
Abstract
Atopic dermatitis (AD) is a chronic inflammatory skin disease with a significant psychological impact. The cardinal symptom of all phenotypes and severities is chronic pruritus with repetitive itching and scratching due to a vicious itch–scratch cycle that can be worsened or triggered by stress. Neuroimaging of brain areas responsible for itch processing in healthy subjects versus patients with AD has provided insights into the brain circuits involved in itch central perception. In patients with AD, the dorsolateral prefrontal cortex appears to be overactive while regulating the itch–scratch circuit, and this persistent hyperactivation over time may disrupt this brain region. Common mechanisms between addiction and scratching could explain why some patients with AD continue to scratch despite showing clinical improvements from conventional treatments. In addition, molecular knowledge indicates bidirectional neuroimmune circuits between the peripheral nervous and immune system and dysregulated skin cells may aggravate and perpetuate AD severity. We provide an overview of the basic mechanisms that underlie the itch–scratch cycle in AD, especially neural sensitization of nonhistaminergic itch-specific pathways, and discuss how integrative therapies may interfere with central and peripheral mechanisms of chronic itch to reduce neuroinflammation and break the itch–scratch cycle. The connection between mind and body in the itch–scratch cycle, involving central mechanisms, suggests that integrative and multidisciplinary treatment approaches could be helpful as an adjunct to pharmacological treatment in the clinical management of AD. Integrative therapies may potentially help to reduce pruritus and scratching, psychological stress and sleep disturbances, and improve immune and skin barrier dysregulation, AD outcomes, and patient well-being.
Capsule Summary
Interrelated itching, scratching, sleep disturbances, and psychological stress may lead to a vicious itch–scratch cycle in patients with atopic dermatitis (AD).
Dysregulated peripheral neuroimmune circuits initiate, aggravate, or perpetuate skin barrier dysfunction and immune dysregulation and may worsen itch and pain.
Patients with AD demonstrate changes in brain circuits modulating itch responses, sleep quality, stress responses, and thereby inflammation and skin barrier dysfunction in a bidirectional way.
Although new pharmacological therapies for AD can modulate adaptive and innate immunity, skin barrier dysfunction, or neuroimmune circuits, AD management may require a multidisciplinary integrative treatment approach to address all aspects of the disease, especially to alleviate pruritus, decrease scratching, and improve psychological well-being. Integrative therapies could potentially interfere with the central and peripheral mechanisms of chronic itch to reduce neuroinflammation and break the itch–scratch cycle.
INTRODUCTION
Atopic dermatitis (AD) is a very common, complex, highly heterogeneous, chronic inflammatory skin disease that affects children and adults. It is characterized by different subtypes/phenotypes based on age, severity, ethnic background, mutations (eg, filaggrin or immunoglobulin E status), and underlying differences in molecular mechanisms defining a variety of phenotypes and endotypes. 1 The cardinal symptom of all phenotypes and severities in AD is pruritus, especially chronic pruritus (over 6 weeks duration), which is the most burdensome symptom. 2 However, repetitive itching and scratching, which perpetuates inflammation and skin barrier dysfunction, leads to a vicious itch–scratch cycle that remains challenging to treat. 1
In this review, we provide an overview of the psychological impact of chronic pruritus in patients with AD and the mechanisms underlying the itch–scratch cycle to highlight the potential of an integrative and holistic approach for alleviating intractable itch and improving patient clinical outcomes and psychological well-being.
