socioeconomic backgrounds and identifying specific areas that require additional attention for low-SEP patients in further developing the DA (RQ2). Through this participatory approach, we aim to generate fundamental knowledge on how to design digital health interventions that are inclusive of low-SEP patients and to develop a medication reconciliation DA that meets patients’ needs and preferences regardless of their socioeconomic background.
Method
Design and material
This qualitative study explored how patients with varying SEP levels experienced a prototype of a medication reconciliation DA. To explore their perceptions effectively with a flexible and practical approach, we conducted interviews that were thematically analyzed. 20 Figure 1 shows a screenshot of the DA prototype. We used an existing instant messaging application that offered end-to-end encryption and supported interactions with chatbots (i.e., Telegram) to have the prototyped DA follow a script based on in-person medication reconciliation conversations specifically developed for this study. The prototype had multiple methods of input for patients to answer the DA’s questions, including multiple choice (Figure 2A), open-text fields (Figure 2B), and open-text fields with autosuggestion (Figure 2C). Detailed information about the development of the DA, and details about the overall project can be found in an online Supplementary Appendix SA1.1
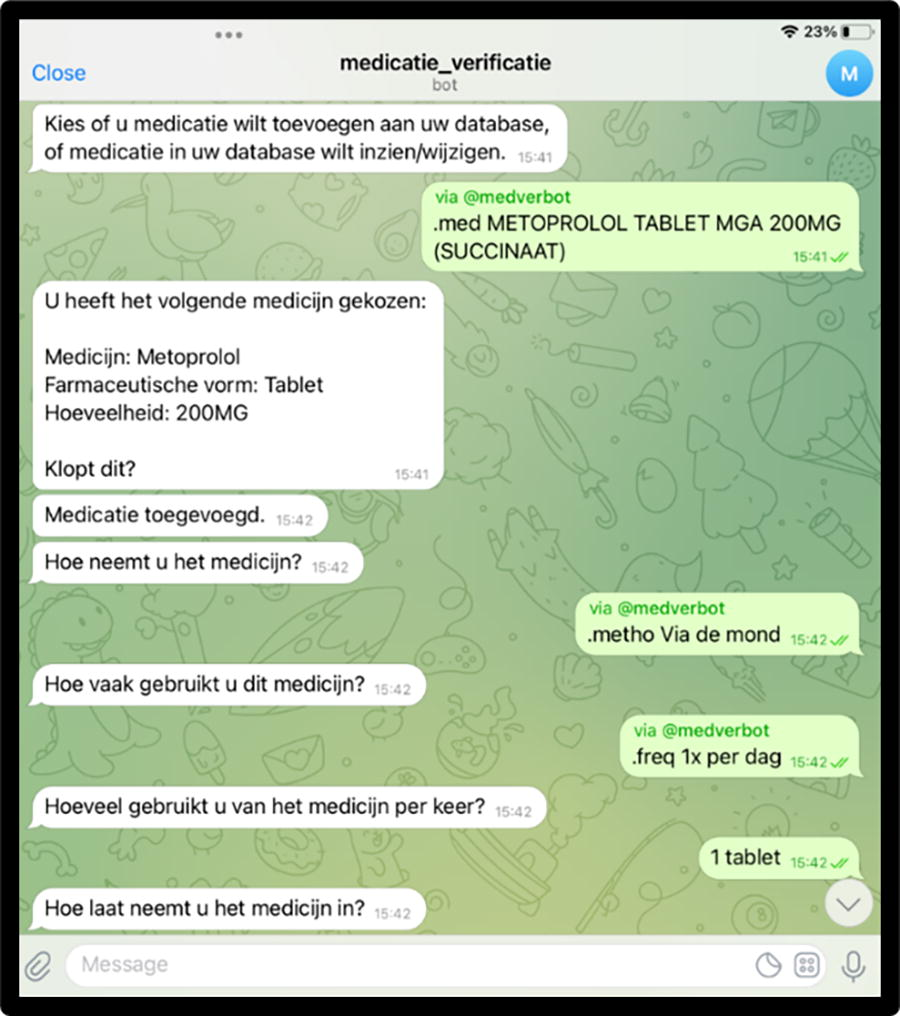
Note. Interaction translated in English: DA: Choose whether you want to add medication to the database or whether you want to see or change the medication in the database. User: (chooses “add medication”) METOPROLOL tablet 200 mg (succinate). DA: User chose the following medication: metoprolol, pharmaceutical form: tablet, amount: 200 mg. Is this correct? User: (chooses “yes”). DA: Medication added. How do you take the medicine? User: (chooses “through the mouth”). DA: How often do you use this medicine? User: (chooses “1 time a day”). DA: How much of the medicine do you use every time? User: 1 tablet. DA, digital assistant.

