
Abstract
Virtual reality (VR) has emerged as a nonpharmacological adjuvant to manage acute and chronic pain symptoms. The goal of this survey study was to determine the acceptability of VR among chronic pain participants hailing from distressed and prosperous neighborhoods in the state of Maryland. We hypothesized that pain severity and interference vary in groups experiencing health disparities, potentially influencing VR’s acceptability. From March 11 to March 15, 2020, we surveyed a cohort of clinically phenotyped participants suffering from chronic orofacial pain. Participants were asked to express their willingness to participate in a longitudinal VR study and their expectation of pain relief from using VR. Seventy out of 350 participants with chronic pain completed the survey (response rate: 20%). There was no difference in the likelihood of responding to the survey based on their neighborhood distress. Among survey respondents and nonrespondents, similar proportions of participants were from distressed neighborhoods. Among the respondents, 63 (90%) and 59 (84.3%) were willing to participate and expected to experience pain relief from the VR intervention, respectively. Age, sex, race, neighborhood distress, severity of pain, and prior VR experience did not influence willingness to participate in the VR trial or the expectations of VR-induced improvement. These findings suggest that VR as an adjuvant intervention is potentially accepted by chronic pain participants, irrespective of neighborhood-level social determinants of health.
Introduction
Virtual reality (VR) is emerging as a potential digital therapeutic for managing chronic pain and other symptoms. 1 In terms of efficacy, recent trials have shown that VR can mitigate the experience of chronic pain.2,3 A recent randomized controlled trial with a 21-day VR program in at-home settings demonstrated that benefits in chronic pain-related outcomes started to strengthen only after 2 weeks of VR intervention. 4 Another follow-up trial established posttreatment efficacy in an 8-week home-based therapeutic VR. 5 Very recently, Maddox et al. conducted a randomized sham-controlled effectiveness trial (NCT05263037) to determine whether an 8-week, self-administered in-home, behavioral skills VR program for chronic low back pain (RelieVRxTM) is superior to sham at Day 56 for improving pain intensity and pain interference in a large real-world sample. 6 The VR program was superior to sham for pain intensity and pain interference reductions from pretreatment to Day 56.
In addition, Eccleston et al. reported that a digital therapeutic VR intervention significantly reduced fear of movement, pain interference, and disability compared with sham and standard care, highlighting VR’s potential over other digital interventions. 7 As digital therapeutics, especially VR, have become increasingly integrated into health care post COVID-19 pandemic, it is essential to investigate the effects of social determinants of health on an individual’s acceptability of the same. 8 Those living in distressed areas may have accessibility challenges based on their neighborhood features.9,10 A recent review explored the usability of VR among marginalized participants and found a limited number of studies (n = 5), including older people with limited education and racial or ethnic diversity. 11 Therefore, there is a need to fill this knowledge gap. Based on this, 11 we conducted a survey study to determine the likelihood of acceptability of VR for pain reduction among distinct groups using the multidimensional measure of socioeconomic deprivation, area deprivation index (ADI). 12 We focused on temporomandibular disorders (TMD), typical yet underserved patients with chronic pain. 13 TMD affects approximately 5–12% of the general population, 14 and access to nonpharmacological pain treatments is often limited. We surveyed a convenient cohort of 350 TMD participants, mapped their neighborhoods, and phenotyped their pain severity and interference. We hypothesized that participants from distressed neighborhoods defined by the ADI would experience higher pain intensity and interference and would be less willing to participate in a VR trial with no expectations of pain relief.
Methods and Materials
Study population
Three hundred and fifty participants with confirmed TMD had given permission and written consent to be re-contacted from a previous study on pain and genetics (HP-00068315 “Chronic orofacial pain: Genetics, cognitive-emotional factors, and endogenous modulatory systems”). The local Institutional Review Board at the University of Maryland, Baltimore, and all participants provided written consent to participate in the study. The study was conducted between March 11, 2020, and March 15, 2020, during the lockdown period of the COVID-19 pandemic, in which they were sent a brief description of a hypothetical longitudinal VR study and survey questions (see flowchart, Figure 1 and Supplementary Data S1).

