
Abstract
Aim:
Identify and systematically review cohort studies examining the association between cyberbullying (CB) and suicidal ideation, attempted suicide, self-harm, and nonsuicidal self-injury (NSSI).
Methods:
Systematic literature review following PRISMA guidelines. Searches for relevant literature were conducted in Scopus, Web of Science, PubMed, PsyINFO, CINAHL, Embase, and Cochrane up until July 2023. Cohort studies were included that provided information regarding the association between CB and different dimensions pertaining to self-injurious thoughts and behaviors (SITB) separately. Gathered information included data on study characteristics, sample characteristics, prevalence, and associations between CB and variables pertaining to SITB. Findings were synthesized, and grouping studies as a function of the outcome variable was analyzed.
Results:
A total of 19 studies were included. Suicidal ideation was analyzed in 11 studies, with the majority (n = 8) reporting statistically significant positive associations (aOR = 1.88 [1.08, 3.29], β = 0.08 to 0.47). Only a single study conducted independent analysis of attempted suicide, finding a statistically significant association (aOR 1.88 [1.08, 3.29]). Outcomes regarding the self-harm variable were equivocal, with only two out of five studies finding a statistically significant association and one of these, which conducted a gender differentiated analysis, only finding a significant association in females. Studies that considered the NSSI dimension were also inconclusive, with only a limited number of studies (n = 5) producing contradictory outcomes.
Conclusion:
There is a need to continue exploring the relationship between CB and different dimensions within the spectrum of SITB through longitudinal studies. It is recommended that analyses adopt a new perspective in which short-term follow-up is prioritized or individualized follow-up periods are considered, given the rapidly changing nature of suicidal tendencies. It would be interesting to analyze the frequency, persistence, or severity of CB events and broaden research to include all age ranges. Special attention should also be given to potential gender differences and possible mediators or moderators.
Introduction
Cyberbullying (CB) is defined as the harm caused, intentionally, by one person to another online, through the use of computers, mobile telephones, and other mobile devices. 1 Throughout the world, 7 out of every 10 children, adolescents, and young people suffer CB. 2 Studies using representative populational samples indicate that prevalence in the European Union of CB ranges between 2.8% and 31.5%. 3
Suffering from CB can drive towards meaningful negative psychological maladjustments, such as more problematic internalization (e.g., depression, anxiety, and loneliness), somatic issues, stress, and negative emotions, while also leading to lower levels of well-being and life satisfaction. 4 CB has also been related to suicidal ideation, suicide attempts, and self-harm.5,6 This led some authors to coin the new phrase, cyberbullicide, which refers to suicides that are directly or indirectly linked to CB. 7
Suicide is the fourth leading cause of death among individuals aged between 15 and 29 years. 8 This is a global phenomenon that affects all regions, and, according to some authors, the prevalence of both suicide ideation and attempts significantly increased during the COVID-19 pandemic. 9
The self-injurious thoughts and behaviors (SITB) spectrum is defined as all thoughts and behaviors that involve deliberate physical injuries to one’s own body, whether imaginary or real, and extends to more passive desires, such as the desire to be dead. It is generally acknowledged that the suicidal SITB spectrum (suicidal ideation, plans to commit to suicide, and suicide attempt) is distinguished from the non-suicidal SITB spectrum, which includes non-suicidal self-injury (NSSI) and suicidal threats or gestures. 10 A number of research studies report that NSSI significantly increases future risk of suicidal behavioral to an even greater extent than does having a previous history of suicide attempts.11,12 The SITB spectrum is considered to represent an important public health issue, not only because it is associated with suicide but also because of the physical and psychological harm it causes to individuals and the resultant impact of this on health care. 13
Specifically, suicidal ideation is defined as all thoughts about actions that have the aim of bringing an end to one’s own life. 10 A meta-analysis conducted by Lim et al. estimates that the global prevalence of suicidal ideation over the course of one’s lifetime is around 18%. 14 A meta-analysis of cross-sectional studies conducted by John et al. highlights that children and young people who are victims of CB are 2.15 times more likely to develop suicidal ideation, 13 whereas a more recent meta-analysis indicates that this likelihood is even greater, leaving such individuals 3.52 times more likely of this outcome. 5
