
Abstract
Interpersonal bias based on weight and race is widespread in the clinical setting; it is crucial to investigate how emerging genomics technologies will interact with and influence such biases in the future. The current study uses a virtual reality (VR) simulation to investigate the influence of apparent patient race and provision of genomic information on medical students’ implicit and explicit bias toward a virtual patient with obesity. Eighty-four third- and fourth-year medical students (64% female, 42% White) were randomized to interact with a simulated virtual patient who appeared as Black versus White, and to receive genomic risk information for the patient versus a control report. We assessed biased behavior during the simulated encounter and self-reported attitudes toward the virtual patient. Medical student participants tended to express more negative attitudes toward the White virtual patient than the Black virtual patient (both of whom had obesity) when genomic information was absent from the encounter. When genomic risk information was provided, this more often mitigated bias for the White virtual patient, whereas negative attitudes and bias against the Black virtual patient either remained consistent or increased. These patterns underscore the complexity of intersectional identities in clinical settings. Provision of genomic risk information was enough of a contextual shift to alter attitudes and behavior. This research leverages VR simulation to provide an early look at how emerging genomic technologies may differentially influence bias and stereotyping in clinical encounters.
Introduction
Bias against minoritized populations is widespread and evident across health care contexts. 1 Health care provider discrimination against individuals of color in the medical system2,3 culminates in racial health disparities.4–10 Similarly, health care providers have shown significant bias against patients with higher weight,11,12 which is associated with a host of negative outcomes, including worse patient physical and mental health.13,14 Research has demonstrated unique, substantial, and complex influences of race and body weight, individually, and in conjunction on clinical processes related to genetics and genomics.15–17 As we move to realize the promise of new genomic medicine technologies, it is crucial to investigate how they will influence and interact with race- and weight-based biases. We use a virtual clinical simulation to evaluate how patients’ apparent race influences bias and stereotyping of a simulated patient with obesity in the context of genomic information provision.
Clinical application of genomic risk information relevant for common complex diseases such as obesity is a goal for genomic medicine.18,19 By modeling this scenario, we can investigate where genomic technologies might exacerbate or attenuate biased behavior and attitudes toward marginalized patient groups. The complexity of genomic risk information introduces additional uncertainty into clinical encounters regarding how and when this information should be applied, and such uncertainty can exacerbate bias and discrimination; for example, prompting decision-making based on medically irrelevant factors. 20 Genomic information could also directly influence perceptions of patients’ health status, such as whether the patients are blameworthy for causing their condition, how likely they are to improve, or what kind of medical interventions might be most appropriate. Discussion of genetic influences on obesity in clinical encounters has previously been associated with reduced weight-based stigma.15,16,21 Consideration of patient self-identified race adds additional nuance because although race is a social construct with limited application to genomic medicine, providers frequently use race when making clinical decisions,17,22,23 which can exacerbate racial health disparities.24–26
There is mounting evidence of an interaction between race and weight stigma. On one hand, possessing multiple disadvantaged identities often creates multiplicative disadvantage. Alternatively, buffering effects can occur that protect an individual from disadvantages associated with a single social category. 27 For Black women with higher weight, there is some evidence of a buffering effect.28,29 For example, Black women with higher weight tend to be penalized less harshly for their weight compared with White women. 30 Health care providers’ specific attitudes toward higher weight among Black women are less clear from existing research given the mixed results.31–33 Some studies suggest that Black patients with obesity report poorer clinical interactions than other groups, 34 while others are more equivocal. 35 There is no experimental research focused on the intersection of race and weight in a clinical context, which may help clarify this picture.
Assessment of bias in clinical encounters brings with it a host of methodological challenges. Chiefly, assessments in a real-world health care environment rarely allow for causal inference. To address this, researchers have leaned on simulation technologies such as virtual reality (VR), in which experiments can be conducted in controlled but psychologically realistic environments and focal patient characteristics can be randomized. 36 In addition, implicit measures of bias in VR are collected continuously and covertly and can indicate subconscious differential treatment through assessment of physical, nonverbal behavior such as gaze direction, interpersonal distance, and speaking duration. 37 These interactions also produce linguistic behaviors (i.e., speech) as participants interact with virtual patients, which can be examined for bias,38,39 such as the extent to which a provider mirrors the patient’s tone, demonstrating a more harmonious social exchange. 40 As such, experimental VR simulation studies can provide strong evidence for causal relationships between patient characteristics and bias.