BURDEN OF ITCH IN AD
Patients with AD often identify pruritus as the most burdensome symptom when describing treatment needs. 3 Chronic recurring itch significantly impairs quality of life (QoL) in patients with AD4,5 and may be underestimated by physicians, highlighting the importance of focusing on itch when evaluating treatment options for AD. 6
PSYCHODERMATOLOGY OF ITCH
The relationship between mind and skin and associations with stress is well established, as psychological stress can trigger AD and perpetuate itch.7,8 Pathophysiological pathways between skin and mental disorders (eg, anxiety, depression, attention deficit hyperactivity disorder [ADHD], emotional problems, and suicidal ideation) may involve T helper 2-mediated systemic inflammatory responses and stress–system disorders (ie, overactivation of the sympathetic nervous system and hypothalamic–pituitary–adrenal [HPA] dysregulation), 9 as well as neuroinflammatory circuits (eg, neuropeptides activating central receptors).10-12 In response to acute itch, scratching, and mental stress, patients with AD had a significantly higher heart rate than healthy controls, indicating an autonomic nervous system dysfunction that may reflect the itch–scratch cycle perpetuating stress 13 ; this is also reflected by the clinical sign of white dermographism. 14 Furthermore, following acute stress, patients with AD reported a reduction of cowhage-evoked itch sensation but exhibited an increase in spontaneous off-site scratching. In patients with AD, higher sensitivity to stress over time with increased spontaneous scratching may aggravate the itch–scratch cycle, as well as decrease the threshold for neural sensitization, thereby increasing the severity of AD and itch.14B15 -18
Itch and neuroimmune dysregulation, in which peripheral itch mediators communicate with the brain, may contribute to depression and decreased QoL.12,16,17 In a longitudinal study, 9% of patients with chronic pruritus had a psychosomatic consultation, and 77% of these had a psychological comorbidity. 19 A systematic review on cohort and case–control studies found comorbid psychopathologies frequently associated with chronic pruritus in patients with AD were depression, anxiety, and sleep disorders.20,21 Compared with controls, patients with AD were more neurotic, less extraverted, less agreeable, and more depressed. Also, they were more sensitive to itch-inducing material, with a higher increase in scratching when watching a video of crawling insects than when watching a control video. 22 In patients with AD, an association between greater induced scratching and lower agreeableness was observed, suggesting that this group of patients may benefit most from psychological interventions. 23 Pruritus was positively correlated with anxiety state and anxiety trait, with a significant effect on QoL. 24 In a large, longitudinal, birth cohort study, severe AD was associated with symptoms of depression. 25 Furthermore, in a systematic review and meta-analysis, patients with AD were 44% more likely to have suicidal ideation and 36% more likely to die by suicide than healthy individuals. 26
A potential link between patients with AD and ADHD and atypical neurodevelopment has been suggested27,28 but could be related to several factors, including sleep disturbance, stress, and impaired HPA axis.21,29-31
Promoting adequate sleep for patients with AD is extremely important as sleep disturbance may contribute to cutaneous, systemic, and possible brain inflammation, which are key drivers of psychiatric disorders. 5 Poorer sleep quality due to nocturnal scratching and difficulty functioning during daytime activities in patients with AD are correlated with increased pruritus severity and lower QoL. 32
Due to the psychological burden of chronic pruritus in patients with AD, treating itch is important to improve well-being, and these patients might benefit from certain psychological interventions. However, the complex pathophysiology of chronic itch in AD, which involves an interplay of different mechanisms and pathways from the skin to the spinal cord and brain, is not fully understood and may explain why finding effective solutions to break the itch–scratch cycle remains challenging.1,16,33,34
MECHANISMS OF ITCH IN AD
Basic Mechanisms of Itch
The basic mechanisms of itch have been reviewed elsewhere.1,16,34B35 -39 Briefly, itch is initiated when allergens, pruritogens, and irritants, for example, activate cutaneous nerve fibers involved in itch sensing, which are the epidermal dendritic extremities of sensory neurons whose cell bodies are found in the dorsal root ganglia. Itch can be directly (or indirectly) stimulated by exogenous trigger factors such as house dust mites, Staphylococcus aureus, or irritants.1,40,41 Alternatively, itch may be a consequence of a dysregulated adaptive and/or innate immune system resulting in sustained neuroimmune interactions where, for example, immune cells release mediators that not only induce inflammation but also itch.35,42B43 -46
Recent research suggests that epidermal keratinocytes sense itch stimuli and release itch mediators, which subsequently activate itch receptors on sensory nerve endings. They interact tightly with intraepidermal and dermal nerve fibers via ligand-receptor binding, activating, and/or sensitizing sensory nerves.45,47B48 -53 Keratinocytes also communicate with immune cells (eg, T cells, mast cells, eosinophils) that, in turn, release itch-inducing mediators such as cytokines or proteases.43,54 Subsequently, the itch signal is propagated along neural pathways to the spinal cord and to the brain to induce the perception of itch that provokes scratching. 55 The two major itch pathways (histamine-dependent and histamine-independent) mostly involve distinct receptors and distinct cutaneous nerve fibers that follow separate spinothalamic tracts to connect with different neural pathways in the central nervous system (CNS).16,17,56 Although they activate slightly different brain areas, several core brain regions are activated by both pathways (eg, thalamus, somatosensory cortices, anterior and posterior cingulate cortex) as demonstrated in a human functional imaging study.57,58 The pathophysiology of chronic itch in AD is predominantly underpinned by the nonhistaminergic pathway.34,42 The etiopathogenesis of pruritus, illustrating the connection between the brain and the skin, and the main psychoneuroendocrinoimmunology mechanisms involved in the link between distress and chronic pruritus have previously been described.8,59,60
The Itch–Scratch Cycle in AD
In AD, itching and scratching frequently lead to a vicious itch–scratch cycle with immune dysfunction, inflammation, and sensitization, while the subsequent scratching disrupts the skin barrier, allowing allergens, pollutants, and microbes to enter, further exacerbating itch.1,61B62 -64 Various triggers may activate different parts of the complex vicious cycle to aggravate and perpetuate each other.1,65 The itch–scratch cycle describes the complex interplay between itching and scratching, which leads to worsening skin inflammation (the itch–scratch cycle), with additional interrelated negative effects of sleep disruption and psychological stress (the scratch–sleep cycle), as represented in Figure 1.