Attempted suicide refers to carrying out an action that has the potential of being lethal, with the intention of dying as a result of this action. 10 The global prevalence of attempted suicide is estimated to be around 6% according to the meta-analysis conducted by Lim et al., 14 while being a victim of CB during childhood and adolescence is significantly associated with a 2.57 and 3.52 times greater likelihood, respectively, of attempting suicide.5,13
Self-harm is defined a self-inflicted injury, regardless of suicidal intention or motivation. 15 According to data provided by a recent meta-analysis, its global prevalence is estimated to be 13.7%. 14 Evidence available at the time of writing indicates that children and young people who have suffered CB have a 2.35–3.57 times greater risk of developing self-harm behaviors.5,13
NSSI is defined as intentional and self-inflicted superficial harm to the body without suicidal intention. 16 NSSI prevalence across the lifespan is placed at around 22%, 17 with this issue also being significantly associated with CB.18,19
At the present time, various systematic reviews emphasize the relationship between CB and the spectrum of SITB. Nonetheless, all of these reviews share the same limitation that the majority of original studies examining the relationship between both issues have a cross-sectional design.5,13,20–22 This represents a substantial limitation regarding the validity of current evidence, given that the existence of a causal relationship between CB and the spectrum of SITB is not clearly defined.
Some findings suggest that individuals who experience mental health problems tend to turn more to the Internet and social networks as a way of mitigating their negative emotions or unfulfilled basic psychosocial needs. This leaves them potentially more open to being exposed to CB. 23 Likewise, various studies indicate that individuals with mental health problems are more likely to be victims of CB because of factors such as vulnerability or them being differentiated from their peers. 24 For this reason, it is not possible to make conclusions regarding causality and temporality based on cross-sectional studies.
Another aspect to consider is that the majority of published studies were conducted in adolescent (up until 19 years) and youth (up until 25–26 years) populations, yet CB also affects adults. 25 To the best of our knowledge, the systematic review conducted by Wilson et al. (2023) represents the most recent work on the topic. This review examined longitudinal studies published up until July 2021 on traditional bullying, CB, and the spectrum of SITB. This being said, the majority of included studies focused on traditional or face-to-face bullying and the review was limited to the child and youth population.
Thus, the present work seeks to address the gaps identified in research on this topic. A scientific literature review is presented that focuses, singularly, on the phenomenon of cybervictimization. It exclusively considers cohort studies, without imposing any limits on the age range of study populations and considering each individual dimension on the spectrum of SITB independently.
Objectives
General aim
Identify and systematically review cohort studies that analyze the association between CB and suicidal ideation, attempted suicide, self-harm and NSSI.
Specific objectives
Review and identify cohort studies conducted up until the present day that analyze the association between CB and some of the outcome variables.
Analyze the different dimensions of the spectrum of SITB and qualitatively synthesize findings reported by studies identified for inclusion.
Methodology
This systematic review was conducted in accordance with methodological recommendations outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guide. 26 The study was registered in Open Science Framework files pertaining to data, and data analysis is openly available (DOI 10.17605/OSF.IO/5QHF2). The present study is exempt from research ethics committee approval.
Data sources and search strategy
Web of Science (WOS), PubMed, PsyINFO, CINAHL, Embase, and Cochrane databases were consulted. The strategy, which combines MeSH (Medical Subject Headings) terms and keywords appearing in titles and abstracts, was initially designed for PubMed and later adapted and used in all remaining databases. The search strategy is detailed in Supplementary Appendix SA1, and search outcomes are summarized in Figure 1. Searchers were finalized on the July 13, 2023, with no restrictions being applied in terms of language or date of publication.