Note. Screenshot A shows multiple choice and reads the following question asked by the DA: “Which side effects do you experience when using this medication?” Options: Skin rash, feeling of tightness, swollen throat, swollen lips, swollen face, swollen tongue, itching, stuffy nose, and none of these. B shows open-text entry and reads the following question asked by the DA: “At what time do you take the medication?” C shows open-text, including autosuggestion, and reads multiple answer options based on the user typing “26” as a response to the DA asking, “For how long have you been taken the medication?” Autosuggestion options include 26 days, 26 weeks, 26 months, and 26 years.
Semistructured interview questions were developed by a multidisciplinary research team, including academic researchers, DA developers, and pharmacists to gain information about users’ perceptions regarding the design, the functionalities, and the intended use of the DA (Supplementary Appendix SA2). The interview guide was pilot-tested for clarity and completeness in one interview. A waiver was obtained from the Medical Ethics Review Committee Brabant as the study was not within the scope of the Dutch Human Research Act (NW2022-21). Additionally, the study was approved by the Board of Directors of the Elisabeth Tweesteden Hospital (ETZ), the participating hospital (Research manager, study L1525.2022).
Study population
Patients were recruited at the Neurology, Rheumatology, Traumatology, and Vascular Surgery departments of ETZ At ETZ, over 60,000 medication reconciliation conversations are conducted annually. Data were collected face to face between May 2022 and May 2023. Patients were eligible if they were 18 years or older, and (had) used at least one medication (common over-the-counter medications such as pain relievers like acetaminophen included). No predetermined requirements were made regarding patient SEP in approaching potential participants. Patients were excluded from participation if they had insufficient knowledge of the Dutch language, or appeared mentally or physically incapable of participating, which was assessed by the nurses working in the departments. During the data collection process, data from one participant were excluded due to experiencing language barriers during the interview. This resulted in a final sample of 24 patients (Mage = 62.04, standard deviation [SD]age = 15.08, range = 24–85 years).
Based on previous research, 21 patients were allocated a low-, middle-, or high-SEP score based on their education level, postal code-based status score, 22 and income relative to their household and work situation. This yielded seven low-SEP patients, nine middle-SEP patients, and eight high-SEP patients. Table 1 shows an overview of patient characteristics.
Patient Characteristics (n = 24)
To determine SEP, patients were given separate SEP scores for (1) education level, (2) neighborhood, and (3) a combined assessment of income, household, and occupation. If at least two of the three variables were at the same level, that level was assigned as the patient’s SEP. If all three variables differed, a middle-SEP score was assigned. In cases of missing information or significant discrepancies, the education level served as the decisive factor. For more details on SEP assessment see Tenfelde et al. (2023). 21
SEP, socioeconomic position.