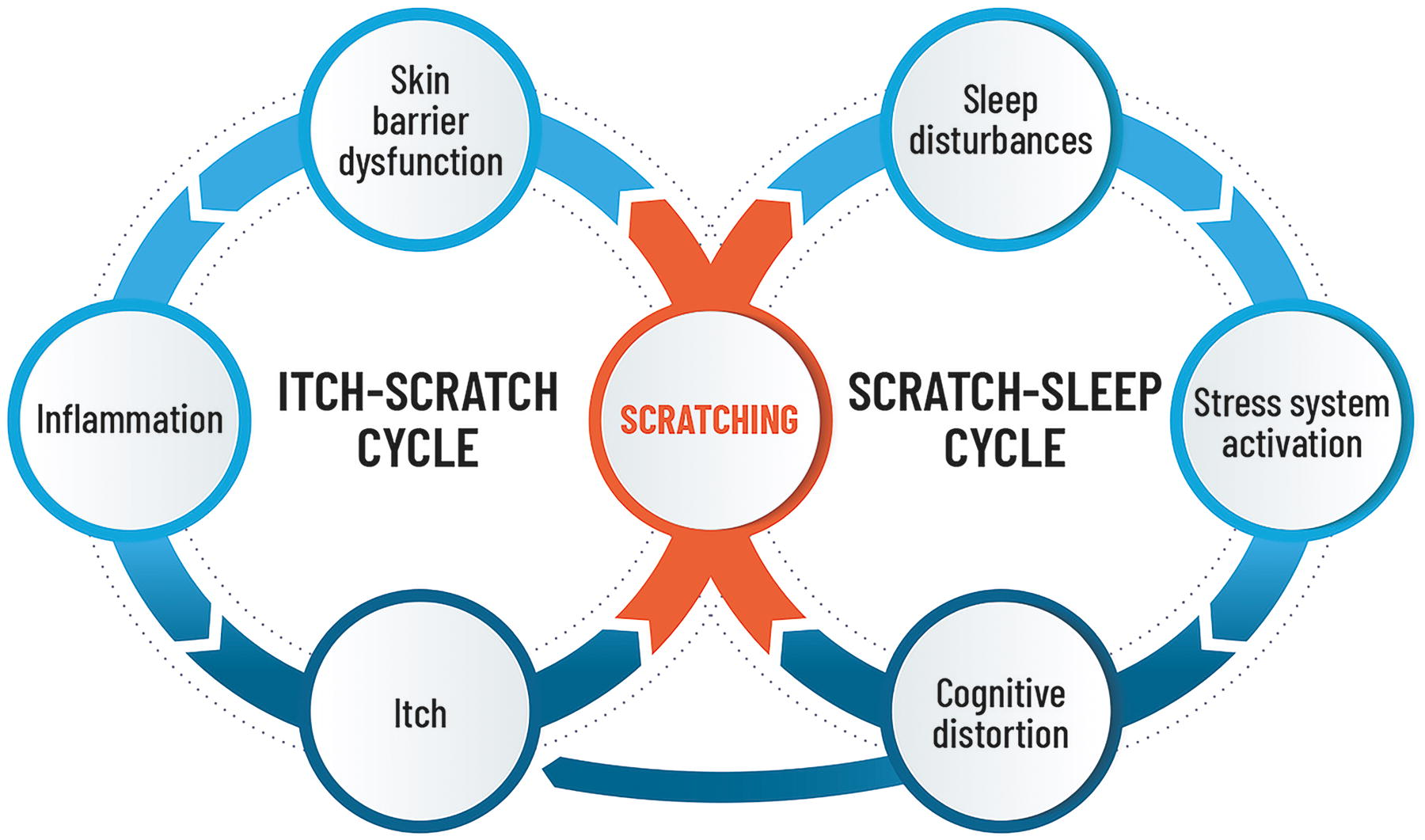
Interrelated cycles of itching, scratching, sleep disturbances, and psychological stress in patients with atopic dermatitis.