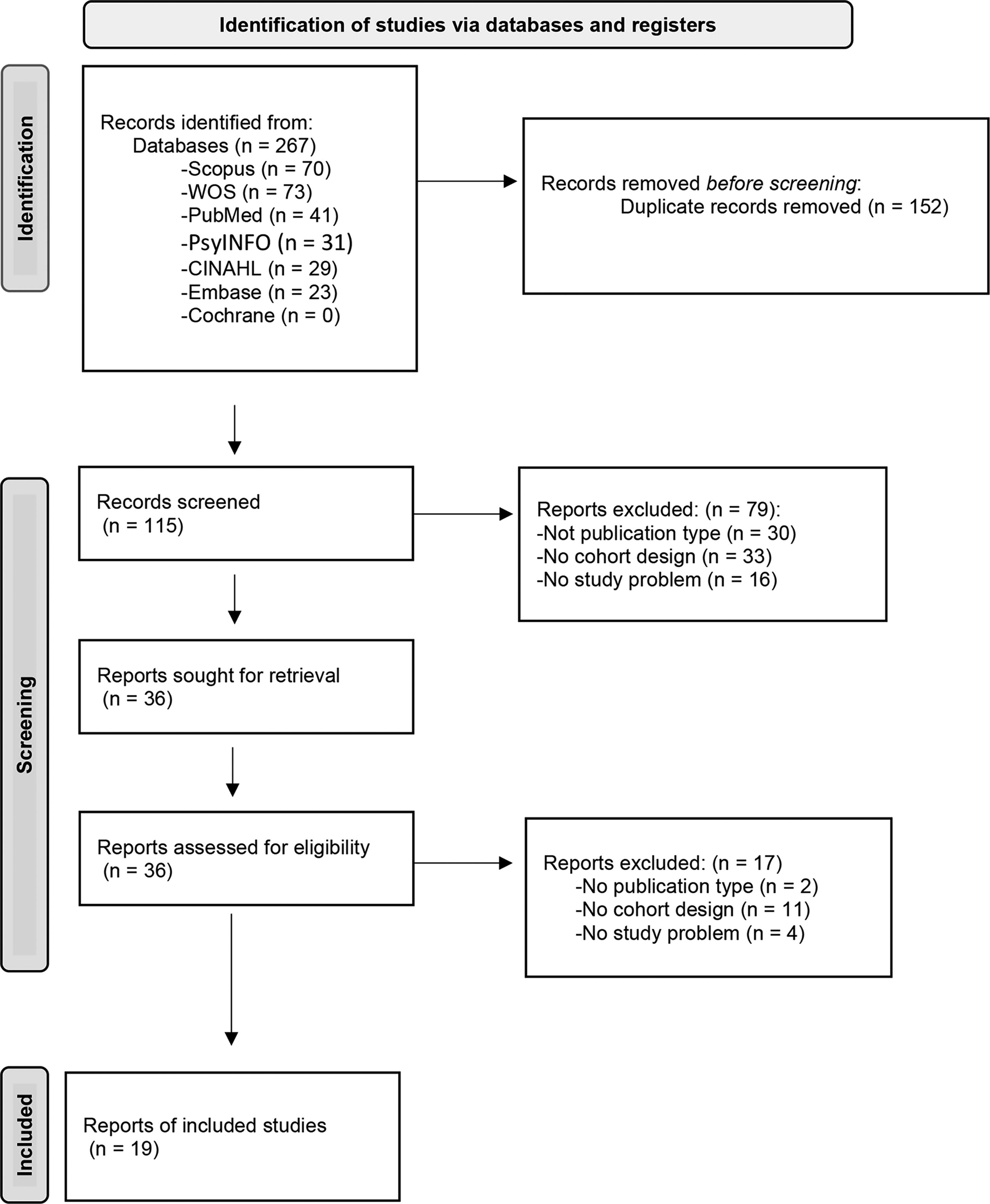
PRISMA flowchart of the study selection process.
Selection process
Inclusion criteria for study selection were defined as follows: Cohort studies analyzing the relationship between CB and different dimensions on the spectrum of SITB (suicidal ideation, attempted suicide, self-harm and NSSI).
Exclusion criteria for study selection were as follows: Unoriginal studies (narrative or systematic reviews, abstracts from conference proceedings, editorials, commentaries and letters to editors, etc.), qualitative studies, and observational studies in which the sample is not followed-up over time. Articles were also excluded if they did not gather data on cybervictimization via CB as an independent variable (e.g., included other types of bullying such as traditional bullying).
