
Abstract
Background:
Preventing the complications of diabetes requires tight control and minimizing blood glucose fluctuation. Pursuing these goals increases the risk of severe hypoglycemia. The authors hoped to identify if using continuous glucose monitoring (CGM) decreased the incidence of severe hypoglycemia, resulted in less fear of hypoglycemia, and improved patient empowerment and what impact CCM had on quality of life (QOL) issues.
Methods:
Questionnaires were used to gather demographic data, to measure educational experiences with CGM, QOL issues concerning fear of hypoglycemia and severe hypoglycemia, confidence to make changes to insulin regimens before and after using CGM, and the incidence of severe hypoglycemia before and while using CGM, and to assess the impact of CGM on QOL.
Results:
The data and answers reported suggest significantly less fear of hypoglycemia and severe hypoglycemia and increased patient empowerment with CGM. Further shown is a reduced incidence of acute complications as evidenced by significantly decreased incidence of severe hypoglycemia. CGM appears to have a significant, positive impact on the stress associated with having and managing diabetes.
Conclusions:
Using CGM as part of the diabetes self-management plan offers the potential to significantly improve user outcomes as measured by QOL, reduction of fear, and patient empowerment. Using CGM can allow patients to achieve tighter control of their blood glucose values with reduced fear of hypoglycemia, reduced incidence of severe hypoglycemia, and a decreased sense of burden from having diabetes.
Introduction
It has been emphasized that CGM is not a “cure but another measure that may for some bring a far better level of glucose control while reducing the incidence and risk of hypoglycemia.” 9 If true, does this premise also lead to improved quality of life (QOL)? Does it cost more or less—is the cost only economical? Are there more benefits than burdens?
To assess the effects of CGM on QOL, one needs to measure the potential benefits to the patient versus the disadvantages. In reviewing early retrospective data for benefits, no difference was shown in QOL and fear of hypoglycemia with CGM. Further, there are few available data on this topic using real-time CGM. However, studies have convincingly shown a decrease in A1c with CGM. 10,11
Published studies have shown a decrease in time spent in hypoglycemia while using CGM. 5,6 It has also been stated that sufficient evidence providing clear demonstration of the impact of CGM on hypoglycemic unawareness and severe hypoglycemia is still missing. 10
The primary objectives of the present study were to query 150 subjects with type 1 diabetes who had purchased and used a CGM system about their experience. Specifically, the authors looked at these questions: Do people using CGM get the right information about how to use it accurately and effectively? Does using CGM result in less fear of hypoglycemia, less stress overall concerning one's diabetes, and an increase in confidence in diabetes management ability? Did using CGM impact the psychological burden of having and managing diabetes and reduce the incidence of severe hypoglycemia?
Subjects and Methods
Rocky Mountain Diabetes and Osteoporosis Center (RMDOC) is a specialty and primary care practice in Idaho Falls, ID. In January 2008, the practice patient population of 17,000 included a registry listing 1,200 people with type 1 diabetes and 550 PWD type 1 using continuous subcutaneous insulin infusion. One hundred fifty patients within the diabetes registry were known to be using or had recently used real-time CGM systems. All the patients using CGM had type 1 diabetes. The study group consisted of subjects who purchased and used personal systems and were not participants in industry-sponsored research.
The 5-page RMDOC CGM and QOL (RMDOC CGM/QOL) Questionnaire was developed in December 2007 and mailed to subjects in January 2008. Questions were multiple choice and fill in the blank. The authors conferred with William Polonsky, Ph.D. regarding a QOL measurement, and the Diabetes Distress Scale (DDS) was provided for use in this study. A second, 1-page questionnaire was mailed separately from the first asking two multiple choice questions about the incidence of severe hypoglycemia 6 months prior to and while using CGM. In total, subjects were asked to complete 8 pages of questions.
All materials were submitted to the local Institutional Review Board, and 150 questionnaires were mailed to all RMDOC patients with type 1 diabetes over the age of 18 years who had used CGM therapy for any length of time (1 month to 2.5 years). The anonymous responses were mailed back to RMDOC in self-addressed, stamped envelopes. No questionnaires were accepted into the data pool after April 1, 2008.
The data were transferred to and tabulated using an Excel (Microsoft, Redmond, WA) spread sheet. Analyses were performed using analysis of covariance and the Wilcoxon signed-rank test for matched pairs. Analyses examined the clinical significance between patients using CGM in the management of their diabetes versus those who were using CGM and stopped.
