
Abstract
Background:
Skin autofluorescence (AF) as measured with the AGE Reader (DiagnOptics Technologies, Groningen, The Netherlands) is a noninvasive prognostic marker in diabetes mellitus and other diseases with increased cardiovascular risk. This study provides reference values of healthy Caucasian control subjects as a function of age, tobacco smoking, and gender.
Methods:
The results of skin AF measured in 428 healthy Caucasian control subjects by the AGE Reader (n = 211) and its nonautomated but otherwise similar predecessor, the Autofluorescence Reader (n = 217), were analyzed. Linear regression analysis was performed to obtain reference values for skin AF as a function of age. Further analysis was performed on the effect of tobacco smoking (n = 96) and gender.
Results:
Skin AF was described by a linear increase with age of approximately 0.023 arbitrary units (AU) per year for subject age up to 70 years. Tobacco smoking was associated with an absolute increase of skin AF by 0.16 AU (P < 0.01), without a significant further increase with age (P = 0.17). Gender had no influence on skin AF in nonsmokers. Among current smokers, female subjects had a 0.2 AU higher skin AF than male subjects (P = 0.02), with no further age-related increase.
Conclusions:
The present results provide reference values of skin AF for healthy Caucasian control subjects over a broad age range. A major contribution of age and some interaction of smoking and gender were observed, resulting in reference values of skin AF suitable for clinical settings and future studies.
Introduction
The aim of the present study was to provide reference values of skin AF for control subjects over a broader age range. Furthermore, the effects of age, tobacco use, and gender have been investigated.
Subjects and Methods
Instrumentation
