
Abstract
Background:
Two regimens are used to achieve excellent glycemic control during pregnancy in type 1 diabetes mellitus (T1DM): continuous subcutaneous insulin infusion (CSII) and multiple daily injections (MDI). We assessed their efficacy and safety and the effect of pregnancy planning.
Methods:
We examined 269 pregnant T1DM women: 157 treated with MDI (MDI group), 42 with CSII (CSII group), and 70 who switched from MDI to CSII in the first trimester (MDI/CSII group). There were 116 women who planned pregnancy: 58 in the MDI group, 38 in the CSII group, and 20 in the MDI/CSII group. The estimated differences in glycemic control and maternal and fetal outcomes were adjusted for baseline characteristics.
Results:
Mean glycated A1c (HbA1c) in the first trimester in the whole group was 6.9%, and the women differed depending on whether they planned pregnancy or not (P < 0.0001). A multiple regression model showed an average difference of about 0.9% in favor of pregnancy planning, with no interaction between the planning and treatments. In the second trimester, HbA1c decreased to a mean value of 5.8%, with improvement of HbA1c across all treatments: by 1.5% in not-planning and 0.9% in planning women. Despite greater improvement, not-planning women still had a higher HbA1c (by 0.3%, P = 0.05). In the third trimester, there was no further significant changes; nevertheless, women who planned pregnancy still had a lower HbA1c (by 0.5%, P = 0.02). There were 14 malformations, stillbirths, and perinatal infant deaths in the not-planning versus five in the planning group (P = 0.07). Patients in the CSII group had a 2 kg greater weight gain compared to the MDI group (15.0 kg vs. 13.0 kg; P = 0.005).
Conclusions:
In pregnancy with T1DM, both MDI and CSII can provide excellent glycemic control. Pregnancy planning has a beneficial effect on glycemic control, independent from the therapy model. CSII seems to predispose to a larger weight gain in mothers.
Introduction
Achieving normoglycemia in T1DM women before conception and during pregnancy has been proven to reduce maternal and neonatal adverse outcomes. Two insulin regimens are commonly used: multiple daily injections (MDI) and continuous subcutaneous insulin infusion (CSII) with a personal insulin pump. The application of the CSII method in patients with diabetes has gradually gained popularity, and the frequency of its use has steadily increased, especially among children and adolescents. CSII seems to be a more physiological way of delivering insulin, and it may better mimic both basal and mealtime insulin production. Furthermore, it provides more flexibility and freedom in composing diet and meal planning. Numerous clinical studies on T1DM patients have demonstrated effectiveness of CSII in attaining normalization of glycemia and the lowering of glycated hemoglobin (HbA1c) levels with no increase in risk of serious hypoglycemia events and episodes of ketoacidosis. 14 –17 Systematic reviews demonstrated a possible advantage of CSII over MDI in achieving normoglycemia in T1DM. 18,19 Clinical studies have proven that pump therapy was especially effective in persons with unstable diabetes, dawn phenomenon, hypoglycemia unawareness, and small daily insulin requirement or in those who lead an irregular lifestyle. 20 –22 However, data on CSII use in T1DM during pregnancy are scarce. For example, the recent Cochrane systematic review was only able to identify two randomized studies, both outdated, for the meta-analysis of pregnancy outcomes in women with pregestational diabetes using CSII and MDI. 23 The two studies were performed many years ago and thus are of limited value to today's clinical practice. The number of observational studies is also limited, and their study sample size are too small to conclusively investigate the efficacy of CSII therapy during pregnancy. 24 –30 Thus, there is a need for more data on the use of modern insulin pumps in pregnant women with T1DM.
Here, we present the results of an observational study that aimed to assess efficacy and safety of CSII and MDI as well as the effect of pregnancy planning in pregnant women with T1DM.