All references identified from the search strategy were imported and managed through the platform Rayyan QCRI. 27 Two reviewers (I.M.A. and G.P.M.) independently conducted an initial review of titles and abstracts with a view to later reading the full texts of potentially relevant articles. Selection criteria were applied to determine article eligibility. In cases in which there was disagreement, a third reviewer (V.B.H.) was consulted in order to reach a decision based on consensus.
Data extraction
Forms were designed for data extraction to gather information on the main characteristics of studies included in the review, alongside outcomes pertaining to the methodological quality assessment. Collected data included study characteristics (authors, year of publication and year of data collection, country, sample size, and cohort follow-up period), sample characteristics, and prevalence and association between CB and variables included on the spectrum of SITB (effect size and 95% confidence intervals). Further, in cases in which analyses were adjusted for covariates or mediation/moderation analyses were performed, adjustment variables were listed. One reviewer (I.M.A.) extracted key information from each study. This information was later verified by another reviewer (G.P.M.).
Methodological quality assessment
Methodological quality assessments were performed for all included studies. For this, the Newcastle-Ottawa Scale (NOS) for cohort studies was used. This scale is based on three categories (selection, comparability, and outcome) and comprises eight criteria. 28
With regard to the comparability category, the most important confounding factor to control for when performing analyses was considered to be the antecedents of mental health issues. With regard to the follow-up period criteria within the outcome category, a follow-up period of 12 months or less was considered to be sufficient, taking as a reference a meta-analysis that points out the importance of short follow-up periods when investigating SITB spectrum. 29
The NOS produces scores that range from 0 stars (high risk of bias) to 10 stars (low risk of bias). Studies receiving scores of between 7 and 10 stars were considered to have a low risk of bias, whereas studies with between 4 and 6 stars were rated as having a medium risk of bias and studies with between 0 and 3 stars were rated has having a high risk of bias. Two reviewers (I.M.A. and G.P.M.) assessed the methodological quality of included articles, and discrepancies were discussed and resolved through consensus.
Synthesis of findings
First, descriptive analysis was performed to examine the distribution of included studies according to characteristics pertaining to design, publication, and methodological quality. Following this, outcomes were synthesized by grouping studies as a function of the outcome variable under study, namely, suicidal ideation, attempted suicide, self-harm, and NSSI.
Results
Study selection
Figure 1 shows search outcomes. A total of 267 references were identified, of which 152 were duplicates. After reading the full texts of articles, 19 references were selected to form the final sample of the systematic review. Reasons for which articles were excluded are detailed in Figure 1.
Study characteristics
Table 1 summarizes the characteristics of included studies. The 19 selected studies were published between 2014 and 2023, with the majority of these (n = 12) being published between 2021 and 2023. Most (n = 10) studies presented data that had been collected prior to the year 2018. In six studies, the year in which data were collected was not specified.
Summary of Study Characteristics
With regard to the follow-up period, most studies (n = 12) followed the population under study up over a period of 6–12 months, with the most frequent time period being 12 months of follow-up. In five studies, the sample was followed up over time periods that were longer than one year and, in only two studies, follow-up time-periods shorter than 5 months were used.
Studies were distributed across Asia (n = 7), North America and Oceania (n = 6), and Europe (n = 6). Sample sizes ranged between 121 and 16,292, with the median being 1,192. Participants involved in the studies had ages that ranged between 10 and 29 years. One study conducted with a university population did not report the age of participants. 30 Prevalence of CB ranged between 2.6 and 28.8%, although most studies (n = 12) did not provide this data.
With regard to examined dimensions of the spectrum of SITB, a total of 23 items pertaining to outcome variables were examined across the 19 studies (Table 2). The most commonly examined dimension was suicidal ideation (n = 11), followed by self-harm (n = 5), NSSI (n = 5), and attempted suicide (n = 1). One study analyzed suicidal ideation and attempted suicide as a single variable. The prevalence of suicidal ideation ranged between 4.92 and 27.02%, ideation alongside attempted suicide ranged between 13.3 and 25.5%, self-harm prevalence ranged from 0.0069% to 12%, NSSI prevalence ranged from 14.5 to 22.01%, and attempted suicide had a prevalence of 4.6%. With regard to 10 of the items under analysis, prevalence was not reported.
Summary of Outcomes
The total does not add up to 19 because an article can consider more than one variable (total number of outcome variables = 23).