The skin AF results were obtained with the AFR and the AGE Reader. The AGE Reader is a fully automated version of the AFR with an built-in spectrometer. In both instruments (AFR and AGE Reader) the excitation light source is a similar ultraviolet-A blacklight tube, with a peak wavelength of 370 nm, which illuminates ∼4 cm2 of the skin on the volar side of the forearm. A noncontact optical fiber detects the emission and reflected excitation light at an angle of 45°. Using a spectrometer and computer software, the intensity spectrum, of which a typical example is shown in Figure 1, is analyzed. Skin AF is calculated as the ratio between the total emission intensity (420–600 nm) and the total excitation intensity (300–420 nm), multiplied by 100, and is expressed in arbitrary units (AU).
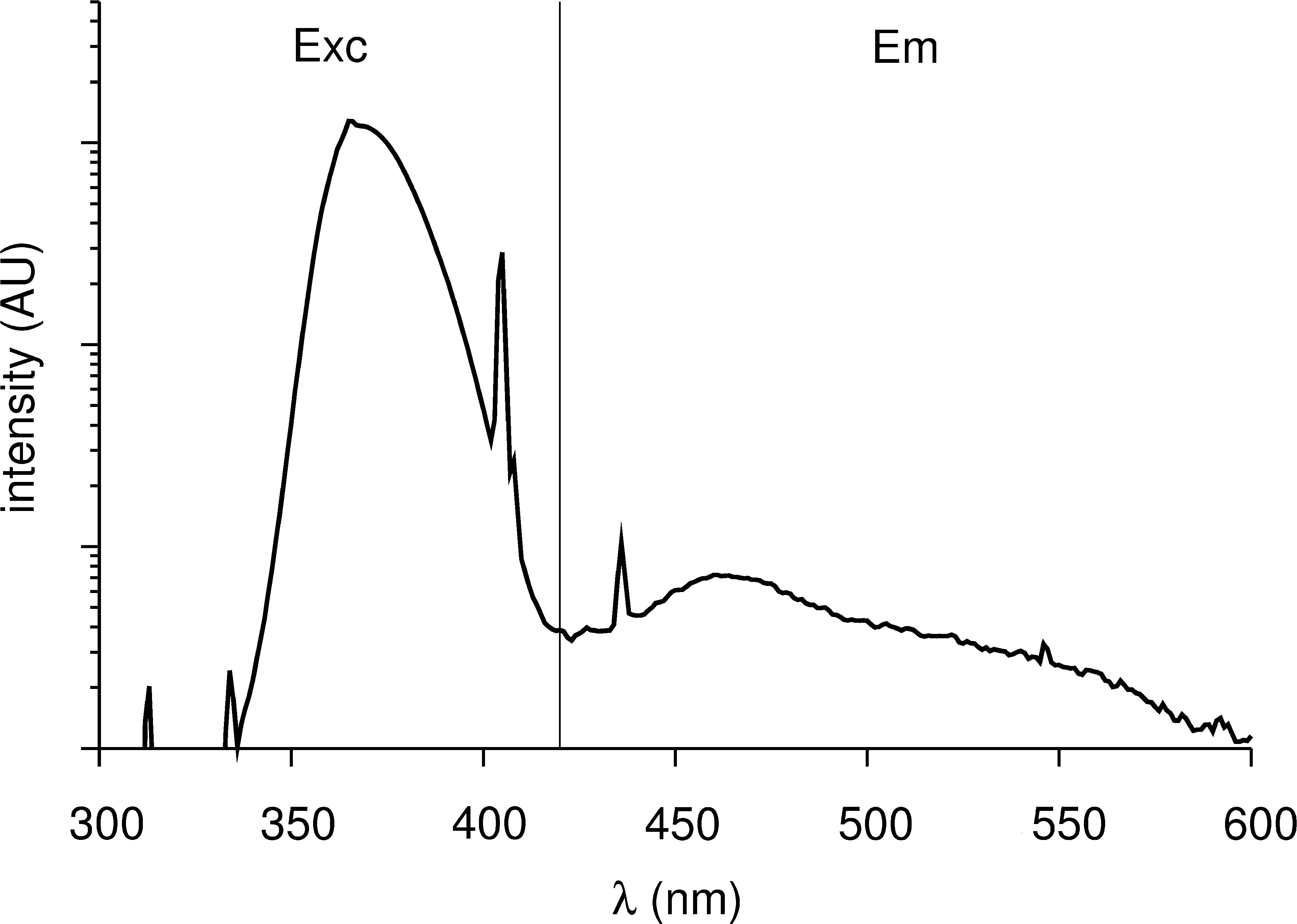
Typical example of an intensity spectrum as detected from the skin. Exc is the excitation part of the spectrum (300–420 nm); Em is the emission part (420–600 nm).
Although also the optical path and parts of the AGE Reader have been designed to be similar to that of the AFR, some differences between the two instruments exist. The AGE Reader has a Borofloat-glass window (Schott, Jena, Germany) in the sample opening for protection of the interior. This glass window has been selected for exhibiting only very low fluorescence. Furthermore, a rubber mat is applied for better shielding of environmental light and subject comfort and to aid proper cleaning. To arrive at an instrument that provides results in agreement with the AFR, a direct intraindividual comparison between the AFR and an AGE Reader was performed by DiagnOptics Technologies, using a limited number of healthy individuals and subjects with diabetes (n = 25) with a broad range of age and skin AF values. Figure 2 shows the results from this substudy.