Subjects and Methods
Patients
Over the period 2000–2008, there were 287 pregnant women with T1DM who were treated in the Department of Metabolic Disease, Jagiellonian University Medical College, Krakow, Poland. Women with T1DM, who were pregnant or planned pregnancy, received an intensive diabetes management that involved education, frequent outpatient visits, and hospitalizations, if necessary, with the following therapeutic targets: (1) HbA1c <6.1%, (2) fasting self-monitored blood glucose within 60–90 mg/dL, and (3) subsequent pre- and postprandial glucose self-measurements within 60–120 mg/dL. In this study, we included all patients who met the following criteria: (1) clinical diagnosis of T1DM established at least 1 year prior to conception, (2) medical care in the Department initiated not later than in the first trimester of gestation, and (3) complete follow-up until delivery. As not all study participants were followed from before conception, we excluded the patients who miscarried, to avoid selection bias. Overall, 269 women with T1DM enrolled in the study; they all were Caucasians and residents of Southeastern Poland. None of the patients from the current report was included in earlier reports from the Polish population. More than half of the patients were treated with the MDI regimen (n = 157, 58.4%) through the whole period of gestation (MDI group), predominantly with human prandial insulin (n = 151, 96.2%). There were 18 subjects that had their own personal pumps. They continued the CSII regimen throughout pregnancy. Additionally, in the Department there were insulin pumps available for rent to T1DM pregnant women or T1DM women who planned pregnancy. There were 24 patients who received a pump from the clinic prior to conception. Therefore, there were 42 women that were treated exclusively with CSII (CSII group); 17 (40.5%) of them used human insulin, whereas the others were treated with analogs. Seventy women (CSII/MDI group) switched from MDI to an insulin pump and initiated CSII therapy in the course of the first trimester of gestation (median week of gestation, 9.0). Among them there were 67 who rented a pump and three who initiated therapy using their own instrument. Selection of treatment regimen and time of CSII initiation depended on the availability of pumps, patients' preference, physicians' discretion, and an evaluation of subjects' ability to properly use personal pumps, which was carried out by a trained educator when the CSII option was considered. The indications for the switch from MDI to CSII in the first trimester included, for example, the lack of compensation of diabetes and long disease duration that might predict difficulties in achieving glycemic control; however, transfers to CSII were also influenced by pump availability. The proportion of women treated with