The current study examines the influence of apparent patient race and provision of genomic information on medical students’ behavior toward patients with higher weight. Medical students are a key population to target to mitigate bias in the health care environment. Participants were randomly assigned to interact with a virtual patient who appeared to be Black or White; in both cases, the medical record indicated the patient was female and met the body mass index (BMI) criteria for obesity. Participants were further randomly assigned either to receive genomic risk information about the patient for five common complex diseases, or to receive only a negative carrier test result with no applicable disease risk information.
We approached this study with three hypotheses. Because the literature on race and weight intersectionality is mixed and largely unexplored in the clinical context, we based hypotheses on general findings of poorer treatment for patients from racially minoritized groups, not accounting for weight status. Hypothesis 1: Medical student participants who encounter the Black virtual patient with obesity will exhibit more negative attitudes, stereotyping, and biased behavior than participants who encounter the White virtual patient with obesity.
Following the literature showing that provision of information about genetic factors in weight tends to reduce weight bias (above), we similarly propose reduced bias with provision of genomic test results. Hypothesis 2: Participants who receive a report with the virtual patient’s genomic risk information for obesity and other common, complex diseases will exhibit fewer negative attitudes, less stereotyping, and less biased behavior than participants who do not receive this information.
As mitigating information tends to reduce negative attitudes toward the in-group or individuals with higher social status more than lower social status, we proposed an interaction hypothesis as well.41,42 Hypothesis 3: Patient race and the presence of genomic information will interact to affect participant attitudes, stereotyping, and behavior such that the risk information will reduce bias against the White patient with obesity more than the Black patient with obesity.
Method
Participants
Participants in the current study include a sample of 84 third- and fourth-year medical students recruited from the metropolitan Washington, DC, area through social media postings, listserv messages, physical postings on campus, and word of mouth. Exclusion criteria included those related to the VR equipment (seizure or vestibular disorder, high propensity for motion sickness, known pregnancy, low vision or hearing), as well as having received information about the study details before participation. The study was approved by the IRB of the National Human Genome Research Institute.
Procedure
Participants consented to the study, and the study procedure was described verbally. Participants reviewed the patient’s medical record, including basic information, records from a previous examination (all normal except for elevated BMI of 33), and results of a direct-to-consumer genetic test that the patient brought to the visit. Depending upon randomized condition, participants received either genetic carrier results only (in which the patient was not a carrier for any condition listed), which functioned as a control group, or they received carrier information plus genomic risk results for five common health conditions. Genomic risk was elevated for obesity, type 2 diabetes, and kidney disease and typical for hypertension and heart disease. Participants then interacted with the virtual patient in a simulated clinical encounter (with the patient appearing Black or White depending upon randomly assigned condition). All other aspects of the virtual patient, including their voice and mannerisms, were identical (see Fig. 1).

Virtual environment from participant perspective with Black virtual patient.
At the beginning of the encounter, the medical student participant was instructed to verbally introduce themselves. The virtual patient conveyed her current medical concerns (i.e., chronic knee pain and recent onset fatigue) to the participant. A physical examination was not possible during this simulation. Participants responded verbally to the patient with any content they felt was appropriate at that time (Fig. 2). Due to the nature of the encounter, virtual patients did not answer questions. Although a lack of question and answer is unusual for a clinical encounter, this allows for an identical experience among all participants. During all phases of the virtual experience, participants’ gaze, body position, verbalizations, and talk time were recorded for analysis. Following the virtual encounter, participants completed a questionnaire. Description of all measures included in analyses can be found in Table 1.

Temporal structure of the virtual clinical visit.
Measures
LIWC, Linguistic Inquiry and Word Count; VR, Virtual Reality.
Means (Standard Deviations) and Analysis of Variance Results (F Value) for All Dependent Measures
p < 0.05.
p < 0.01.
p < 0.001.
Data preparation and analysis
Explicit bias variables were assessed with ANOVA and planned contrasts. During analysis, significant amounts of missing data were noted, and a deeper exploration of missingness patterns based on condition and participants’ reported racial group was conducted including chi -quare analyses to assess possible differences between groups.