A total of 9 studies performed mediation or moderation analyses involving different variables with the potential to affect the relationship between CB and subsequent suicidal ideation (n = 6), or between CB and subsequent NSSI (n = 5). With regard to gender, aggregated data as a function of gender were not presented for the majority of outcome variables (n = 15).
Methodological quality
Methodological quality pertaining to all studies overall was medium (between four and six stars). Most common risk of bias emerged in relation to two of the selection criteria because of the fact that data for the exposure variable were gathered through self-administered questionnaires (n = 18) or that the method of data collection was not reported (n = 1), and that none of the studies were able to demonstrate that the outcome variable was not present at the beginning of the study. Common bias pertaining to comparability criteria were that many studies failed to control for the main variable, while in regard to the outcome category, data for the outcome variable were mostly gathered using self-administered questionnaires (n = 17), and data were lost during follow-up (Table 3).
Evaluation of Methodological Quality
Newcastle-Ottawa Scale (NOS). An asterisk (*) denotes a quality rating of one star on the NOS, indicating the level of methodological quality.
Synthesis of outcomes
Association between CB and suicidal ideation
A total of 11 studies4,24,30–38 examined the association between CB and suicidal ideation (Supplementary Appendix SA2). Some studies (n = 3) reported non-significant associations;24,31,32 however, the majority (n = 8) reported statistically significant positive associations.4,30,33–38
Only one of the three studies whose outcomes were reported in terms of ORs indicated that risk of suicidal ideation was greater in CB victims, in this case increasing risk by a factor of 1.88.33 In studies reporting regression coefficients (n = 8), associations were found to be significant in seven studies, with values ranging between 0.08 and 0.47.430,34–38
Six studies performed some type of mediation or moderation analysis, considering a range of variables.4,30,34,36–38 Analyses concluded that six of the seven analyzed variables either moderated or mediated the relationship between CB and later suicidal ideation, with protective factors being life satisfaction, high core self-evaluation (a combined indicator of self-esteem and emotional self-regulation) capacity, parental support, perceived social support, and mindfulness. On the other hand, one study revealed that depression mediated the association between CB and later suicidal ideation. 30
Five studies produced some kind of outcome regarding the influence of gender on the association between CB and suicidal ideation,24,30–32,37 with significant gender outcomes emerging in two of these studies. Mediation analysis performed in a study conducted by Fu et al. 30 indicated that female CB victims were at greater risk of depression, which, in turn, increased the risk of suicidal ideation. A study conducted by Maurya et al. 32 indicated, after performing analysis adjusted for CB, that prevalence of suicidal ideation was three times higher in females than in males.
Association between CB and attempted suicide
One study analyzed the association between CB and attempted suicide, finding a statistically significant association (aOR 1.88 [1.08, 3.29]). 33 One study analyzed suicidal ideation together with attempted suicide and produced non-significant outcomes (aOR 1.37 [0.97–1.93]) 39 (Supplementary Appendix SA2).
Association between CB and self-harm
A total of five studies analyzed the association between CB and self-harm24,40–43 (Supplementary Appendix SA2). Outcomes reported as ORs or hazards ratios (n = 2) were not statistically significant (aHR: 1.2 [0.4, 3.3] and aOR: 2.01 [0.82, 4.92]). In studies that provided regression coefficients (n = 2), one study reported an inconclusive association (β = −0.03 [−0.13, 0.08]), while another study reported a weak positive relationship (0.13, p < .001). Finally, only one study performed a gender-stratified analysis. This study revealed that suffering CB was only associated with a greater risk of self-harm in females (aOR: 2.42 [1.41, 4.15]) but not in males (aOR: 1.59 [0.35, 7.26]). 43
With regard to gender, one further study conducted gender-specific analysis but did not produce statistically significant outcomes. 24
Association between CB and NSSI
A total of five studies analyzed the association between CB and NSSI36,37,44–46 (Supplementary Appendix SA2). Associations were statistically significant in three studies, with regression coefficients that revealed weak-medium strength associations through correlations of between 0.08 and 0.31.37,45,46
These five studies performed some type of mediation or moderation analysis to examine the influence of different variables on the relationship between CB and NSSI. A study conducted by Lin et al. 45 identified self-esteem and peer attachment as protective factors. Two studies analyzed parental support, with this emerging as a protective factor in only one of these studies. 37 Two studies established that depression and anxiety mediated the association between CB and NSSI, with emotional reactivity and self-control, respectively, moderating these aforementioned relationships.44,46
Only one study performed a gender-differentiated analysis, and this did not produce statistically significant outcomes. 44
Discussion
The review included a total of 19 longitudinal studies that analyzed the association between CB and different manifestations of the spectrum of SITB, namely, suicidal ideation, attempted suicide, self-harm, and NSSI. Given that most existing evidence at the time of writing comes from cross-sectional studies and that the possibility of inverse causality has not been explored in existing previously conducted research, the present study focused exclusively on longitudinal studies with the aim of addressing this deficit and more accurately establishing causal relationships. In addition, another strength of the present study is the broad search strategy used, unrestricted in terms of age, date, country, and language.