human insulin in their pumps was similar in both the CSII and CSII/MDI groups (n = 29, 41.4% in CSII/MDI). There were 116 women (43.1%), who started intensive diabetes management prior to conception (“pregnancy planning”): 58 (36.9%) in the MDI group, 38 (90.5%) in the CSII group, and 20 (28.6%) in the group of women transferred from MDI to CSII in the first trimester (MDI/CSII group). The other 153 women entered the intensive diabetes management program in the first trimester. Therefore the terms “pregnancy planning,” “planned,” and “unplanned” used in this article refer to time of entry to our intensive care program. Figure 1 shows the numbers of patients in all study groups, based on the treatment method and pregnancy planning.
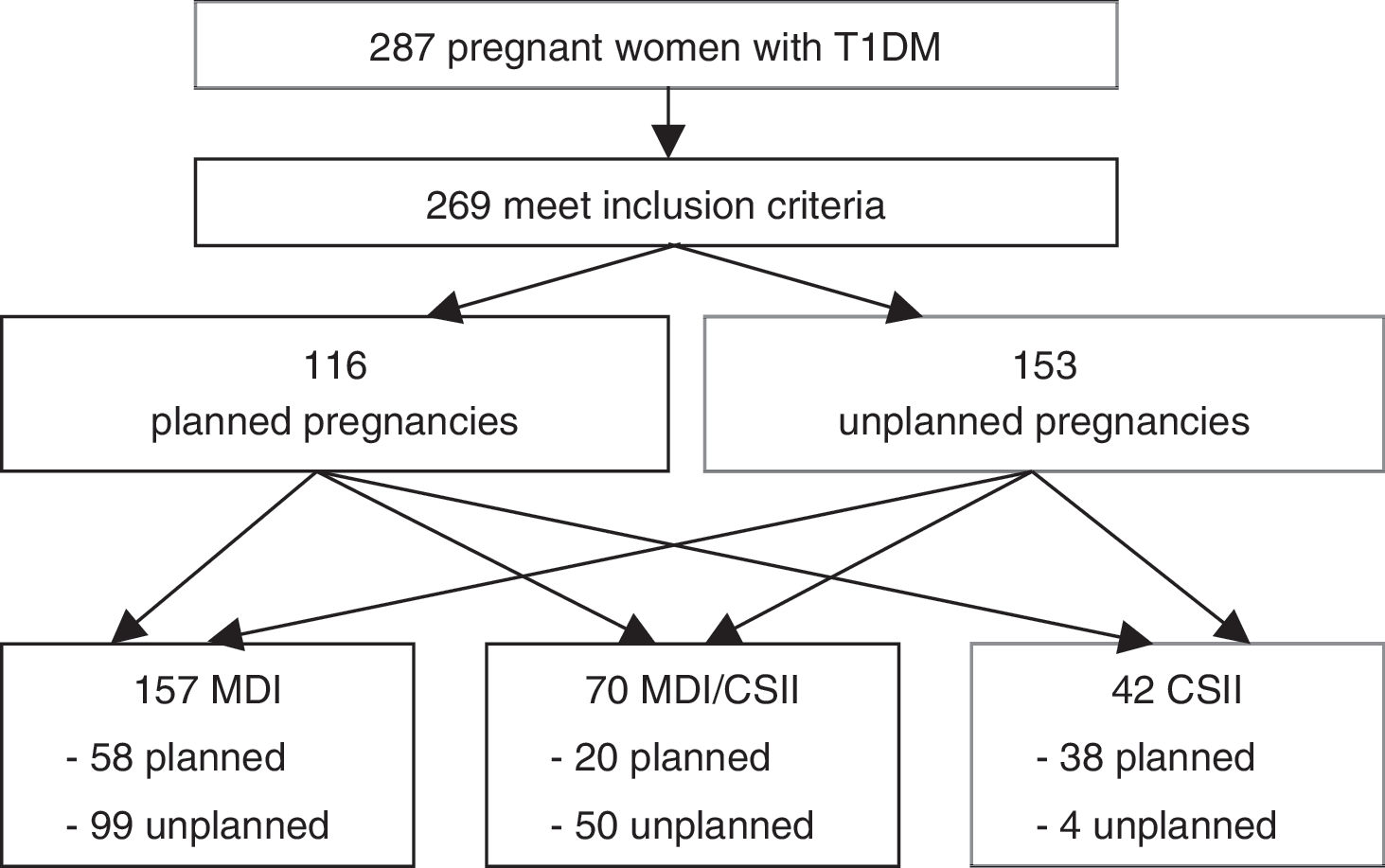
Number of patients enrolled in the study and stratification by treatment modality and pregnancy planning.
All women received a thorough education covering self-monitoring of blood glucose, glycemic targets, diet, and self-adjustment of insulin doses. Recommended daily caloric intake included 40–50% carbohydrates, 20–30% fats, and 30% proteins. Standard calorie intake was 35 kcal/kg of body weight. Excessive weight gain was addressed with reducing daily food intake accompanied by a regular daily self-assessment of urine ketones. 31 The subjects treated with CSII received additional instructions regarding pump usage. All patients received additional individual education, if necessary.
Baseline characteristics
The baseline characteristics were assessed during the initial visit and included patients' age, duration of diabetes, weight before conception, body mass index (BMI), and presence of diabetes complications. Retinopathy was diagnosed ophthalmoscopically, while diagnosis of nephropathy was based on the albumin excretion rate (with values between 30 and 300 mg/24 h classified as albuminuria).
Outcomes
We analyzed the following study outcomes: mean HbA1c through the first, second, and third trimesters of pregnancy, mean daily insulin dose in the first, second, and third trimesters, mean mothers' weight gain during gestation (based on weight before pregnancy and the last weight measured within a week before delivery), number of episodes of severe hypoglycemia (defined as requirement of assistance from another person) and diabetic ketoacidosis (DKA) (documented by an arterial pH <7.30), frequency of caesarean deliveries, frequency of preterm births (<37th week), mean children's birth weight and frequency of macrosomia in full-term pregnancies (>4,000 g), and frequency of combined stillbirths, hospital infant deaths, and malformations. Multiple pregnancies (n = 7; two in the MDI group, one in the CSII group, and four in the MDI/CSII group) were excluded from analysis of cesarean sections, macrosomia, preterm deliveries, and birth weight.