Language matching, gaze, and interpersonal distance were assessed both in aggregate and within each segment individually. Segments were separated based on whether the participant was speaking to the virtual patient versus listening to her speak given differential nonverbal behaviors typically associated with each. Summary measures were assessed with ANOVA. Individual segment values for the behavioral measures were entered into a repeated-measures ANOVA. When Mauchly’s test of sphericity was significant, a Greenhouse–Geisser correction was applied. Assessment of minimum distance in each segment controlled for the user’s starting position. Because technical aspects of the VR environment can sometimes render behavioral measures invalid, gaze data were only analyzed for participants who spent at least 10% of the encounter gazing at the patient’s face. This cutoff was determined through visual inspection of discontinuity in the data.
Results
Participant demographics
Study participants (n = 84) were 64% female and 36% male. A total of 42% reported their race as White, 31% Asian, and 20% Black, with the remaining 7% reporting American Indian/Alaska Native or multiracial. A total of 43% reported that they were in their 3rd year of medical school, and 57% were in their 4th year. Participants reported an average age of 26 years (SD = 2.20), and they had an average measured BMI of 23.8 (SD = 4.20).
Self-report patient stereotypes (explicit bias)
Negative obesity-related stereotypes associated with laziness revealed no main effect of race and no interaction. There was a significant main effect of genomic information provision in which laziness stereotypes were higher when the patient was accompanied by genomic information versus control (see Table 2). Analysis of obesity stereotypes related to unpleasantness revealed no main effects and a significant interaction, Figure 3. Within the control group, which did not receive genomic risk information, the White patient was stereotyped significantly more than the Black patient (p = 0.047), whereas stereotyping did not differ when genomic information was presented. Average responses to behavioral likelihood items related to negative patient stereotypes revealed no significant main effects, and a significant interaction. Planned contrasts confirmed a similar trend; in the control condition, the White patient was rated significantly more negatively than the Black patient (p = 0.024), whereas when genomic information was provided, the White patient was rated significantly more positively than the Black patient (p = 0.033).

Graphical representations of significant interactions for self-report variables; error bars denote 95% confidence interval.
Assessment of missingness in the self-report data revealed that for some measures, over half of all participants elected not to respond to one or more items that comprised a given scale. The rate of missingness, while high, was not significantly related to the patient’s apparent race, provision of genomic information, or the participant’s reported race. See Supplementary Table S1.