Flowchart.
Study design
We conducted a survey study using quantitative and qualitative data. We recontacted 350 TMD-confirmed participants via email. The diagnosis of TMD was previously confirmed at the Brotman Facial Pain Clinic, School of Dentistry University of Maryland, with an in-person clinical examination by an independently trained examiner according to the Axis I Diagnostic Criteria (DC/TMD). 15 Clinical pain was also assessed with an Axis II evaluation via the Graded Chronic Pain Scale (GCPS). 16 TMD eligibility criteria 17 are reported in Table 1.
Criteria for Inclusion/Exclusion 17
The participants were emailed a link to access a brief description of a VR for pain relief via REDCap (Research Electronic Data Capture), a secure, confidential, Health Insurance Portability and Accountability Act, (HIPAA)-compliant, web-based electronic data capture tool hosted at the University of Maryland School of Nursing.
Respondents were asked two dichotomous questions with yes/no responses, followed by two optional open-ended questions. The first question was, “Would you be willing to participate in a two-week trial with a Virtual Reality experiment to relieve pain?” The second question was, “Do you expect to experience some level of pain improvement from the VR intervention?” The open-ended questions were intended to obtain additional details from the participants about their responses by asking, “Why or why not.”
Area Deprivation Index
Developed by the US Federal Government, ADI consists of 17 census variables such as education, income/employment, housing status, and household characteristics, and it utilizes social characteristics not usually captured in electronic health records. 18 It makes it possible to rank communities in an area of interest according to socioeconomic disadvantage (e.g., at the state or national level). It considers factors such as employment, education, income, and the standard of housing. The national percentile rankings of the ADI range from 1 to 100 for the country. The country’s lowest level of “disadvantage” is represented by a block group with a ranking of 1, and the highest level of “disadvantage” is represented by a block group with a ranking of 100. To ensure generalizability, we used national ADI ranking 19 by extracting participants’ addresses, geocoding them using QGIS 3.16 Hanover, mapping them to the census tracts of the state of Maryland (Figure 2), and assigning the appropriate ADI scores. Distressed neighborhoods were defined as having a National ADI percentile range from 61 to 100. 20

Distribution of survey respondents and nonrespondents in a Maryland map. About 31.14% of participants were from a most disadvantaged or distressed neighborhood in Maryland. Among the participants who responded to the survey, 19.3% were from a distressed neighborhood in Maryland, whereas among those participants who did not respond to the survey, 80.7% were from a distressed neighborhood in Maryland. The participants’ zip codes were geocoded to the census tract information of Maryland from the Area Deprivation Index.
Data analysis
Identification of covariates
We compared the differences in age, sex, and race among the participants from distressed and prosperous neighborhoods to determine which variables to include as covariates. An independent t-test and a chi-square test were performed on continuous variables (age) and categorical variables (sex and race), respectively. Any variables that showed significant differences were controlled for as confounding variables.
Neighborhood distress, chronic pain intensity, and interference
We examined how neighborhood distress could have impacted the levels of chronic pain severity in the TMD cohort. We assessed the normality of chronic pain intensity and interference outcomes. We conducted a univariate analysis of covariance (ANCOVA) and the rank-transformed (Quade’s test) ANCOVA appropriately, 21 with neighborhood distress as the between-subjects factor and race as the covariate. Bonferroni corrections for multiple comparisons were applied.