Statistical analysis
Baseline characteristics were compared with two-way analysis of variance for quantitative traits or χ 2 test for categorical data. Logarithmic transformations were carried out to meet normality assumption (for weight gain and birth weight). To test the impact of treatment modality or pregnancy planning on the study outcomes, linear or logistic models were used, with age, age at diagnosis of diabetes, and BMI as covariates. To compare changes in HbA1c and insulin dose over time, a linear mixed model was applied with the same covariates as above. All computations were performed with SAS version 9.2 software (SAS, Cary, NC). Values of P < 0.05 were considered significant.
Results
Baseline clinical characteristics of the study groups are presented in Table 1. In brief, we did not find significant differences in subjects' age and frequency of microvascular complications of diabetes. There were significant differences in duration of diabetes and BMI between strata formed by treatment group and planning factors (Table 1).
For the given number of individuals, the percentages refer to the whole study population (n = 269), and the P value was obtained from χ 2 test of association between pregnancy planning and treatment group assignment (significant at P < 0.0001).
Significant difference in duration between planning and not-planning women in MDI stratum (P = 0.01).
Significant difference in BMI between planning and not-planning women in MDI stratum (P = 0.0007).
Significant differences in HbA1c between planning and not-planning women in all treatment groups (P < 0.0001).
Significant differences in insulin dose between CSII versus both MDI and MDI/CSII (P < 0.0001).
In frequency/n (%). Percentages refer to proportions within subgroups (treatment × planning).
Mean baseline HbA1c in the first trimester in the whole group was 6.9%. The women differed significantly by HbA1c in the first trimester (Table 1 and Fig. 2) depending on whether they planned pregnancy and entered the intensive treatment program prior to conception or not (P < 0.0001). A multiple regression model showed an average difference of about 0.9% in favor of pregnancy planning, with no significant interaction between planning and treatment group. Adjusted for planning and covariates (age, duration of diabetes, and BMI), there was no significant difference in HbA1c between the treatment groups. Further HbA1c changes are shown in Figure 2. In brief, in the second trimester, HbA1c decreased in all groups and reached a mean value of 5.8%. Across the three treatment groups there was similar significant improvement of HbA1c as compared to baseline value: by 1.5% in not-planning and 0.9% in planning women (P < 0.0001). The difference in improvement between planning and not-planning patients (0.6% in favor of not-planning) was also statistically significant (P = 0.017). In the second trimester, the mean HbA1c in the MDI group reached 5.7% in planning and 6.0% in not-planning women, in the MDI/CSII group it was 5.5% in planning and 5.9% in not-planning women, and in the CSII group it was 5.6% versus 5.8%, respectively. Despite greater improvement, not-planning women still had a significantly higher HbA1c level in the second trimester (by 0.3%, P = 0.05). In the third trimester there was no further significant changes in HbA1c level, compared to the second trimester. Mean HbA1c was 5.8%, significantly less than in the first trimester (P < 0.0001). Women who planned pregnancy had a significantly lower HbA1c level in the third trimester than not-planning women (by 0.5%, P = 0.02). The mean HbA1c in the MDI group was 5.6% in planning and 5.9% in not-planning women, in the MDI/CSII group it was 5.5% in planning and 5.7% in not-planning women, and in the CSII group it was 5.5% versus 6.6%, respectively. The substantial and unexpected rise of HbA1c in the third trimester that occurred in not-planning CSII patients was not statistically significant, as this stratum comprised only four patients.

Mean HbA1c level in MDI (squares), CSII (circles), and MDI/CSII (diamonds) treatment groups stratified by pregnancy planning (solid lines connect values in planning strata, and dashed lines connect values in not-planning strata).
Insulin dose increased significantly over the course of pregnancy (P < 0.0001). The mean insulin dose in the first trimester was 47.6 U, in the second 55.4 U, and in the third 79.9 U. The lowest insulin dose in the first trimester was observed in the CSII group (41.9 U), which was significantly lower than in the MDI and MDI/CSII groups (49.2 U [P = 0.02] and 48.5 U [P = 0.02], respectively). In the second trimester, insulin doses rose to 55.9 U, 57.2 U, and 51.1 U in the CSII, MDI and MDI/CSII groups, respectively. In the third trimester, the doses were 79.4 U, 81.4 U, and 77.4 U, respectively. Contrasts between the first and second trimesters were significant at P < 0.0001 in MDI and CSII study groups, whereas in the MDI/CSII group, insulin dose in the second trimester did not change significantly (P = 0.3) from the first trimester. There were no significant differences in insulin dose between the study groups in the second trimester (P = 0.06 for MDI vs. MDI/CSII) and, similarly, in the third trimester. Pregnancy planning did not have an impact on insulin dose.