RMDOC CGM/QOL Questionnaire
A total of 150 questionnaires were mailed to CGM users, and 54 (36%) of the initial mailing and 58 (39%) of the second mailing were returned to RMDOC. The first part of the RMDOC CGM/QOL Questionnaire collected information designed to unveil characteristics of the CGM users: Age, gender, ethnicity, education, diabetes history, diabetes management CGM training received by users Type of CGM system used Who paid for the CGM systems Who continued, who quit, and why
The second half of the RMDOC CGM/QOL Questionnaire looked at the impact of CGM on the level of fear related to hypoglycemia before and after CGM use and on the confidence to adjust the insulin regimen.
It is important to recognize the limitations of this study. It is retrospective and self-reported and deals with a small population of subjects. The RMDOC CGM/QOL Questionnaire was developed by the authors and is not validated.
Results
Demographics
Subjects varied widely in age, but those who stopped using CGM were younger by 5 years. Those using CGM were older than expected, with 19% over the age of 60 years (Table 1). The level of education ranged from high school dropouts to advanced degrees. Education level did not statistically relate to whether the subject continued or stopped using CGM. Responders were overwhelmingly insulin pump users: 49 pump users versus five multiple daily injection. Twenty-one DexCom™ (San Diego, CA) STS®, 26 DexCom Seven®, five Medtronic (Minneapolis, MN) MiniLink™, and two Medtronic MiniMed Guardian® CGM systems were used.
Fifty-two subjects (96%) received education on how to use their system, and 85% were trained by a C.D.E. from either RMDOC or from the CGM manufacturers. Seventy-five percent came to the clinic for follow-up at least once. Forty-one percent of subjects electronically downloaded CGM information from their systems, and 75% of these subjects discussed the results with their C.D.E. or physician.
Fifty percent of all subjects stopped using CGM. Subjects were allowed to identify more than one reason for stopping use. Reasons for stopping are given in Table 2.
Thirty percent cited cost as the only reason for stopping CGM.
RMODC CGM/QOL Questionnaire
Subjects were asked to rate their fear of hypoglycemia, severe hypoglycemia (hypoglycemia requiring intervention from another person to treat), and improvement in confidence to make changes to personal insulin regimens before using CGM and while using CGM. Subjects were asked to rate their fear on a 1 to 5 Likert scale, with 1 being the least fear and 5 the greatest, or 1 being the least confident and 5 the most confident.
The reduction of fear of hypoglycemia was shown to be significantly greater in all subjects who used CGM and continued to use CGM (Fig. 1).
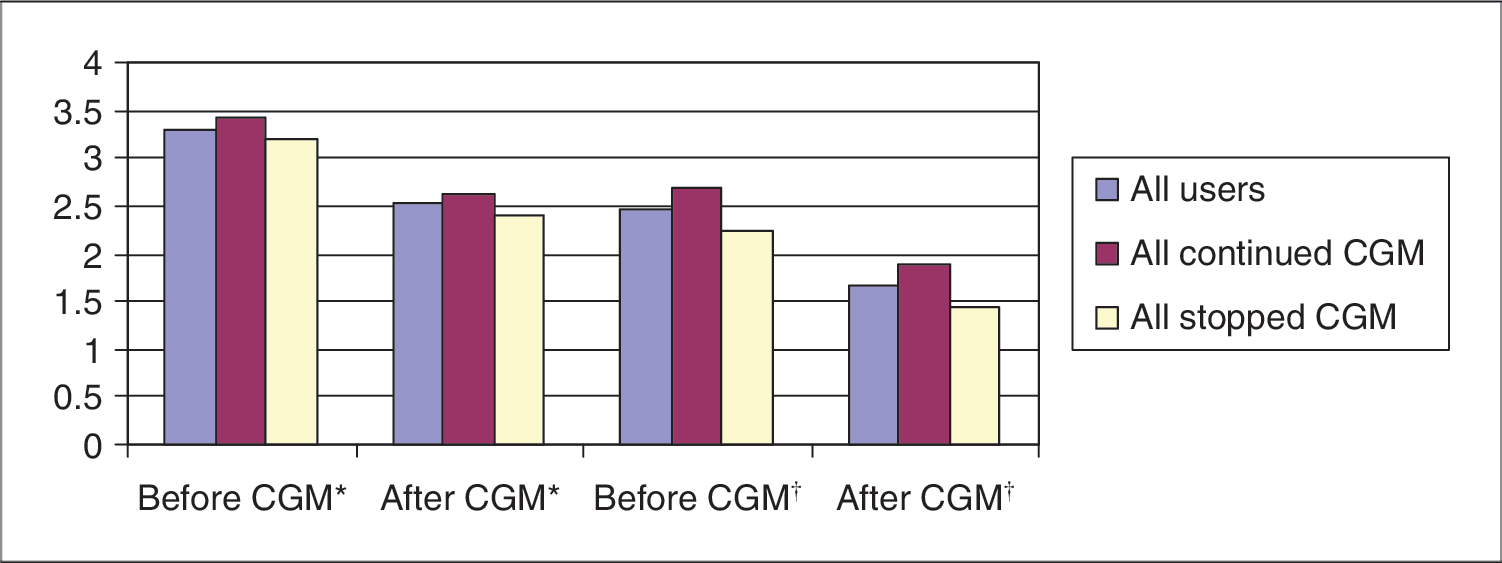
RMDOC CGM/QOL Questionnaire: reduced fear of hypoglycemia and severe hypoglycemia. *Subjects' answers concerning fear of hypoglycemia. †Subjects' answers concerning fear of needing help to treat severe hypoglycemia. Color images available online at
DDS
The DDS is a simple, 1-page questionnaire that asks a series of questions subsequent to a subject having diabetes that allow a level of psychosocial stress in his or her life to be determined. Each question is answered with a rating of 1 to 5. The higher the rating, the greater perceived level of stress the patient feels concerning the question. There is an overall DDS score as well as scores for Emotional Burden, Physician Distress, Regimen Distress, and Interpersonal Distress. The DDS was administered only post-CGM use. A second group of patients who had never used CGM were surveyed with the DDS as a control group (Table 3).
RMDOC incidence of severe hypoglycemia questionnaire