Activation of sensory nerve fibers by pruritogens (eg, cytokines, proteases, and other mediators) promotes neurogenic inflammation and sensitization of nerve fibers, resulting in dysregulation of neuroimmune circuits and chronification of itch, inflammation, skin barrier dysfunction, and thus therapy resistance. 1 Although scratching can temporarily relieve itch in healthy subjects, chronic itch in patients with AD can drive persistent scratching responses that aggravate itch and dermatitis in a vicious cycle, for example, involving activation of toll-like receptor-3 in keratinocytes. 63 The injured “scratched” keratinocytes in lesional skin thereby release itch mediators, such as endothelin-1 or thymic stromal lymphopoietin (TSLP), 63 and aggravate neuroinflammation by perpetuation of interleukin (IL)-31 release.1,35,46 Type 2 inflammatory mediators are part of the neuroimmune axis and directly stimulate nerve fibers, while IL-4, IL-13, and IL-31 cytokines are also involved in neural sensitization so that neurons become hypersensitive to stimuli.1,66
Chronic Itch and Neural Sensitization
In patients with AD, persistent itching and scratching exacerbate skin sensitivity and neural sensitization, 62 which involves itch, pain, burning sensation, and neuroinflammation.36,65,67,68 Neural sensitization in patients with AD causes an increase in sensitivity of itch‐selective neurons at the level of the skin, spinal cord, and brain,16,17 with alloknesis (where nonpruritic stimuli are perceived as itch) and hyperknesis (increased sensitivity of nerves to pruritic stimuli).33,69 Somatosensory sensitivity to pruritus induced by various stimulations (eg, chemical, thermal, and mechanical stimuli) has been observed in patients with AD, especially in lesional skin, and this sensitization with neuroimmune dysregulation, for example, by increased levels of IL-31, 70 is a major factor driving chronification (pruritus lasting over 6 weeks).34,69
The nervous system becomes hypersensitive to itch stimuli or other factors involving various signaling pathways and mediators in both the peripheral nervous system and CNS, resulting in heightened responsiveness and sensitivity of itch-processing neurons and refractory itch after lesions have been resolved.18,71
Patients with AD experienced significantly higher itch after exposure to both mechanical and chemical pruritic stimuli (ie, cowhage but not histamine) in lesional and nonlesional skin areas, suggesting a sensitization of nonhistaminergic itch-specific pathways and nonpruritic mechano-sensitive circuitry. 72
Future research is needed to investigate the cross talk between itch mediators, immune cells, and sensory nerves as drivers of neural sensitization in chronic itch.
CENTRAL MECHANISMS OF ITCH IN AD
The CNS (spinal cord, brain) is involved in itch transmission, processing, and scratching response. Neuropathic itch develops in normal skin from excess peripheral firing or dampened central inhibition of itch-associated neurons, but targeted treatments remain limited as the mechanisms are not fully understood. 16 Further studies are needed to elucidate the spinal circuits and supraspinal pathways in relation to chemical and mechanical itch pathways to improve our understanding of the central mechanisms of itch.