Mean weight gain during pregnancy was 13.9 kg in the whole study cohort. The largest weight gain was observed in both CSII-treated groups (15.2 kg in the MDI/CSII group and 14.7 kg in the CSII group, compared to 13.0 kg in the MDI group). Patients treated with CSII (both CSII and MDI/CSII groups) had, on average, a 2 kg greater weight gain compared to MDI (15.0 kg vs. 13.0 kg), and this difference was statistically significant in a multiple regression model (P = 0.005). Pregnancy planning did not significantly modify this outcome.
Cesarean sections were more frequent in CSII users, from both CSII and MDI/CSII groups combined (64.9% vs. 86.7%, P = 0.008) and in pregnancy planners (62.8% vs. 75.5%, P = 0.03). These differences were explained by differences in age, duration of diabetes, and presence of microvascular complications; thus multiple logistic regression analysis did not yield significant results. We did not observe significant differences in preterm labors, either between the treatments (22.9% vs. 28.6% vs. 17.1% in MDI, CSII, and MDI/CSII, respectively; P = 0.3), or attributable to pregnancy planning (18.9% vs. 26.7%, planning vs. no planning, respectively; P = 0.13). There were no significant differences in birth weights across the strata (mean 3,571 g, excluding multiple pregnancies and preterm deliveries) and no different proportions of macrosomic births (18.1% in the whole cohort in full-term pregnancies).
Study subjects reported 13 episodes of severe hypoglycemia that occurred during pregnancy: five (11.9%) in the CSII group, two (2.9%) in the MDI/CSII group, and six (3.8%) in the MDI group, respectively. Both incidents of severe hypoglycemia in the MDI/CSII group occurred during MDI before the transfer to CSII. The difference between CSII- and MDI-treated patients was significant (P = 0.04). In addition, there were six episodes of DKA during pregnancy in the entire cohort: two (4.8%) episodes in the CSII group, one in the MDI group (0.6%), and three (4.3%) in the MDI/CSII group, respectively. All three episodes of DKA in the MDI/CSII group occurred before the therapy switch and constituted a direct indication for CSII implementation. The difference of DKA frequency in MDI- versus CSII-treated patients (P = 0.2) was not significant (by Fisher's exact test). Pregnancy planning did not have a significant impact on severe hypoglycemia or DKA frequency.
There were 19 malformations and/or stillbirths and deaths (16 and seven, respectively) in the study cohort: 13 in the MDI group, one in the CSII group, and five in the MDI/CSII group. The study was underpowered to detect any differences in proportions of these outcomes across treatments. There were 14 malformations and stillbirths combined in the group of women that did not plan pregnancy (10.7%) and 5 (4.5%) in the planned pregnancy group. This difference reached a borderline significance (P = 0.07).
We did not observe any impact of short-acting insulin type (human vs. rapid-acting analog) on any of the study outcomes.