VR acceptability and predictors
Within the subgroup of participants who responded to the surveys, independent t-tests and chi-square analyses were performed to examine how age, sex, and race could have predicted the willingness to participate in a hypothetical VR trial (willing vs. not willing). Similar analyses were conducted with regard to expectations toward VR effectiveness (yes vs. no). Moreover, logistic regressions were performed with neighborhood distress, race, and GCPS grades as independent variables, and VR acceptability (willing vs. not willing) and expectations toward VR effectiveness (yes vs. no) as the dependent variables. A p value of 0.05 was set as the level of significance. SPSS version 27 was used for all the quantitative analyses above.
Two research team members (N.R.H. and T.B.) also analyzed qualitative data using MAXQDA, a qualitative data analysis tool. Responses were coded and grouped using an inductive content analysis. An inductive approach is recommended when little is known about a phenomenon 22 because it allows the researcher to form concepts from abstraction. 23 Data were grouped to answer the study question and to find similarities without preconceived ideas about the findings.
Results
Neighborhood distress, chronic pain intensity, and interference
Among the 350 TMD patients contacted to complete the survey, 109 TMD patients (31.14%) hailed from distressed neighborhoods within the State of Maryland. Participants from distressed and prosperous neighborhoods did not differ in age or sex distribution. However, the majority of non-White TMD participants hailed from a distressed neighborhood (n = 73, 66.9%), which was significantly higher than the White participants (n = 36, 33.1%, χ2 = 20.79, p < 0.001).
The participants who responded to the survey suffered from mild to severe chronic pain intensity (mean = 47.6, SD = 24.3) and interference (mean = 27.14, SD = 29.1), and 28.4% were identified as having high-impact pain. 14
After controlling for self-reported race, we observed a marginally significant main effect of neighborhood distress on chronic pain intensity (F1,347 = 3.34, p = 0.068) (Figure 3A) and interference (ANCOVA F1,347 = 3.21, p = 0.074; Quade’s rank test ANCOVA F1,347 = 4.62, p = 0.068) (Figure 3B). Those living in a distressed neighborhood tended to experience greater levels of chronic pain intensity (mean = 50.94, SD = 23.40) and interference (mean = 31.89, SD = 27.27) compared with those who were living in a prosperous neighborhood (chronic pain intensity: mean = 44.88, SD = 21.80; interference: mean = 23.91, SD = 27.07). The duration of pain did not differ among these participants (F1,343 = 0.44, p = 0.508).

VR acceptability and potential predictors
Seventy of the 350 contacted participants completed the survey (20%) over 5 days (see flowchart, Figure 1). The survey respondents and nonrespondents exhibited similar mean ages, with an odds ratio of 1.01 (95% confidence interval: 0.99, 1.03). Demographic factors such as sex, race, annual household income, education level, and neighborhood distress were of comparable proportions between the surveyed groups, as indicated by odds ratios closer to 1 (Table 2). Chronic pain intensity, interference, duration, and severity also displayed similar patterns. Hence, there are no substantial differences between the surveyed groups. In this cohort of TMD participants, living in a distressed neighborhood did not affect the likelihood of responding to the survey (χ2 = 0.053, p = 0.81). A Maryland map with the distribution of respondents and nonrespondents is shown in Figure 2.
Sociodemographic and Clinical Characteristics
Nearly 90% (63 out of 70) of the respondents indicated they would be willing to participate in the hypothetical VR experiment (Figure 4A). Of the participants willing to participate, they wrote that they were “interested” (n = 18, 28.6%), “curious (n = 3, 4.8%), or “willing to try anything to relieve [their] pain” (n = 9, 14.3%). Two respondents (3.2%) expressed that it would be a “relatively risk-free option to try,” and three respondents (4.8%) believed that it was another alternative to pain medications. Another three respondents wanted to help with research. Participants who were unwilling to participate wrote that the intervention needed to “fit [their] schedule.” Participants described a “lack of time,” “working full-time,” and “time commitment and length of travel” as barriers to participating. One participant provided details about having to work and offered a suggestion: “[the intervention is] time intensive. [I am] unable to take that much time away from my work. If it was one or two days each week over that 2-week period, maybe.”