Interview and data collection
Patients were approached face to face for participation by a rheumatologist, neurologist, the first or second author, or a student assistant and received verbal information regarding the design of the study. They were told that participation was voluntary, the data obtained by the DA would be processed anonymously, and it would not be used by the researchers or the hospital nor stored in their PEHR. If patients were willing to participate, they received a written information letter and signed a consent form. Prototype testing and interviewing took place in a consultation or patient room, depending on where the patient was located in the hospital. The interviewer (the first or second author or a student assistant) then provided a more detailed introduction and explanation of the DA, both verbally and by showing it on a tablet or smartphone with the DA installed. Consequently, participants were given the choice of using either a tablet or a smartphone to interact with the DA. Using the selected device, they then completed the medication reconciliation process for one or two of their medications. Upon completing their interaction with the DA, patients were interviewed. Interviews were audiorecorded and took between 6 and 25 minutes (M = 12.1; SD = 5.2) After the interview, patients completed a questionnaire containing demographic questions and received a gift card to thank them for participating. Patient SEP was assessed confidentially by the first author afterward, based on the data collected in the questionnaire. Data collection was ceased after we had a well-varied group regarding patient SEP and data saturation was reached.
Analysis
All audiorecordings were transcribed verbatim. Thematic analysis, following Braun and Clarke’s method, 20 was performed to analyze the interviews. An inductive approach to coding was adopted, allowing to extract codes from the data. The first step was to (re)familiarize ourselves with the data by rereading the transcripts and highlighting relevant quotes. To maintain impartiality regarding SEP, this process was conducted without prior knowledge of the participants’ SEP level. Then, the first author coded the highlighted parts of the transcripts using Atlas.TI software, version 23. Codes were subsequently grouped into similar categories, resulting in various main- and subcategories. The categorization of these codes was discussed and refined among all researchers until consensus was reached. Subsequently, the first author identified possible themes in the data based on the categorized codes. Then, the theme descriptions were discussed with all researchers, after which the first author defined and refined each theme. This iterative process led to the identification of seven main themes (RQ1). Each theme was then given theme labels to improve the readability of our results. Next, the coded transcripts were linked to the participants’ SEP level to explore how each theme presented among both low- and high-SEP groups, aiming to uncover the most pronounced SEP-based differences and similarities (RQ2). As a final step, the first author selected quotes fitting each theme and translated these into English.
Results
Table 2 presents an overview of all themes, including theme labels, descriptions, and exemplary quotes, based on all (n = 24) participants (RQ1). Our analysis revealed seven themes that were possible to categorize into two categories: (1) system-related themes that pertain to the features and functionality of the system itself (i.e., design, input method, and comprehensibility) and (2) person-related themes that focus on the user’s perspectives and feelings about using the system (i.e., privacy concerns, benefits, intention to use, and reassurance). Below, we discuss the themes in light of low- versus high-SEP-related similarities and differences (RQ2). Table 3 at the end of the results section provides a summary of the key differences within the themes between low- and high-SEP patients.
Themes Identified in the Data and Exemplary Quotes
DA, digital assistant.
Key Differences Between Low- and High-SEP Patients Across All Themes
These differences highlight the most outstanding SEP distinctions in a concise manner. Findings are based on a qualitative thematic analysis; for more nuance regarding these findings, please see the text.
System-related themes
Design
Both low- and high-SEP patients thought the design of the DA was adequate. Some patients brought up that the font size could be bigger, but most patients, both low- and high-SEP, were rather indifferent when it came to the design, colors, and fonts of the DA: “Sure, it is fine. I have to say that ehm, it [the design] doesn’t matter, it should be functional. So, yeah, if it just looks orderly, it’s good” (P18).
Input method
Although patients generally did not voice a strong preference, low-SEP patients specifically reported disliking fully open-text fields as input method. Low-SEP patients seemed to appreciate autosuggestion because: “often you do not really know how to write it [the medication]” (P01). Regardless of the preferred input method, patients emphasized the need for clarity and consistency throughout the DA. This was valued by both low- and high-SEP patients, with one low-SEP patient mentioning: “The only thing is that, ehm. pressing a ‘send’ button one time and choosing an option in a menu the other time, that creates confusion. […] So, yeah, either one or the other but let it be the same everywhere.” (P03).
Comprehensibility
Both low- and high-SEP patients found messages received from the DA easily readable. As one patient puts it: “yeah, no, it was good, it is definitely no legalese. 2 ” (P04).