With regard to the association between CB and suicidal ideation, some studies indicated the existence of a weak non-significant relationship; however, most studies consistently supported the existence of a statistically significant positive relationship. This agrees with evidence produced by systematic reviews performed on cross-sectional studies.5,13 The three studies that did not produce evidence of significant associations came from broader cohort studies and, therefore, included larger sample sizes; however, it is possible that they were not specifically designed to address the question at the heart of the present study. These three studies also included, generally speaking, longer follow-up periods (8, 24, and 36 months). In contrast, in the studies that reported statistically significant associations, sample selection was performed via convenience or randomly in line with study needs and shorter follow-up periods were examined.
A meta-analysis including 365 longitudinal studies addressing potential risks related to an outcome on the SITB spectrum concluded that only 16.39% of reviewed articles used follow-up periods shorter than 1 year. This review concluded that, although studies with longer follow-up periods may, generally, have greater predictive capacity as they capture more events, this reasoning cannot be applied to research addressing suicidal behaviors and thoughts, given that many factors could induce an increase in risk during only a short period of time. For this reason, it is maintained that studies with short follow-up periods are potentially stronger, methodologically, when it comes to analyzing possible risk factors behind suicidal behaviors and thoughts. This is especially true when concerning time-dependent risk factors. 29 That discussed above is applicable to the present study hypothesis, given that potential repercussions of CB will be born out over time and depend on the specific characteristics of the event. Indeed, a single CB event in isolation will not have the same repercussions as various events occurring over time.
With regard to attempted suicide, the present review reveals a scarcity of studies addressing this issue. Only one single study considered attempted suicide as an independent variable. This study revealed a significant association between prior experience of CB and a later suicide attempt. This finding corroborates outcomes reported by cross-sectional studies.5,13 Nonetheless, the present review reveals that this is an area in need of further research through longitudinal studies, with the lack of research on this issue potentially being, at least partly, because of the low prevalence of the phenomenon of attempted suicide.
Findings regarding the relationship between CB and self-harm were less conclusive. Most studies found this relationship to be nonsignificant in contrast to other existing evidence.5,13 Nonetheless, findings reported by a study conducting gender-stratified analysis 43 stand out in that they revealed that a significant association did exist but only in females. Various studies have indicated that the female gender is associated with a greater risk of falling victim to CB. Further, it is well acknowledged in existing literature that females are at a greater risk of suffering from mental health issues.47,48
The present review presents evidence that research is lacking on the gender impact on potential relationships between CB and suicidal behaviors and thoughts. The few studies to perform gender-differentiated analysis mostly indicated an absence of statistically significant differences. Nevertheless, as is mentioned above, the studies that did uncover significant differences suggest, in accordance with other existing literature, that females represent a more vulnerable group and highlight the importance of considering gender differences when conducting research in the fields of health and sociology.47,48
With regard to the NSSI dimension, reviewed studies also failed to produce conclusive outcomes, with only a limited number of studies being available and findings being contradictory. Thus, the need is urged to continue to broaden current research on the topic through longitudinal studies that enable causality to be established with regard to the relationship between CB and NSSI.