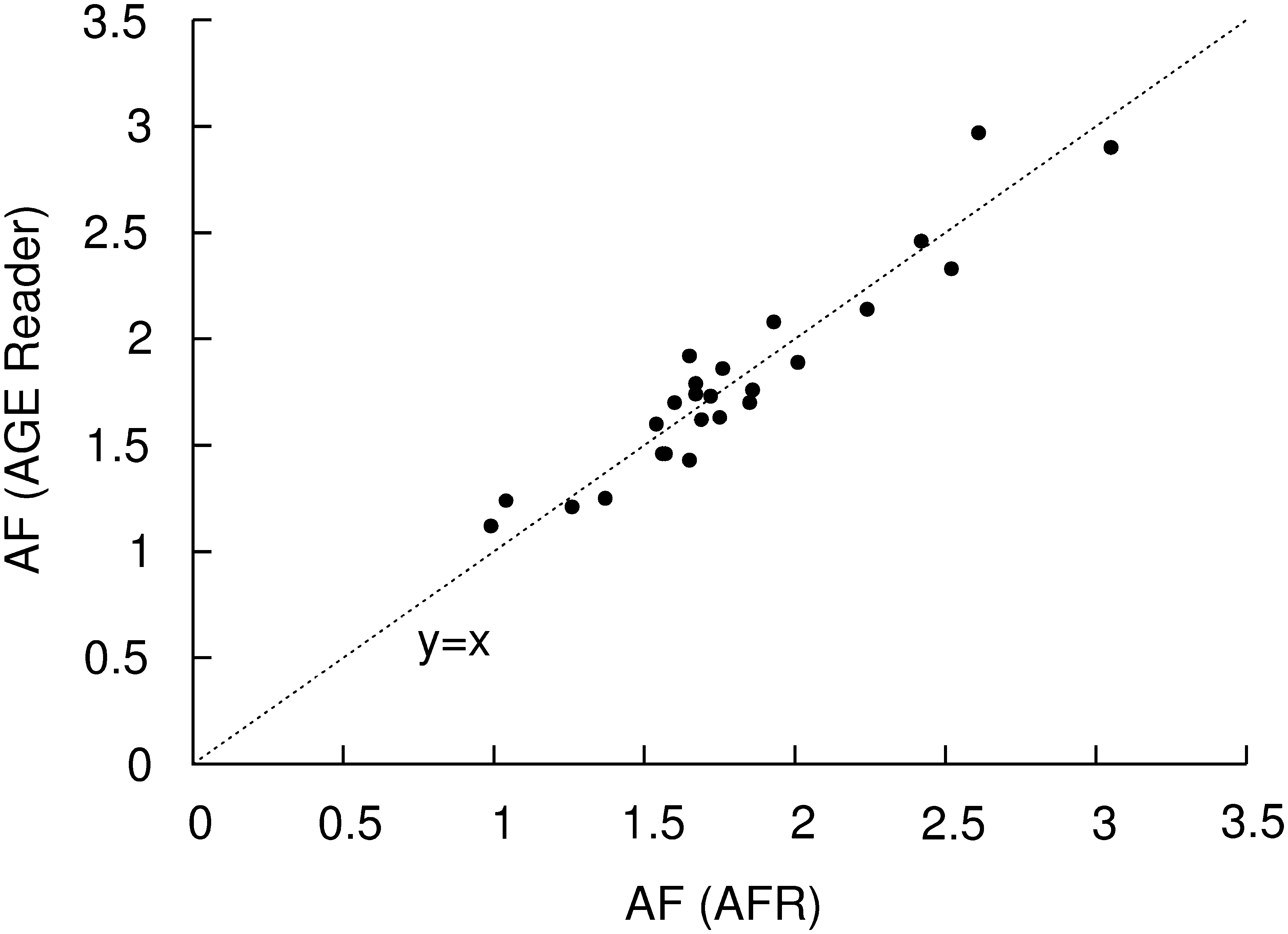
Skin AF as measured with the AGE Reader compared to the AFR. R 2 of a fit-line (not drawn) is 0.90.
Measurements in the first group
In the previous study, skin AF values were collected using the AFR from a group of 231 Caucasian subjects. 7 The study is limited to Caucasian subjects because dark skin may influence skin AF assessment. 6 Skin AF was measured at three positions on the volar side of the lower arm, and the mean of these three measurements was used in the analysis. Besides skin AF values, information was obtained on age, gender, body mass index, current smoking status, and systolic and diastolic blood pressure. Subjects were regarded as nonsmokers if they did not use tobacco within the last year. Only subjects with no known history of diabetes, cardiovascular events, or renal dysfunction (creatinine values within reference values of 70–110 μmol/L) were included. As the subjects were recruited from the outpatient clinic for presurgery screening, they were further classified according to the American Society of Anesthesiologists (ASA) score (1–5). In the present study, only the control subjects, who had an ASA score of 1 or 2 (ASA 1 = normal healthy subjects; ASA 2 = subjects with a mild systemic disease), were included. The 20 persons with ASA score 3 were not included in the current analyses.