Nonetheless, a few low-SEP patients mentioned that more simplistic language would be valued. More general confusion regarding the DA’s actual communicative function was expressed by high-SEP patients: “But, ehm, when I get a new medicine, the system will not say something like ‘you need to pay attention to this side effect and that’ right?—like, it is not to replace the pharmacist?” (P21).
Person-related themes
Privacy concerns
Most patients, both low- and high-SEP, perceived no strong privacy concerns while using the DA. Opinions ranged from “I think it [privacy laws] is so exaggerated, they’re all crazy” (P06) to “In general, I feel safe […], but it [my medications] is not something that I would want to be out in the open” (P18). The majority of higher-SEP patients, however, mentioned that a secure digital environment is imperative to feel safe using the DA: “It depends on how it [the DA] is linked. If it runs via the ETZ app, then it is fine because I need to log into a safe environment” (P18).
Benefits
Patients from all SEPs perceived the benefits of using the DA. Most notably, they appreciated being able to choose their preferred time and place for their medication reconciliation: “[when I got the medication reconciliation call] I was caught off guard […]. I was like okay … and then what were the names of those medications again? I needed a moment because I had to find and look at that [medications] again […]. It is nice to be able to use the DA when the time suits you” (P21). Some patients also mentioned that using the DA probably saves caretakers’ time. One low-SEP patient appreciated that a DA could prevent verbal miscommunication.
Although benefits were seen, understood, and valued, some low- and high-SEP patients mentioned that using a DA is also “simply a lot less convenient than having an in-person conversation” (P23) and that using a system for the medication reconciliation task may feel “impersonal” (P22), which is why in-person medication reconciliation still is preferred by some. No notable SEP differences were observed in this theme.
Intention to use
Regardless of patients’ (mostly positive) experiences with the DA, imagining actually using the DA was hard for some, especially for low-SEP patients. They mentioned that using a system like the DA simply “does not suit them.” As one patient puts it: “yeah, well, I just don’t use those kinds of things. It just doesn’t appeal to me” (P07). In addition, higher-SEP patients mentioned that they were unsure whether patients with lower (digital) literacy levels or older age would use such systems: “Well, I am quite young myself and know how to handle phones and such. But I can imagine that it can be difficult for older people, especially with that tiny little screen” (P17). Patients also expressed practical reasons for not wanting to use the DA, such as not having access to a smartphone, tablet, or computer (P05).
Reassurance
Throughout the interviews, it became clear that both low- and high-SEP patients were concerned about making mistakes in the DA. Some low-SEP patients worried about incorrectly spelling the medication or using brand names instead of medication names: “when you hear the pronunciation of those medications, what they’re officially called, people trip over their tongues. And you guys [the pharmacists] just effortlessly say it” (P04). One low-SEP patient (P07) also noted that when it comes to ‘health stuff,’ they always just immediately pass that on to their children as they have trouble understanding it.
Furthermore, we observed concerns in both low- and high-SEP patients about taking responsibility for their own medication. This was mainly because they thought their data input in the DA would be definite, and they expressed a need for feedback either through the DA or by the pharmacist: “Yes! [I miss feedback], to know that I entered my medication correctly” (P22).
Discussion
This study aimed to explore how an inclusive medication reconciliation DA can be developed by delving into the experiences and preferences of patients from varying socioeconomic backgrounds, something that is often overlooked in the design of digital health interventions. We performed interviews and applied thematic analysis to reveal three themes related to the system of the DA (i.e., design, input method, and comprehensibility) and four themes related to personal factors about using the DA (i.e., privacy concerns, benefits, intention to use, and reassurance).