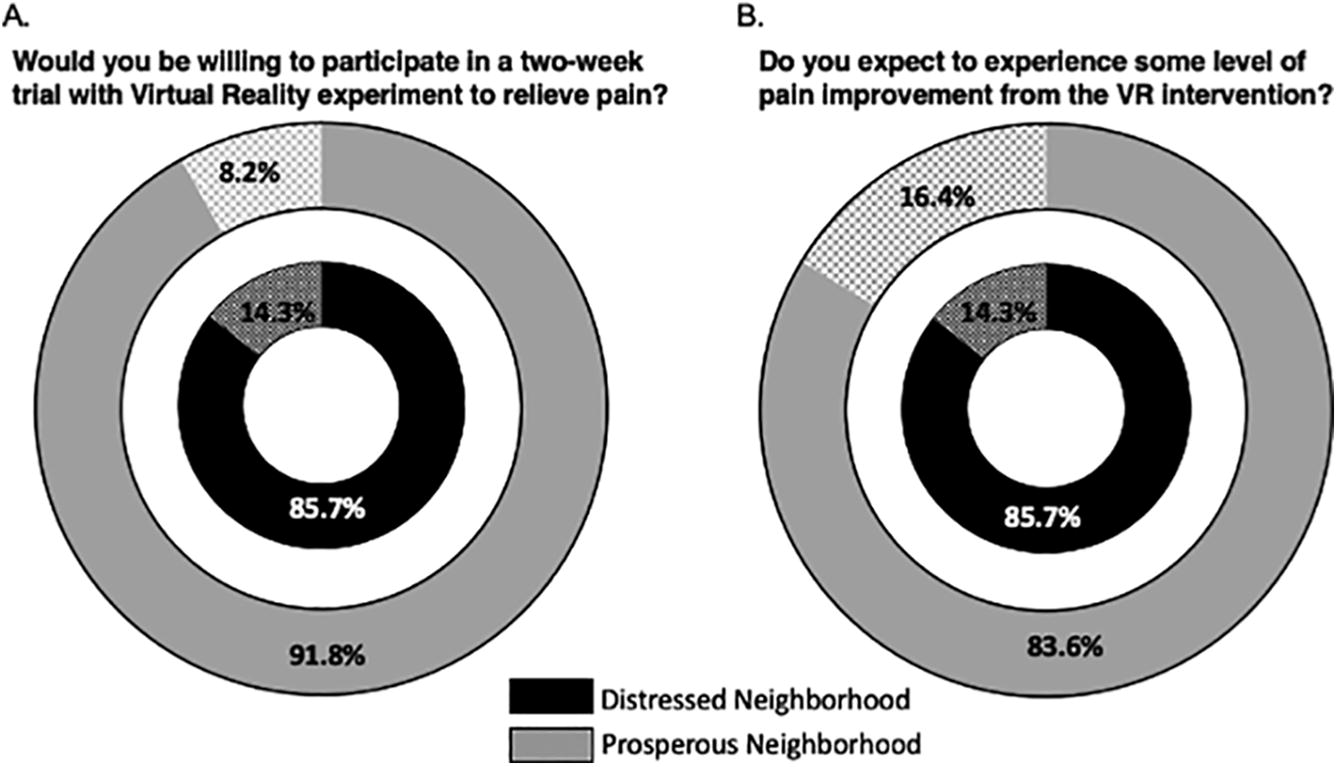
When asked if they expected to experience pain improvement from the VR intervention, 84% indicated “yes” (Figure 4B). A few participants had tried VR in the past and believed that it had some effect. In addition, we found that prior VR exposure did not influence VR’s acceptability (Fisher’s exact p = 0.18). Participants wrote that it “could be [helpful],” “you never know,” and “why not try it?”. Most subgroups that expected pain relief (n = 19, 27%) predicted that a VR intervention would be a distraction. One participant wrote that “…even distraction from pain would be a benefit.” Another wrote that “I trick my brain all the time with different exercises,” and “it’ll give me an opportunity to focus on something else.” One respondent proclaimed the treatment as a “brief psychological relief that is minor and transient.” Some participants (n = 5, 7.1%) believed that there was a correlation between meditation and other integrative medicine modalities. Some wrote that VR would create a “calming reaction” or “evoke a relaxation response.” There were 11 participants (16%) who did not expect to benefit from the hypothetical VR clinical trial. Two respondents did not have experience with VR. One was “skeptical of its effectiveness.” Five participants (7.1%) previously experienced VR and had no success. Other reasons ranged from “not having an opinion on this” to “making my visual challenges worse.”