Measurements in the additional group
In addition to the measurements described above, we used the AGE Reader to measure skin AF in a group of 281 Caucasian volunteers with a broad age range. Using a self-administered questionnaire, information was obtained on age, gender, and current smoking status. Further items assessed in the questionnaire were history of hypertension, diabetes, stable coronary artery disease, acute coronary syndrome or coronary revascularization or intervention, stroke, and renal dysfunction. Subjects were excluded from this study if one of these items were positive or in case of pregnancy or use of body lotions or creams on the measuring site.
Analyses
The AGE Reader and AFR are similar instruments and should therefore generate the same results. Data of both groups were compared to evaluate this similarity. Because tobacco smoking influences skin AF, 7,14 only nonsmokers were included in this first comparison. After correction for subject age, both groups were compared using Student's t test. After the similarity of both instruments was established, results from both groups were combined for the further assessment of skin AF. Least squares linear regression analysis was performed on the total group, to obtain reference values for skin AF in a healthy population as a function of age. Subsequently, the effect of tobacco smoking was analyzed, after correcting for subject age. Finally, the effect of gender was investigated for the current smokers and the nonsmokers, by assessing the gender-dependent residual after correction for age using the respective age fits for smokers and nonsmokers.
Results
Skin AF values of the nonsmokers as obtained with the AFR and the AGE Reader are shown in Figure 3. Different symbols were used to show which of the instruments was used for each measurement. For the linear regression fits, only subjects less than 70 years old were included. In both groups, skin AF increases equally with subject age. The offset of 0.03 AU between the two regression lines is not significant (P = 0.26).