This questionnaire was mailed 1 week after the initial questionnaires to the same 150 subjects who received the first questionnaire. It included two questions addressing the incidence of severe hypoglycemia in the 6 months prior to using CGM and the incidence of severe hypoglycemia while using CGM. Fifty-eight questionnaires were mailed back. It is unknown if the same subjects responded to the second questionnaire as responded to the first questionnaire.
CGM use significantly reduced the incidence of reported severe hypoglycemic events (Table 4) by 32.8% among the respondents to this questionnaire.
P = 0.0006, Fisher's exact test, two-tailed.
Discussion
Demographics and education
Study data from this subject population provided beneficial information about CGM use. The subjects were older than expected, with the oldest being 76 years. Subjects had a variety of occupations, including agricultural, white collar, and blue collar. Level of education and gender did not play a role in who continued or stopped CGM. Thirty percent of subjects cited cost as the only reason for stopping CGM. Eleven percent who stopped had insurance coverage, and 19% of all users had insurance coverage for their systems and sensors. Cost does not appear to be an insurmountable obstacle to using CGM. Subjects received initial education on how to use their systems but did not always returning for follow-up. Fewer than half the subjects were using the download-management software.
Having patients identify if they are good CGM candidates should be part of the initial orientation process and occur before the decision to purchase a CGM system is made. Setting realistic expectations of what CGM can and cannot do will help increase patient satisfaction with the technology and reduce the incidence of non-use.
Using the management software to download historical glucose data further increases the value of CGM. Teaching patients to interpret the downloaded data will empower them to make appropriate changes in their insulin regimens to reduce glucose variability and improve their A1c. Follow-up with the healthcare provider is essential to enabling patients to maximize the benefit of CGM.
Continued use
Several subjects reported they “felt tied to the CGM, it ruled my life, it got caught on things at work, and/or it alarmed all the time.” Despite these inconveniences subjects used CGM on a continuous basis 78% of the time. Those who used it intermittently did so to reduce costs. Ninety-eight percent of all subjects used the sensors longer than the manufacturer's indicated wear time for a single sensor. The longest time reported was 21 days for the Dexcom STS sensor. During CGM training patients were taught by the education staff at RMDOC to restart the sensor. Patients were taught to determine if the data from the receiver were reliable by looking at gaps in data reporting, decreased consistency between sensor and blood glucose monitor readings, and increased alerts for additional calibrations. No comments were made concerning skin irritation or infection.
Stress reduction
The level of stress reported was higher in all categories for CGM stoppers versus continued users, with the difference being significant for Physician Distress and Regimen Stress (Fig. 1). Research has shown there is an inherent level of stress that comes with adding more management tasks. It may be favorably argued that adding CGM to a diabetes regimen did not increase stress significantly in continued users when compared to naïve controls. The slight increase in stress seen is potentially offset by the benefit. The DDS scores may suggest that interpersonal distress may be reduced. Increased confidence in the management regimen may relate to an improved relationship with the health care provider.