Neuroimaging of Brain Neural Networks in Healthy Subjects and Patients With AD
Positron emission tomography and functional magnetic resonance imaging studies have identified changes in brain areas responsible for itch processing that provide some insights into the brain and brainstem circuits involved in itch central perception.71,73,74 It has been suggested that the “itch-processing network” can be divided into three main matrices, respectively, encoding the feeling of itch sensation (location and intensity), affective and motivational aspects of itch, and subjective perception of itch. 75 A meta-analysis on the central mechanisms of itch perception and processing identified several brain regions involved in itch signal transmission and scratching behavior outputs in healthy subjects, including thalamus and the parietal, secondary somatosensory, insular, and cingulate cortices, in particular the precuneus. 73 However, there may be several differences in the itch matrix in patients with chronic pruritus, including patients with AD.73,76 Differences between itch-induced brain activity in healthy individuals and patients with AD have been observed in imaging studies (Table 1) during histamine-induced itch,77-79 cowhage-induced itch, 80 allergen-induced itch,81,82 and contagious itch from watching a video. 83 The main brain areas activated in patients with AD are summarized in Table 1 and Figure 2.
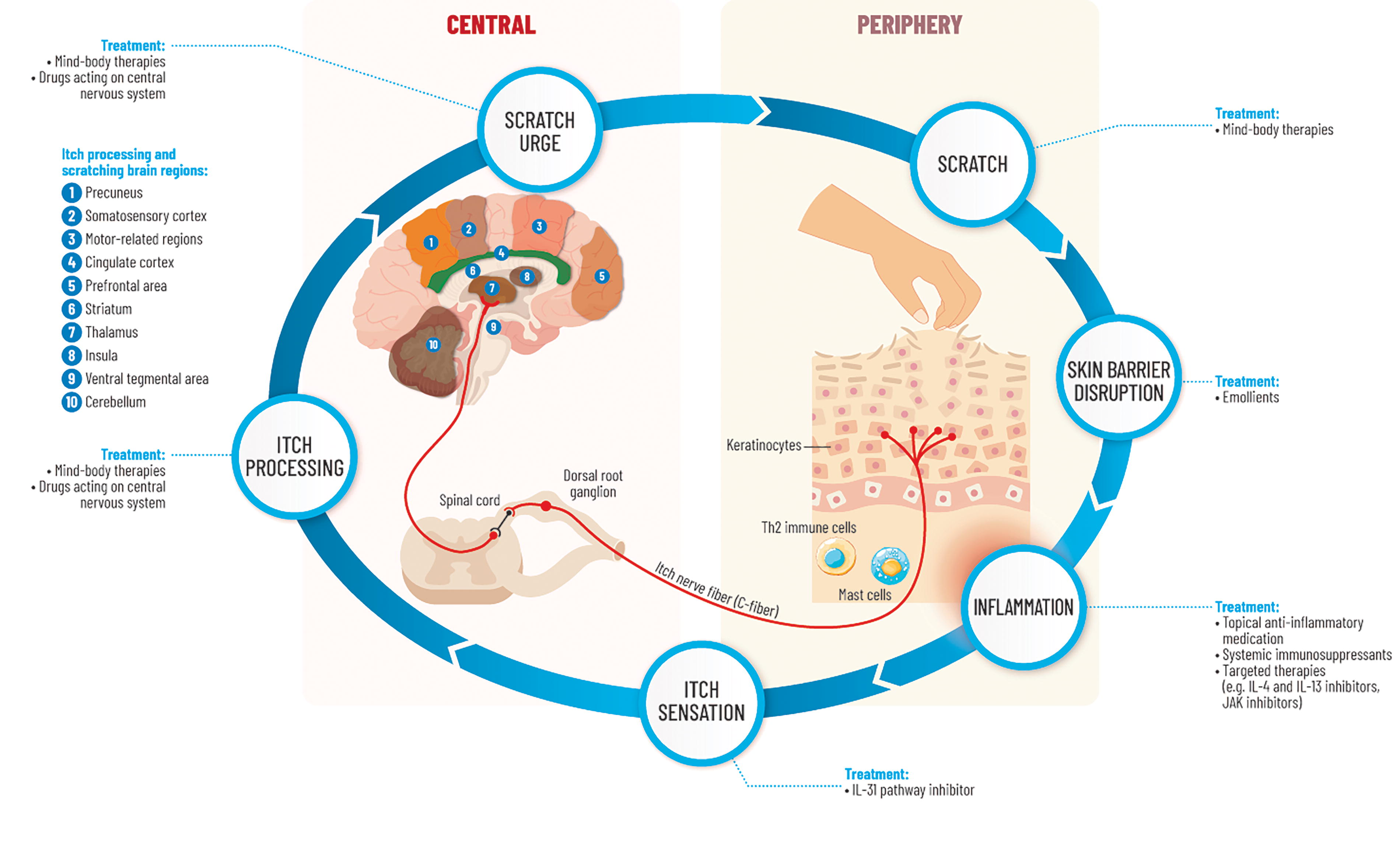
Summary of peripheral and central pathways of the itch–scratch cycle in atopic dermatitis.