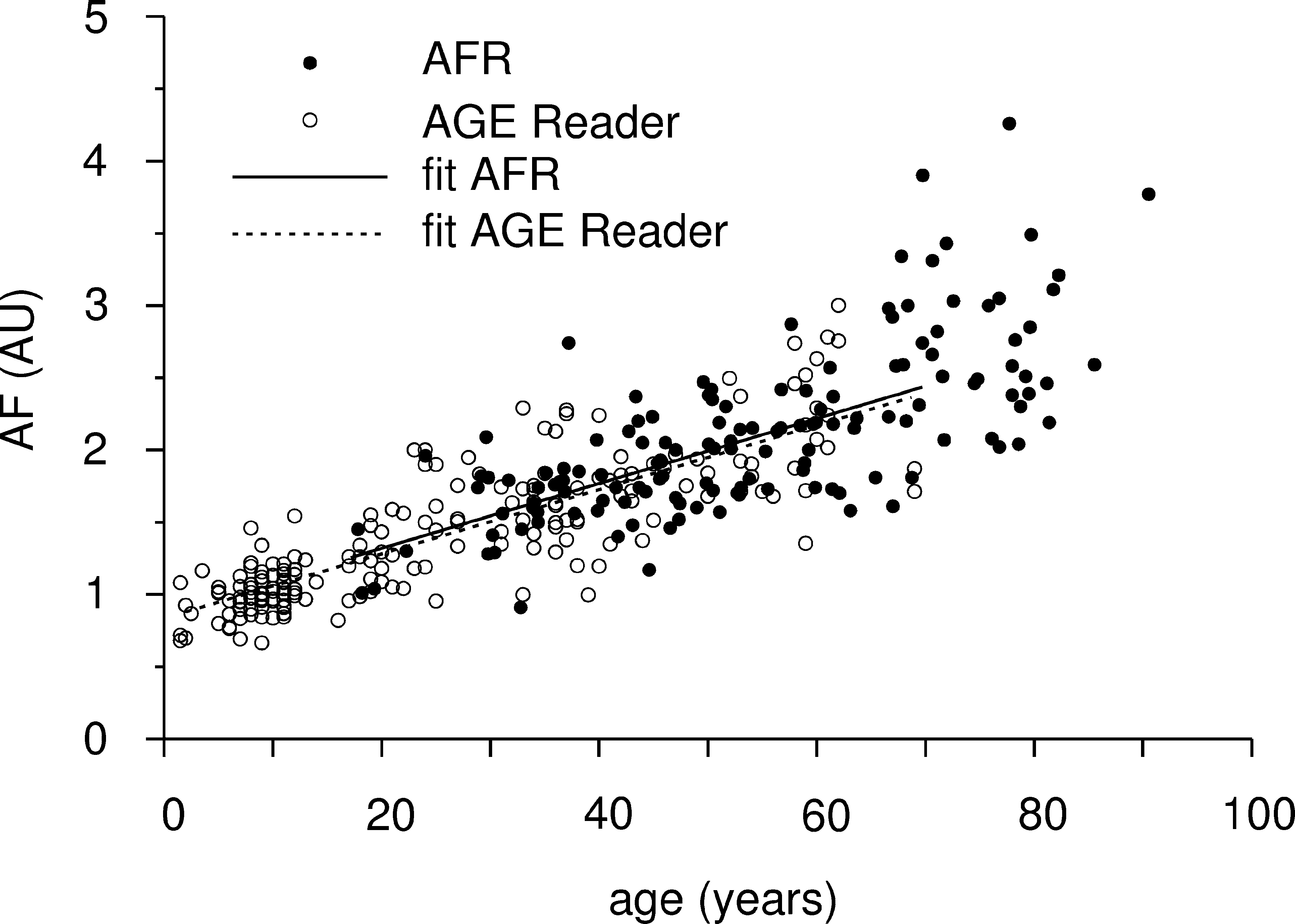
Skin AF as a function of subject age. The data and linear regression fits are obtained from the AFR group (solid symbols and solid line) and the AGE Reader group (open symbols and dashed line). The fits are determined using least squares fitting.
Group characteristics
For the measurements in the previously reported reference group, 7 211 subjects (129 female and 82 male) were included. Age was 51 ± 17 years (mean ± SD) and ranged from 17 to 91 years. In this group, 32% of the subjects were current smokers (40 female and 28 male). For the measurements in the new cohort, 217 subjects (119 female and 98 male) were included. Age was 27 ± 17 years (mean ± SD) and ranged from 1.5 to 69 years. In this group, 13% of the subjects were current smokers (16 female and 12 male).
From here on, both groups have been combined into one large group of 428 subjects (248 female and 180 male). Age was 38 ± 21 years (mean ± SD) and ranged from 1.5 to 91 years. In the total group, 22% of the subjects were current smokers (56 female and 40 male).
Influence of age and smoking status
Skin AF values for the nonsmokers and the current smokers of the total group are shown in Figure 4. Skin AF for the nonsmoking subjects can be described as 0.023 × A + 0.83 (R 2 = 68%), where A is subject age in years. The SD around this fit is 18% of the fit-value, independent of age. The current smokers have an increased skin AF compared to the nonsmokers, which can be described as 0.029 × A + 0.78 (R 2 = 41%). The SD around this fit is 23% of the fit-value, independent of age. The age related increase in skin AF was not significantly different between current smokers and nonsmokers (P = 0.12). The effect of smoking on the skin AF value is given by an absolute increase, which is 0.16 AU (P < 0.01). The difference between smokers and nonsmokers within each age group is only significant for the age groups 30–40 and 60–70 years.