Can conclusions be drawn about stress reported by these participants? One can speculate using two different scenarios:
Speculation 1
All learners start with the same level of diabetes-related distress. One group receives education that they understand, embrace the technology, thrive (in relationship and benefit), and continue with CGM and ultimately become less distressed. Another group receives education that they do not understand, becomes overwhelmed because they do not receive the support they need, does not embrace the technology, becomes more distressed, and ultimately stops using CGM.
Speculation 2
All learners are not the same. One group consists of people who are open to change, have less stress, use the technology, and thrive. Another group consists of people who have more stress, are resistant to change, become more stressed with time, quit trying, and ultimately give up.
Confidence to make changes
The person using CGM gains confidence to make changes in management regimens when presented with a larger body of glucose values to support changes and decisions. Although it must be acknowledged that currently available CGM systems are to be used adjunctively with traditional fingerstick self-monitoring of blood glucose, looking at and analyzing CGM information provides the patient with insight to glucose patterns that may make adjustments to regimens more meaningful. Subjects in the continued use group scored higher on confidence to make changes in their insulin regimen than subjects in the stopped use group. Eighty-five percent of continued users scored 4 or 5 for confidence to make changes after using CGM compared to 67% of stopped users. Additionally, 59% of continued users started with a pre-CGM confidence score of 4 or 5 compared to 29% of stopped users. This may indicate that certain subjects are less likely to want to manage their insulin regimens more aggressively (lower confidence) and will realize less benefit from CGM and potentially abandon the technology.
Fear of hypoglycemia
All subjects reported that, while using CGM, whether they continued or quit, they had less fear of hypoglycemia and severe hypoglycemia. All results are highly significant with a P value of < 0.001. CGM systems allow users to set alerts that notify of falling glucose values or values below a set target. Many patients have found that setting the glucose hypoglycemic alert higher (90 versus 80) allows the necessary time to correct the falling glucose, avoid hypoglycemia, and potentially reduce the fear of severe hypoglycemia.
A second questionnaire addressing the incidence of severe hypoglycemia 6 months prior to and while using CGM found CGM use reduced the incidence of severe hypoglycemic events (see Table 4). These data show a 32.8% reduction in hypoglycemic events requiring assistance from family or friends, emergency medical technicians, or physicians' offices or at the emergency room while subjects were using CGM systems.
In summary, users experienced: Less fear of hypoglycemia and severe hypoglycemia Increased confidence to make changes to their insulin regimen Reduced incidence of acute complications, i.e., a decrease in the incidence of severe hypoglycemia requiring assistance and potentially hypoglycemic unawareness Significant, positive impact on the stress associated with having and managing diabetes
Conclusions
This small retrospective study provides stimulating feedback about CGM use, users, and value of CGM use on QOL and potential costs. In the completed analysis, the data indicate a statistically significant value of CGM use to QOL, level of stress associated with having and managing diabetes, and reduction in the incidence of severe hypoglycemia.
It is important to continue studies to further assess use habits of CGM, ultimate costs and benefits to QOL, and potential economic impact. Future studies may provide greater clinical insight by administration of the DDS and RMDOC CGM-like questionnaires pre-, post-, and at interval use of CGM. Suggestions for similar studies include evaluation of use of self-monitoring of blood glucose throughout the CGM wear, scheduled A1c tests, and validation of self-reported hypoglycemia by electronic downloading of the CGM. A tally of cost (economic) of severe hypoglycemia through journal use of the event (who treated and how, activity stopped or time lost, etc.) is worthy of investigation as well.
Footnotes
Acknowledgments
The authors express grateful appreciation to: John E. Liljenquist, M.D., Rocky Mountain Diabetes and Osteoporosis Center; Timothy Dunn, Ph.D., Abbott Diabetes Care; William D. Polonsky, Ph.D.; and the Fraternal Order of Eagles, 576 Auxiliary, Idaho Falls, ID, for their generous funding for this study.
Author Disclosure Statement
J.H. is employed at Rocky Mountain Diabetes and Osteoporosis Center in Idaho Falls, ID. She is a consultant for Eli Lilly and Abbott Diabetes Care. C.H. is employed as a Scientific Affairs Manager for Abbott Diabetes Care, headquartered in Alameda, CA, but the performance of this study was done unrelated to her work at Abbott.