Summary of Brain Areas Activated in Healthy Subjects and/or Patients with Atopic Dermatitis During Itching and Scratching
a, anterior; AD, atopic dermatitis; CC, cingulate cortex; dlPFC, dorsolateral prefrontal cortex; dmPFC, medial prefrontal cortex; IC, insula; OFC, orbitofrontal cortex; p, posterior; PFC, prefrontal cortex; SI, primary somatosensory cortex; SII, secondary somatosensory cortex.
Central mechanisms may be involved in the phenomenon of scratching pleasure. In AD subjects, a relationship may exist between alterations in the brain neural network, stress system, and scratching behavior, causing cognitive distortion. 84
Prefrontal Cortex Alterations in Patients With AD
The prefrontal cortex (PFC) integrates information from other brain areas to coordinate responses for self-regulation of behavioral responses, 85 such as scratching behavior and maintaining QoL, well-being, executive functions, and social cognitive responses.84,86 Active chronic itch in patients with AD was found to be associated with an overactivation of the dorsolateral PFC (negatively correlated with perceived itch), with unchanged activity of the somatosensory and motor cortices, potentially having a role in scratching and regulating the itch–scratch cycle.78,84 In AD subjects, sleeplessness due to nocturnal scratching behavior may lead to the activation of the HPA axis and a dampening of dorsolateral PFC regulation of scratching behavior, reward, and habit learning systems. 84 In late phase AD, even when the HPA axis response is blunted, the disruption of the PFC function may maintain itch–scratch cognitive distortion with habitual scratching behavior and skin pathological changes 84 ; this complex process in patients with AD is represented in Figure 1 showing the interrelated itch–scratch cycle and bidirectional scratch–sleep cycle with cognitive distortion from the additional negative effects of sleep disturbance and psychological stress. A positive correlation has been observed between AD severity (Eczema Area and Severity Index score) and activations of the anterior cingulate cortex and dorsolateral PFC.78,87 Persistent hyperactivation of the dorsolateral PFC when regulating the itch–scratch circuit may disrupt this brain region in patients with AD. Since scratching behavior activates the dopaminergic reward and habit learning systems, the dorsolateral PFC may also eventually fail to regulate these systems, resulting in the reinforcement of “uncontrollable” habitual scratching behavior in patients with AD.
Itch–Scratch Cycle and Dopaminergic Pathways
While scratching relieves itch in healthy subjects, the itch does not subside in patients with AD even after repeated scratching as it becomes a compulsive, almost obsessional, habit.88,89 Interestingly, there is an overlap in brain regions, such as midbrain reward systems, involved in addiction, stress-induced depression, and itch–scratch behavior.62,90 Understanding shared common mechanisms between addiction and scratching behavior, and alterations in central neural circuits, may help identify potential therapeutic targets for preventing scratching. 90
Brain imaging studies in healthy and chronic itch patients found that scratching activated brain regions involved in the reward system (ie, striatum, ventral tegmental area).91,92 Higher activity during scratching in chronic itch patients was noted in brain regions related to motor control and the motivation and reward system (orbitofrontal cortex, caudate nucleus), providing a potential explanation for the urge to scratch. 80
In patients with intense and chronic itch, related to inflammation and lesions in the skin, activation of the habit and reward-related areas induced by scratching was significantly increased. 62 This increased activation in patients with AD could be due to the itch–scratch cycle reinforcing persistent scratching behavior. 73 This overactivation may be responsible for the impulsive dimension of scratching behavior that becomes obsessional. 84 Some patients with AD continue scratching despite showing clinical improvements from receiving treatment for inflammation, possibly because it is not directed at relieving itch, and that scratching (even without stimulation) has become a compulsive habit. As regular stimulation of dopaminergic systems can reinforce scratching behavior, controlling activation of this system might be a therapeutic target for itch, or reinforcement of this behavior could be limited by a behavioral approach. 71 Finally, although studies have been carried out in animal models,93-95 the central molecular circuits remain poorly understood and require further investigation.