Language style matching (implicit bias)
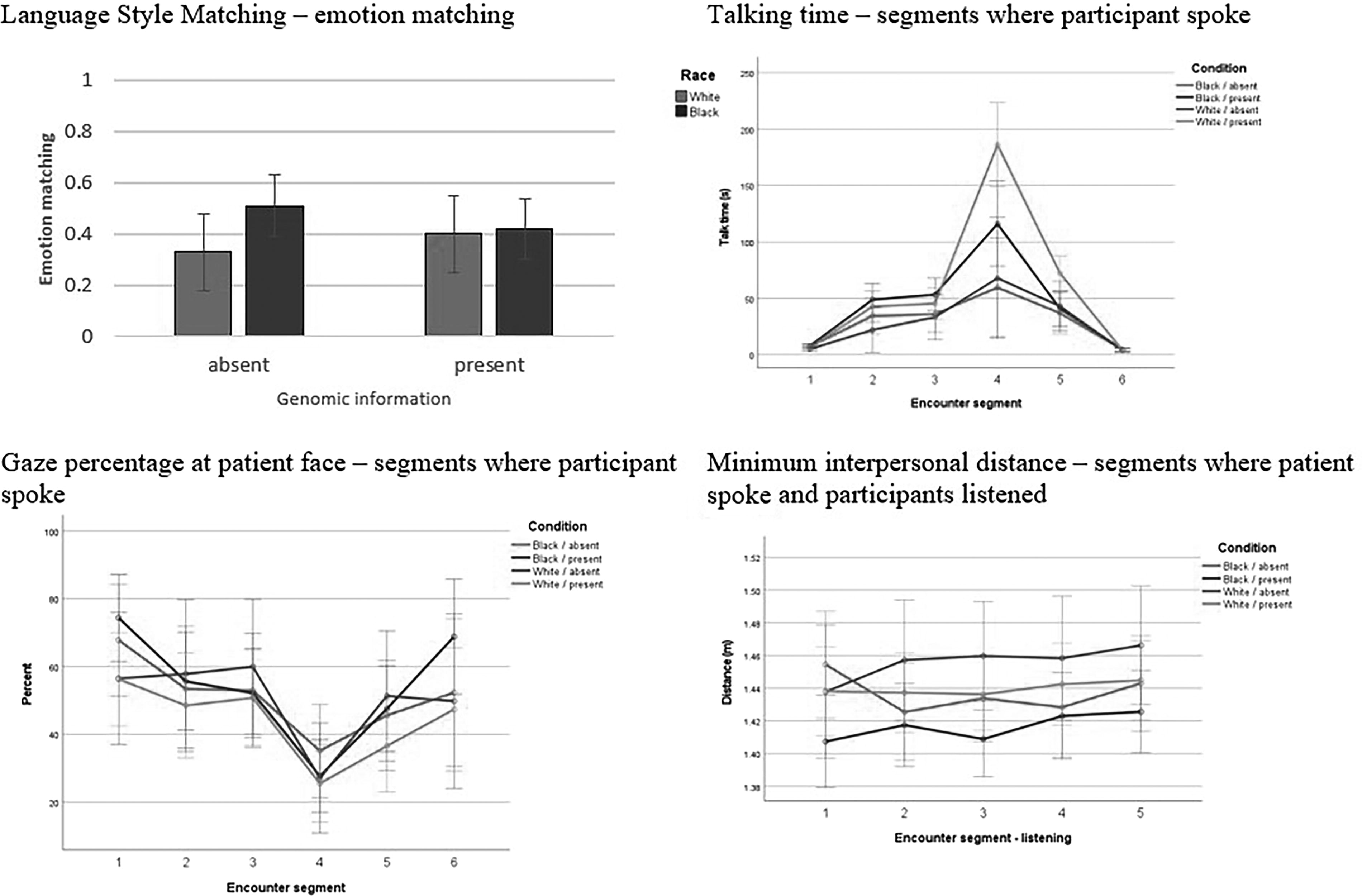
The extent to which participants matched the emotional tone of the virtual patient depended on the patient’s race and genetic risk status (Fig. 4). There was a significant main effect of race, qualified by a significant interaction. There was no significant main effect of genomic information. Participants were more likely to match the emotional tone of the virtual patients if they were Black, but this was tempered if genomic information was provided.
Graphical representations of significant implicit measure findings; error bars denote 95% confidence interval.
Talk time (implicit bias)
Over the aggregate encounter, analyses revealed a main effect such that participants who received genomic information spent more time talking, and thus had a longer encounter, than those who did not. There was no main effect of race or significant interaction. Repeated-measures ANOVA revealed an effect of visit segment [F (1.78, 141.65) = 53.81, p < 0.001], an interaction between segment and genomic information provision [F (1.78, 141.65) = 10.12 p < 0.001], and an interaction between segment and race [F (1.78, 141.65) = 3.31, p = 0.042]. The three-way interaction did not reach significance. Participants who received genomic information and those who interacted with the White patient talked for longer, and this was most apparent in the segment when genetic test results were discussed.
Gaze direction (implicit bias)
There was a main effect in the aggregated encounter, such that participants looked at the Black patient more frequently. There was no main effect of genomic information or interaction. Repeated-measures ANOVA of gaze direction across segments in which the participant spoke revealed an effect of segment [F (4.1, 258.32) = 13.52, p < 0.001], with no other main effects or interactions. Segments where the participant was listening to the patient did not differ.
Interpersonal distance (implicit bias)
There was a main effect of patient race over the aggregated encounter such that participants leaned in toward the Black patient than the White patient and no main effect of genomic information or any significant interaction. Repeated-measures ANOVA of minimum distance across segments in which the participant spoke revealed no main effects or interactions. Repeated-measures ANOVA of minimum distance across segments in which the patient spoke and participants listened revealed no significant main effects. There was a significant interaction between segment, race, and genomic information [F (3.17, 224.80) = 2.72, p = 0.043]. Contrasts suggest that participants tended to approach the Black patient with genomic information at the closest distance, whereas minimum distance from the White patient with control information was the largest, although this latter pattern only emerged after the first segment.