Our first aim was to map out the general experiences with- and perceptions of a medication reconciliation DA of all patients (RQ1). Our findings showed that patients did not really have strong opinions regarding system elements (e.g., the design) of the DA. However, from a personal perspective, patients expressed their opinions more clearly. Interestingly, patients reported having few privacy concerns with using a medication reconciliation DA. This could indicate that patients genuinely feel safe using a DA for medication conciliation. Alternatively, it might suggest our study sample lacked privacy awareness. It is possible that our participants were less experienced with technology, which is often associated with lower awareness of privacy issues. 23 Clear opinions were also expressed regarding the need for reassurance or support among all patients, as they voiced the need for feedback from the system or help from family/friends. If we continue to speculate that our sample might have been less experienced with technology, they may also exhibit low self-efficacy (i.e., an individual’s belief in their ability to successfully execute a particular task). 24 If patients are unsure about their ability to use digital systems, it is natural for them to seek reassurance.
Looking at low- versus high-SEP patients specifically (RQ2), we observed several system-related preferences. Low-SEP patients seemed to prefer structured input methods as opposed to open-text entries. Disliking open-text entries might stem from low-SEP patients often having lower (e-)health literacy skills than higher-SEP patients, 17 which potentially makes them feel less confident about their entries. Structured input methods, such as autosuggestions and drop-down lists, may offer a way to alleviate their lack of confidence. Among high-SEP patients, we uncovered more general confusion regarding the comprehensibility and functionality of the DA. This finding challenges the conventional assumption that lower-SEP patients would have more difficulties understanding and using digital interventions. 15 However, this finding may also reflect low-SEP patients feeling less confident to critique the DA as they might believe they lack the expertise on the subject. 25
Implications, limitations, and future research directions
We demonstrated the potential of a DA as a digital intervention for medication reconciliation for a variety of patients across the socioeconomic gradient. Focal attention points are that the DA’s function should be clearly communicated and that the option for real-life contact remains for patients who need it. Future research is needed to test whether using a DA indeed results in accurate medication reconciliation and satisfied end users.
Furthermore, our findings should be interpreted in light of two important limitations. First, patients in our study evaluated a prototyped DA that was not yet fully functional. Second, participants used the DA in a hospital setting rather than at home, which is the eventual goal for its use. Both factors potentially shaped participants’ experiences and perceptions. Hence, testing more functional versions of DAs in real-life home settings are essential next steps to accurately evaluate their suitability and applicability in clinical care.
With this participatory approach, we were able to identify low-SEP patients’ experiences and needs, allowing for a more inclusive DA design, 14 which may, eventually, increase DA adoption among vulnerable patient populations. 15 This is particularly desirable given the often low intention to use such digital interventions among low-SEP populations, 15 also reflected by the findings of this study. Given that few digital interventions are designed with- and/or catered for marginalized populations, 12 our findings offer a valuable addition to existing literature. Not only do we better understand the needs and wishes of low-SEP patients regarding DAs, but we also showed how to approach inclusive design research. As our findings could be relevant for health intervention researchers, developers, and designers, we translated our findings into concrete recommendations (see Table 4) for designing (medication reconciliation) DAs that cater to the diverse needs of patients from various socioeconomic backgrounds.
Concrete Recommendations for Researchers and DA Designers Aiming to Take SEP into Account
Conclusion
A DA appears to be a viable option for medication reconciliation for patients of diverse socioeconomic backgrounds. Patients generally reported positive experiences with using the DA. To create an inclusive DA design, it is crucial to provide patients with a clear understanding of the DA’s functionalities. The DA can alleviate user concerns by emphasizing that the information entered into the DA is not definite and that pharmacists will always double-check the entered data. For low-SEP patients specifically, more structured input methods can help them feel more confident in their medication entries. Our study demonstrated the value of including patients of various socioeconomic backgrounds and we encourage other researchers and designers to do the same to create inclusive digital tools with the far-reaching goal to help bridge the digital divide.
Footnotes
Acknowledgment
The authors would like to thank the students who helped transcribe the interviews.
Authors’ Contributions
K.T. and A.D. researched literature. K.T. developed interview material and wrote the article. C.L. and J.W. developed the prototype. A.D. and K.T. were involved in prototype testing and interviewing. All authors were involved in reviewing the article. All authors were involved in the conception of the study and reviewing the interview material. All authors edited the article and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.