THERAPIES FOR THE ITCH–SCRATCH CYCLE IN AD
Due to the complexity of the pathophysiology of chronic itch in AD, involving different neural and immune mechanisms, finding effective pharmacological solutions to treat all aspects of the itch–scratch cycle to improve patient well-being remains challenging.
Pharmacological Therapies
Conventional basic therapy with moisturizers and emollients (or emollient “plus” containing additional active, nonmedicated substances) can help to restore and maintain the skin barrier function.96,97 In addition, corticosteroid treatment or calcineurin inhibitors, topical anti-inflammatory therapy, is a mainstay for basic AD treatment and should be used regularly (and as a proactive maintenance therapy 98 ).99,100
Improved understanding of classical biochemical and neurophysiological peripheral itch mechanisms of the itch–scratch cycle, neuroimmune circuits, and neuronal signaling has led to the development of new and emerging therapeutic strategies for AD.1,101 Newer topical or systemic treatments may be required for persistent pruritus,102,103 depending on severity.97,104-106
Emerging topical treatments for controlling itching include topical therapeutic aryl hydrocarbon receptor modulating agent, for example, tapinarof 107 ; phosphodiesterase 4 inhibitors, for example, roflumilast, 108 difamilast 109 ; topical Janus kinase (JAK) inhibitors, for example, ruxolitinib, a potent, selective inhibitor of JAK1 and JAK2, 110 delgocitinib 111 ; brepocitinib, a tyrosine kinase 2/JAK1 inhibitor 112 ; or other topical treatments, for example, transient receptor potential vanilloid 1 antagonist. 113
An ever-increasing number of approved biological therapies aimed at treating dysregulated type-2 immunity have shown improvements in inflammation, skin barrier function, and pruritus in patients with AD by targeting, for example, IL-4, IL-13, or IL-31 receptor-A105,114 (eg, dupilumab, tralokinumab, nemolizumab).35,115 Other targeted therapies are in development for treating AD and pruritus, including agents targeting the OX40 receptor, 116 IL-1a, TSLP, or Oncostatin M (OSM).1,36,71,117,118 Moreover, JAK inhibitors, such as abrocitinib, 119 baricitinib, 120 or upadacitinib, 121 were beneficial on inflammation and skin barrier function and improved pruritus and scratching. 102
The treatment of central itch is still very limited (eg, neuroleptics). As chronic itch is associated with increased stress, treatments that reduce anxiety may have an antipruritic effect.
122
Furthermore, specific brain structures are associated with stress so pharmacological treatments targeting neuronal pathways may help to modulate itch.
123
Treatments for neural sensitization include GABAergic drugs, kappa opioids, immunomodulatory therapies, and N-methyl-
The Importance of Integrative Treatment Approaches for AD Itch Treatment
Despite the ever-increasing number of pharmacological therapies, including biologics, they are unable to address all the aspects of the itch–scratch cycle to achieve complete resolution of AD in all patients. 118 Indeed, clinical studies show that scratching behavior may continue in as many as half of moderate-to-severe patients with AD receiving targeted biological therapies,121,129 suggesting other factors are playing an additional role in the itch–scratch cycle. 36 Multidisciplinary or personalized therapeutic approaches may be required due to the complex heterogeneity of AD. 130 Therefore, in the future, targeted AD therapies may be combined with appropriate pharmacological or psychological treatments in the case of an accompanying or underlying psychological/psychosomatic disease or sleep disturbances for a better patient outcome.1,87,103,131
Furthermore, research on the central molecular mediators, receptors, and pathways is necessary to develop centrally targeted therapies for pruritus, as the currently available pharmacological therapies are limited and may be associated with mild-to-severe side effects.