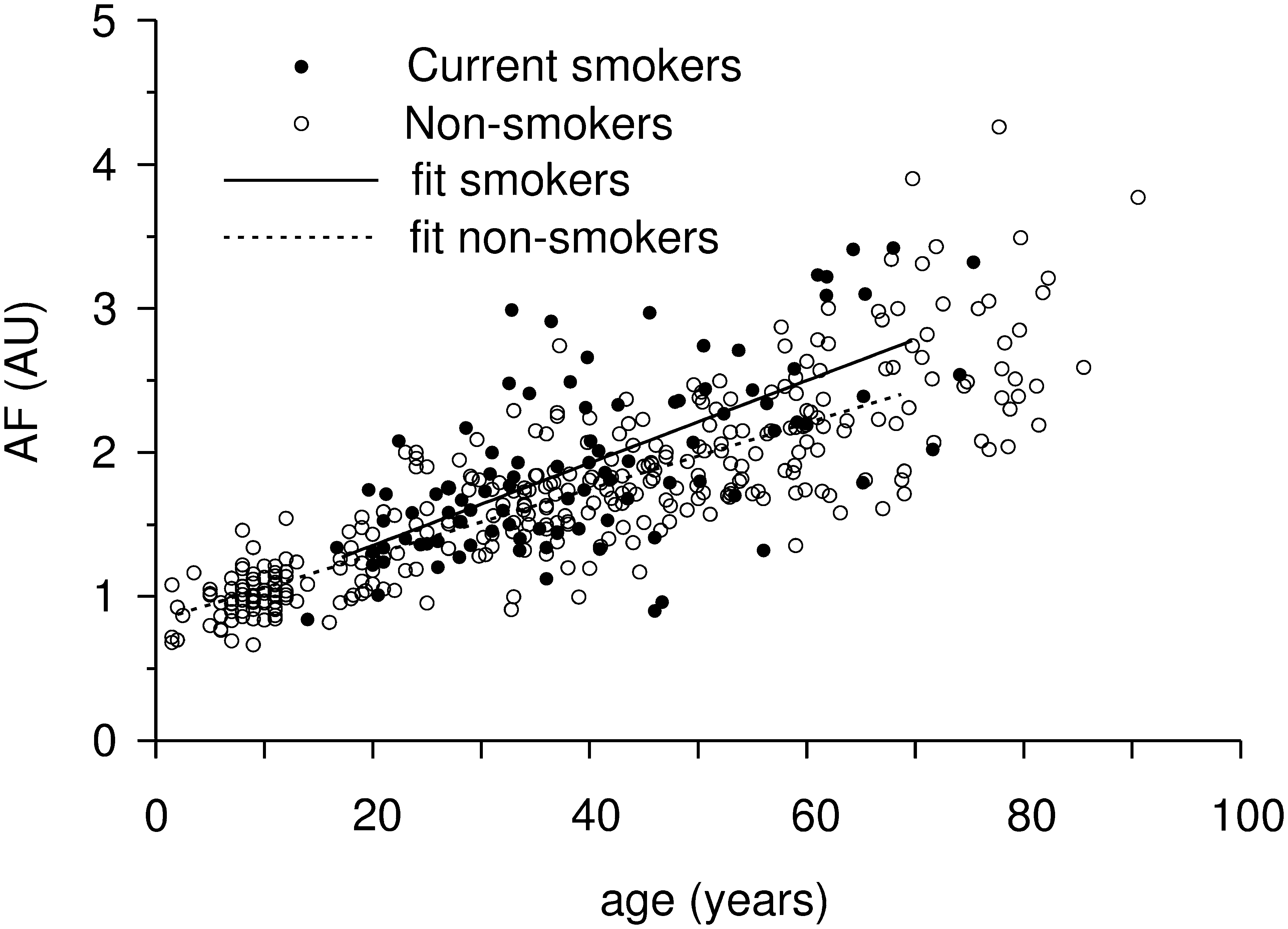
Skin AF for the current smokers (solid symbols and solid line) and the nonsmokers (open symbols and dashed line) of the total group as a function of subject age. The fits are determined using least squares fitting.
When both groups (nonsmokers and current smokers) are combined, skin AF of the total group can be described as 0.024 × A + 0.83 (R 2 = 60%). This fit is not significantly different from the fit for the current nonsmokers only (P = 0.17). The SD around the fit is 20% of the fit-value, independent of age.
The mean skin AF values per age group of 10 years are summarized in Table 1 for reference. The increase in skin AF per 10 years is significant for most age groups as indicated in Table 1.
Data are mean ± 1 SD values, in AU. Significance between subsequent age groups is indicated as P values from Student's t test.
Influence of gender
Within the nonsmokers group, no effect of gender on skin AF was found. Among the current tobacco smokers, the female subjects had a higher skin AF than the male subjects. The effect of gender on the current smokers as studied up to 70 years of age was not dependent on age and was quantified as an absolute increase of 0.2 AU (P = 0.02). Female smokers had skin AF values of 0.24 higher than nonsmokers (P < 0.01); male smokers had skin AF values of 0.04 higher than nonsmokers (P = 0.56).