Discussion
The overall picture of bias and negative attitudes exhibited in the current study differed substantially from hypothesized patterns, but in several instances indicated an interesting interaction between apparent race and the provision of genomic information. We found no persistent main effect of race, and where we did see differences, they were counterhypothesis with participants more closely approaching the Black patient and matching their emotional tone to a greater degree—both generally considered indicators of positive attitudes. We found no evidence for a main effect of genomic information to mitigate bias. These patterns likely relate to the evidence we did find for an interaction between apparent race and the provision of genomic information on implicit and explicit bias. It is critical to note, however, that the nature of these interactions was not fully hypothesis-consistent.
For two measures of explicit bias and one measure of implicit bias, we found that medical students tended to express more negative attitudes toward the White virtual patient than the Black virtual patient (both of whom had obesity), particularly when no genomic risk information was present. This is surprising given the widely demonstrated racial biases throughout the health care system. This finding is, however, quite consistent with the literature focused on race–weight intersectionality for women in the United States and lends credence to the notion that Black women with obesity may be met with less weight-related bias in clinical health care encounters. Because the encounter was virtual, everything about the patient aside from her apparent race was held constant, and as such we can conclude that apparent patient race caused these differences in bias.
When genomic risk information was provided, it often mitigated bias for the White virtual patient, whereas negative attitudes and bias against the Black virtual patient either remained consistent or increased. Genomic information has previously been influential on bias and stigma in patient–provider encounters. The current work extends this area of research suggesting that direct-to-consumer genomic information with relatively small increases in risk is sufficient to alter bias impressions in some cases. Provision of information indicating heightened genomic risk for obesity might be applied as a causal explanation, lowering perceptions of patient fault and thereby lowering bias, at least in the case of the White patient. This explanation seems likely given that shifts in bias were found among study variables rooted in notions of fault and blame. However, it is not possible to tease apart what element of the risk information resulted in these changes. Other possible explanations include the notion that the genomic information induced cognitive load, which reduced participants’ ability to act in a socially desirable manner,47,48 particularly toward the Black patient. This interpretation is less likely because many of the measures were implicit in nature and less subject to cognitive load. Relatedly, genomic information can introduce uncertainty into the clinical encounter, which is often met with the use of heuristics and biases, including those linked to the patient race. 20 It is not possible to definitively establish which mechanisms contributed to the results shown here. Regardless of the mechanism, it is not clear why genomic information did not reduce bias for the Black virtual patient. This may be related to aforementioned tendencies to apply mitigating information for a preferred social group while ignoring such information when making judgments about a nonpreferred group. 41 More research is needed to better understand this pattern.
Sample size and missing data are serious limitations for this study and findings should be considered preliminary. It is fortunate that the study included both implicit and explicit measures, including those that were assessed automatically by the VR environment. This study has several additional limitations. Varied patient weight status would enable a better evaluation of how race–weight intersectionality operates in this context and it is currently unclear how participant responses would have varied in response to lean versions of the virtual patients. It will also be necessary to conduct similar work using a wider representation of virtual patient racial categories as weight stigma is experienced across racial groups and effects of genomic information may vary. The sample size was also insufficient to examine the specific influence of participant demographics (e.g., race) on study outcomes. Our assessment of data missingness did demonstrate, however, that participant race did not influence decisions to answer versus skip self-report items. Further investigation into medical students’ reluctance to answer survey questions related to stereotypes and stigma is warranted. Previous work suggests that health care professionals may refrain from response when their attitudes are more negative. 49 This has important implications for future research as well as for efforts aimed at reducing bias and discrimination.
In all, this research leverages VR to provide a multifaceted look at the intersection of race and weight in the clinical setting and how future genomic technologies may differentially influence bias and stereotyping. The current findings and future work of this nature can contribute to the creation of educational materials, both for formative medical student training in social issues such as interpersonal bias and health equity, and as an accompaniment to the introduction and use of personalized genomic risk reports in clinical settings. This special case can also be used to illustrate the potential influence of extraneous factors on clinical encounters and medical practice. Genomic risk information is clinically important and may have the power to reduce negative attitudes about patients; however, it is crucial to develop genomic data provision approaches that make it positive for all and negative for none.
Footnotes
Acknowledgments
The authors would like to thank Dr. Paul Haidet for his contributions to the study planning. They also thank Christopher Fortney for assistance with material creation and data collection.
Author Disclosure Statement
The authors have no competing interests or conflicts to disclose.
Funding Information
This study was funded by the Intramural Research Program of the National Human Genome Research Institute. Grant number for funding received is Z01- HG- 200383.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.