Integrative, individualized, and multidisciplinary treatment approaches that emphasize the psychosomatic component of AD by combining psychological techniques and modifying standard treatments to improve mental, physical, and emotional health may thus be required to treat the psychological aspect of itch and habitual scratching behavior. 132
The interplay between itch–scratching and sleep disturbances and psychological stress is well recognized (see Fig. 1) and can further aggravate AD and have a significant impact on QoL. 59 Management of chronic pruritus associated with its psychosomatic components in patients with AD is directed at treating the behavioral abnormalities through improving patients’ psychological health. 133 The strong connection between mind and body in the itch–scratch cycle, and the central mechanisms involved, suggests integrative treatment approaches could be helpful as an adjunct to pharmacological treatment in the clinical management of AD (see Fig. 2), especially as many holistic therapies are generally noninvasive and safe. 132
Benefits of Holistic Therapies for AD
A recent focused literature review found a paucity of rigorously designed trials evaluating holistic therapies for AD. 132 Interventions (eg, therapeutic patient education, cognitive behavioral therapy [CBT], habit reversal [HR], meditation, mindfulness, hypnotherapy, biofeedback, progressive muscle relaxation, music therapy, massage) were not always clearly defined in the various studies, and some were evaluated as adjuncts to conventional treatments. However, the overall body of evidence appears to suggest that integrative treatment approaches may provide some potential benefits on pruritus, pain, psychological stress, anxiety, depressive symptoms, and sleep quality. 132
AD guidelines recommend psychological and educational programs, which have proven efficacy in children and adults and improve treatment adherence. 97 CBT such as individual patient education, awareness training, HR, relaxation exercises, and psychosocial support have been widely used in the management of AD with positive effects on itch relief.134-136 CBT with HR therapy to replace a harmful behavior of scratching with a better alternative (eg, the application of emollients or topical corticosteroids, rubbing instead of scratching) may be beneficial in patients with AD to reduce scratching and ameliorate the vicious itch–scratch cycle, as well as reduce skin lesions and improve treatment adherence.
Catastrophizing about itch in patients with AD increases itch intensity and could be treated by psychological interventions with mindfulness to increase acting with awareness. 137 Patients with AD experienced higher itch intensity and scratched more frequently when watching itch videos of mock itch stimuli,83,138,139 which suggests that it should be possible to influence itch and its perception for patients using holistic therapies. Verbal instructions may also modulate itch. Placebo effects are associated with brain regions involved in planning and emotions and can be evoked by outcome expectations, while nocebo effects are associated with brain regions involved in somatosensory itch processing related to the itch–scratch cycle and contagious itch. 140
The finding that noninvasive brain stimulation interventions, such as transcranial direct current stimulation, could reduce itch suggests that the brain is an important target for the treatment of itch in AD. 141 Another review on the potential alteration of brain mechanisms of itch in patients with AD suggested that noninvasive treatments, such as psychological interventions and transcranial direct current stimulation, could target itch-related central pathways to help reduce itching, 87 thereby improving well-being and QoL. Since studies have shown functional and structural changes in the brain after integrative therapies, such as CBT and mindfulness, it has been suggested that they may “rewire” dysfunctional brain networks in chronic itch. 81
The use of new technologies may lead to the development of novel nonpharmacological integrative interventions. For example, initial results of a small study in 10 patients with mild AD showed that closed-loop haptic feedback on an artificial intelligence-enabled wearable sensor may decrease nocturnal scratching. 142 Finally, future studies with functional neuroimaging may be useful for monitoring therapy effects to help choose the optimal therapy for the central mechanism of intractable itch.
CONCLUSIONS
Understanding the complex pathophysiology of chronic itch in AD, which involves immunological, cutaneous structural, and neurological mechanisms, is essential to develop optimal strategies to break the itch–scratch cycle for long-term disease control. Recent promising data indicate that disease modification may be achievable with the new targeted therapies. Nevertheless, existing pharmacological therapies for treating pruritus are unable to control the disease over the long term in absolute terms to completely alleviate itching in all patients with AD. Therefore, integrative therapies could be useful adjuncts in many patients with AD for treating the central aspect of scratching (and the underlying psychological issues) to break the vicious cycle, thus improving outcomes with a good benefit/risk ratio. Additionally, pharmacological treatments that target the CNS may have side effects, while noninvasive holistic approaches and psychological interventions may be safer alternatives to stop the scratching behavior. Integrative holistic therapies, for example, education, CBT and HR, in addition to emollient or emollient “plus” basic therapy, antipruritic agents, and conventional or targeted pharmacological treatments, may help to relieve pruritus and decrease scratching behavior, reduce stress and sleep disturbances, and improve well-being in patients with AD. Future perspectives include the use of precision medicine-based approaches to help identify heterogeneous phenotypes and endotypes with neuroimmune dysregulation and their pathways, as additional therapeutic targets for optimal AD treatment.