Discussion
This study provides reference values for skin AF with the AFR and the AGE Reader, which provided values for skin AF that are in agreement with each other. Skin AF can be described as a linear function of age over a broad age range up to the age of 70 years, with a remarkably constant degree of variation.
In the literature, a linear relation between skin AF and subject age has often been suggested. 15 –17 With the results of the present study, we also constructed exponential and other regression fits. However, these yielded no better results than linear fits. For practical and clinical use, the given linear fits sufficiently describe the relation of skin AF with subject age.
Tobacco smoking increases AGE accumulation and skin AF. 7,14,18 In the present study population, skin AF was increased in current smokers compared to nonsmoking subjects by an absolute increase of 0.16 AU. We expected that the effect of smoking is increasing with age, because older smokers presumably have been smoking longer and have a higher number of pack-years than the younger subjects and may thus have had more and longer exposure to exogenous AGEs in tobacco smoke. However, in our subject group, adding the current smokers (22% of all subjects are current smokers) to the total group results in no significant increase of average age-corrected skin AF.
In the present study, the percentage of smokers was 22%, which may be different in other studies. A formula may be constructed based on a weighted summation of the fits that were found in this study for nonsmokers and current smokers. Reference values of skin AF can thus be adapted to the numbers of current male and female tobacco smokers who are present in the population of interest.
It should be noted that both age and smoking status should be taken into account also in populations of patients suffering from diabetes or diabetes-related complications because smoking status has been shown to be independently and positively related to skin AF, in healthy subjects as well as in patients with diabetes. 7
In our previous study, no difference was found in skin AF values for gender in control subjects. 7 In the current study, we found no differences in skin AF between the female and male nonsmokers. However, within the group of current smokers, female subjects had a higher skin AF than male subjects after correction for age. This suggests that women may suffer more from the effect of smoking than men, an effect that is also seen in chronic obstructive pulmonary disease. 19
Food may have a small influence on skin AF: one study reported a 8.7% increase of skin AF in healthy subjects 2 h after a high fat breakfast (600 kcal) with also a considerable AGE content. 20 The effect of this meal barely decreased after 4 h. In a study where food intake was not restricted, the variation of skin AF over the day was 5%. 6 If food intake would have had an influence in the present study, this influence would have been randomly distributed over the subjects. The reference values of the present study can therefore be used for measurements in nonfasting subjects.
Within each age group of 10 years, the SD of the mean is approximately 20%. Because the coefficient of variation in skin AF for a single measurement is approximately 5%, 6 the remaining variation between subjects can be explained as variation in the amount of accumulated skin AGEs and therefore their relative risk for development of cardiovascular disease. Tissue AGE accumulation has been proposed as a carrier of so-called metabolic memory and the legacy effect. 21 The variation in skin AF may at the same time represent the interindividual differences in metabolic memory and vascular damage.
Only subjects with an age below 70 years were included in the linear fit analysis. Although the linear regression for skin AF seems to continue beyond this age, we noted that some elderly subjects have a more increased skin AF value. Higher skin AF values may be expected in elderly subjects because they may develop complications related to age. On the other hand, it may be expected that the elderly may have a relatively lower skin AF value because lower skin AF is associated with longer survival. These two effects explain the wider distribution and uncertainty, which is the reason why we excluded this age group from the linear regression analysis.
The current study is limited to Caucasian subjects. Therefore, our results may not be applicable to subjects with more pigmented skin. Improvements of the AGE Reader are in progress to enable reliable skin AF measurements in those subjects.
In conclusion, the described relation of skin AF with age, smoking status, and gender as shown for Caucasians provides reference values to apply in clinical settings and future studies.
Footnotes
Author Disclosure Statement
R.G. and A.J.S. are also founders and stockholders of the university spinoff DiagnOptics Technologies BV, manufacturer of the AGE Reader (