Sex (Fisher’s exact p = 0.137) and race (Fisher’s exact p = 1.000) did not influence the willingness to participate in the hypothetical VR clinical trial. Older TMD participants (mean age = 42.92, SD = 13.66) expressed a higher willingness to participate than their younger counterparts (mean age = 33.57, SD = 9.05, independent t = −2.44, p = 0.036). Moreover, controlling for race and chronic pain severity assessed as GCPS grades, socioeconomic profiles (OR = 0.47, p = 0.370) did not influence the willingness to participate in a VR trial, suggesting that VR acceptability was independent of neighborhood distress.
Age (independent t = −0.94, p = 0.363), sex (Fisher’s exact p = 0.681), and race (χ2 = 1.43, p = 0.233) did not influence VR effectiveness expectations. Neighborhood distress (OR = 1.69, p = 0.536) was not significantly associated with the expectations of VR-induced pain improvement after controlling for race and GCPS pain grades.
Discussion
This study explored the intersection between the acceptability of VR as an adjuvant digital therapeutic intervention for treating chronic pain and social determinants of health. When presented with a hypothetical VR-based trial, 90% of the respondents showed interest in participating in the study, and 84% expected some pain relief from the VR intervention. Clinical pain severity and sociodemographic factors such as age, sex, and race did not impact the survey response and willingness to participate in this hypothetical VR trial, suggesting that VR-based therapeutics could be employed among participants suffering from chronic pain from various backgrounds.
Progress in the use of VR has flourished within the past few years and provides a possible solution. Studies have demonstrated that VR is effective in significantly reducing pain in acute pain situations.24–26 In a systematic review, Honzel et al. 27 found that 288 VR articles and 58 database articles had been published supporting the use of VR as an adjuvant for pharmaceutical treatments.
Various studies have shown the effectiveness of VR for acute pain, but there is a lack of literature regarding the use of VR to treat chronic pain. 27 A recent systematic review of nine randomized controlled trials explored whether VR significantly improved chronic low back and neck pain. 28 Interestingly, VR-mediated intervention decreased chronic neck pain and disability when compared with control conditions. 28 Previous studies have found that VR reduced fatigue,29–31 stress, anxiety,32–35 and other psychological problems, which can be associated with chronic pain.26,36–42
In this survey study on the acceptability of a hypothetical trial of VR to treat chronic orofacial pain, we surveyed 350 participants with TMD pain. We are among the first to explore how neighborhood distress may affect the likelihood of responding to a survey and participating in a trial using VR as an adjunct intervention for chronic pain. Recruiting from Maryland allowed us to include a representatively diverse population, with 52.9% White and 47.1% non-White participants. Prior studies had investigated the influence of individual characteristics such as education level, health, income, immigration status, biological sex, and race/ethnicity. 11 Unlike previous studies, we used the ADI to provide a new perspective on measuring neighborhood-level resource access. 20 Zip codes contain a wide range of environmental and socioeconomic information, and ADI scores have been used as a proxy for health disparities in cancer screening 43 and opioid use. 44 In this study, the ADI approach served as a comprehensive and innovative way to investigate neighborhood-level social determinants of health.