With respect to the methodological quality of reviewed studies, all were rated to be of medium quality, with a number of areas emerging with the potential for methodological improvement. For example, studies were limited by the fact that data were gathered through self-administered questionnaires, leading to greater risk of bias, recall bias, interpretation bias, and social desirability. Another notable limitation is that, despite only cohort studies being included, not a single study demonstrated that the outcome variable was not present at the beginning of the study. Further, one study was found that reported a follow-up period that was shorter than the period of time during which the outcome variable was measured. This could lead to bias due to the possibility that the outcome variable was already present prior to exposure.
With regard to comparability criteria, while all studies controlled for other variables, only half controlled for the variable considered to be the most important for being able to discount the possibility of inverse causality, namely, the antecedents of mental health issues. Turning attention to the follow-up criterion, while most studies met criteria regarding the suitability of the follow-up period (12 months or less), it would be useful to examine shorter follow-up periods, given that studies with long follow-up periods may be faced with greater noise that makes analysis more challenging. 6
Given that the search was not limited according to age, the present review reveals that no studies exist in the child population (younger than 10 years) or the adult population (older than 29 years). In the case of the former, this represents a deficit given that access to the Internet and mobile devices is initiated at increasingly younger ages. 49 With regard to the adult population, more than 90% of adults aged between 25 and 54 years, and approximately 75% of those aged between 55 and 74 years regularly use the Internet. 50 Hence, not only adolescents and young people are exposed to the phenomenon of CB, making it important to broaden the age range of individuals recruited to participate in future research.
Findings of the present review reveal complex patterns and variants inherent to the relationship between CB and suicidal behaviors and thoughts. A number of included studies performed mediation and/or moderation analyses and produced findings which suggest that the effect of CB on suicidal ideation and NSSI is partly explained through pathways mediated by other variables, such as depression for both of the aforementioned variables and anxiety in the case of NSSI. Likewise, mediating factors were detected that could have a protective influence. Potential mediators include life satisfaction, self-esteem and emotional self-regulation, parental support, perceived social support and peer attachment, and mindfulness. These findings are of paramount importance, given that they open the door to the use of new tools in the fight against CB. Such tools include interventions targeting the development and reinforcement of skills in young people, such as self-esteem and emotional regulation, so that children and young people are equipped to effectively tackle and manage CB events, should they take place, in this way, avoiding further damage to health.
Limitations
A limitation to note in this study was the inability to conduct a meta-analysis, despite its initial inclusion to better assess the robustness of the observed positive associations. Consequently, several authors were contacted to obtain additional data. However, despite their cooperation, performing the meta-analysis proved impossible due to the diversity of statistical analyses used and the wide range of outcome variables, compounded by the limited number of articles available.
Conclusions
The present review highlights the complexity of examining longitudinal relationships between CB suicidal behaviors and thoughts. Various studies supported the existence of a statistically significant association between exposure to CB and greater risk of suicidal ideation, with findings pertaining to relationships between CB and suicidal intention, self-harm, and NSSI not being as consistent.
The need is identified to continue to explore the aforementioned associations through longitudinal studies, preferably from a new perspective that prioritizes short of individualized follow-up periods, given the rapidly changing nature of suicidal tendencies. At the same time, it would be highly informative to examine risk factor characteristics, such as the frequency, persistence, or severity of CB events and broaden research to include all age ranges. Special attention should also be given to potential gender differences and mediating or moderating factors such as depression and anxiety. Given its public health implications, suicide prevention must take a comprehensive approach that includes interventions directed toward, not only the prevention of CB but also the development of skills and resources that enable episodes of CB to be effectively tackled and managed, should they occur, while, at the same time, promoting a safe and healthy online environment.
Footnotes
Acknowledgment
The authors would like to thank Camila Higueras-Callejón for conducting the literature search and for her support throughout the article preparation process.
Authors’ Contributions
I.M.A. Conceptualization, methodology, formal analysis; writing—original draft, and visualization. V.B.H.: Conceptualization, methodology, and writing—review and editing. I.R.P.: Conceptualization; funding acquisition, writing—original draft, and supervision. C.H.C. Methodology. G.P.M.: Conceptualization and writing—review and editing.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work and the article processing charge was funded by Carlos III Health Institute (ISCIII)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.