Discussion
This observational study demonstrated that both MDI and insulin pump therapy may ensure good glycemic control in T1DM women during pregnancy. So far, there were several observational articles published that evaluated the CSII model and the MDI regimen in pregnant T1DM women. 24 –29 A small randomized controlled trial was also published. 32 The current study was the largest one; the number of our patients on the CSII model was over three times higher than the largest previously published. 27 As in the other studies, the highest values of HbA1c were observed in all three groups in the first trimester of pregnancy. Our patients achieved a substantially better HbA1c level in the second and third trimesters, compared to most other studies, 23 –29 and they reached therapeutic HbA1c targets. Comparable results were reported only in one matched cohort study. 25
Regardless of the treatment strategy, the purpose of intensive insulin therapy in T1DM during the pregnancy planning and after conception is to achieve the target level of normoglycemia. 33,34 The task of achieving therapeutic goals was generally accomplished in the second and the third trimesters in all three groups, CSII, MDI/CSII, and MDI, as indicated by HbA1c level, but it should be pointed out that those levels were still higher than levels observed in pregnant women without diabetes. 35 Data from observational and intervention studies clearly demonstrated that infants born to women with tight glycemic control had fewer congenital malformations than those whose mothers did not reach desired therapeutic goals. 36,37 In our study, neither therapy was better than the others in terms of glycemic control, as measured by HbA1c. Thus, it is not surprising that we observed a lack of significant differences between the treatments in the fetal outcomes. An additional factor that might have contributed to this observation was excellent glycemic control achieved by our patients. Despite a large number of study participants, there were not enough adverse outcomes attributable to insufficient diabetes management to carry out statistically meaningful comparisons. Unlike in previously published reports, we took into account pregnancy planning in our analysis. Our data clearly demonstrate that pregnancy planning allows the patient to enter gestation with substantially better HbA1c in the first trimester in all treatment groups. This effect was sustained in the second and third trimesters, indicating that pregnancy planning has a beneficial effect on glycemic control, not only in early pregnancy, but throughout the whole period of gestation. The proportion of stillbirths and malformations in infants was also associated with pregnancy planning, achieving borderline significance. This additionally supports our finding and shows a great importance of pregnancy planning in all T1DM patients.
In addition, we observed that all women treated by CSII (both CSII and MDI/CSII groups) gained more weight during the pregnancy. Changes in mean daily insulin doses may partially explain this phenomenon, as the rise in insulin requirement was largest in the CSII group. A possible mechanism of increased weight gain on CSII may be larger dietary freedom and flexibility on insulin pumps, a phenomenon that was previously described. 30 This seems to underline the necessity of intensive and repeated dietary trainings in subjects on CSII. In CSII-treated patients we observed a greater risk of severe hypoglycemic episodes than in MDI-treated subjects; this difference reached a weak statistical significance. The proportion of caesarean sections was larger in women using insulin pumps. In multiple logistic regression this was explained, however, by several clinical factors such as age, duration of diabetes, and presence of microvascular complications. In general, the frequency of cesarean section was very high in all the groups, which is in agreement with earlier articles. 9,38
There are a few shortcomings in our study. The major limitation, as in previous observational reports, was the lack of randomization in assigning patients to MDI or CSII treatment. It is well known that observational studies are prone to many biases. In our study, we addressed many possible sources of confounding bias, such as unequal proportion of planned pregnancies and differences in duration of diabetes or BMI. However, several factors that were difficult to control likely influenced assignment to CSII in our cohort. For example, the patients with unsatisfactory glycemia on MDI and those with longer duration of diabetes were more likely to receive an insulin pump, as a result of an attending physician's decision. A failure to achieve therapeutic goals with MDI, as an indication to switch to CSII, could bias towards the null value possible beneficial effect of the CSII suggested earlier in the non-pregnant T1DM population. 18 Certain aspects of the medical care for pregnant women with T1DM are specific to Poland and might influence the therapeutic strategies in these patients. There are a few centers in our country, mostly academic, that provide insulin pumps for T1DM women who are either pregnant or plan pregnancy. In addition, some future mothers acquire pumps individually; this however, is not covered by the public health insurance system. The CSII supplies are reimbursed only for pregnant women. In addition, we were able to examine only some maternal and neonatal outcomes, as, for example, data on the frequency of hypoglycemia in children were lacking. Because of the lack of an appropriate standard, we were unable to report proportion of births that were large for gestational age. It should also be noted that most patients on the MDI regimen were using human insulins rather than rapid-acting analogs. We did not find any association between insulin type and outcomes; therefore, it is unlikely a source of confounding.
To summarize, in pregnant women with T1DM, both MDI and CSII models can provide excellent glycemic control. Pregnancy planning has a beneficial effect on glycemic control, independent from therapy model, and may improve pregnancy outcomes. CSII seems to predispose to a larger weight gain in mothers, probably due to greater dietary freedom in patients on insulin pumps.
Footnotes
Acknowledgments
This work was supported by the Polish Ministry of Science grant N N407 414436. The authors would like to express their gratefulness to The Great Orchestra of Christmas Charity, a non-governmental aid organization in Poland that provided insulin pumps to most women included in this study.
Author Disclosure Statement
No competing financial interests exist.