In terms of qualitative results, we found that among the 70 TMD participants who responded to the survey, 90% were willing to participate and expected the intervention to relieve their pain and serve as a distraction. Most respondents showed positive attitudes, including “… distraction from pain,” “tricking the brain,” and “brief psychological relief.” Our findings are in line with previous surveys demonstrating the acceptability of VR among women with metastatic breast cancer, 45 patients with advanced-stage colorectal cancer, 46 fibromyalgia,47,48 intellectual and learning disabilities,49–51 Parkinson’s disease, and lower extremities injuries.52,53
This study had several limitations and strengths. Given that this survey collected responses in a 5-day window, a longer window would have increased the response rate or changed the participants’ characteristics. We attempted to minimize sampling bias by utilizing an easily accessible online survey through REDCap, which allowed participants to complete the survey at their convenience and in the location of their choice. Our response rate is in line with prior research,45,46,54,55 and we found no significant difference between the demographic characteristics of the prior TMD study participants who did not respond to this survey. This bolsters the validity of our results (e.g., level of accuracy to support our conclusions), but it is also important to mention that our survey was not tested for reliability. Despite no significant difference in sex and age of the participants from distressed versus prosperous neighborhoods, the respondents from prosperous neighborhoods were twofold. This highlights a significant limitation, suggesting a potential imbalance when interpreting the findings. Beyond this, while the online survey format was easily accessible and cost-effective, having live interviewers to record participants’ responses would have allowed for more and better communication. The description of the study itself and the questions asked about it could have been expanded in such a setting. Finally, the fact that we only surveyed participants with TMD limits the study’s generalizability. Although these limitations warrant that our results be replicated in a larger sample incorporating a wider variety of chronic pain diagnoses over a greater period, our findings are still promising and informative because we implemented the ADI approach.
However, the study has important strengths. Using the ADI, we explored differences in participants’ views toward VR and established the acceptability of the hypothetical VR trial based on their level of neighborhood distress. Employing open-ended follow-up questions also gave us further insight into why patients would likely or hesitate to participate. Using an inductive approach for the qualitative analysis of these follow-up questions allowed us to identify common themes that may be useful for future researchers as they design VR-based therapeutic trials and recruit participants with chronic pain.
The implementation and transition of VR into health care settings with participants suffering from chronic pain show promise. Future research should consider the attitudes and acceptance of a longitudinal study using other patient populations and a larger sample to increase the generalizability of the results. Given the large number of participants expecting pain relief from the intervention, researchers should also consider the role of expectations 56 when analyzing the VR findings.
While recent commercialization has made VR technology more accessible with cost-friendly, lightweight, and mobile options, 57 significant variations exist in the quality and capability of VR headsets across different price points. Practitioners and researchers should note that higher quality, often more expensive VR systems are more likely to deliver the therapeutic benefits required. Therefore, balancing accessibility with the need for effective intervention is crucial to maximizing the benefits of VR in pain.
Our results suggest that participants would accept participating in a VR trial to treat their chronic pain condition independently of their level of neighborhood distress. The combination of greater access to VR and participants’ interest clearly justifies further research into this burgeoning field for chronic pain populations.
Data Sharing
Data are available upon publication by contacting the corresponding author with a request.
Footnotes
Author Disclosure Statement
The opinions expressed herein are those of the authors and are not necessarily representative of the official policy or position of the Uniformed Services University of the Health Sciences, Department of Defense, Department of Health Affairs, or United States Air Force. The funding agencies have no roles in the study. The views expressed here are the authors own and do not reflect the position or policy of the Agency for Healthcare Research and Quality, Maryland State and University of Maryland, or any other part of the federal and state government.
Funding Information
This work was funded by MPowering the State Initiatives: Strategic Partnership Grant (LC), the National Center for Complementary and Integrative Health (NCCIH, R01 AT011347, LC), and the National Institute for Dental Craniofacial Research (NIDCR, 1R21DE032532, LC).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.