
Abstract
Background:
A progressive weight gain is associated with various pharmacological options improving glycemic control in type 2 diabetes mellitus (T2DM). Ghrelin has been implicated in the regulation of feeding behavior and energy balance in humans. Based on evidence that functional ATP-sensitive channels are present in ghrelin-producing cells, we hypothesized that meglitinides may affect circulating ghrelin levels in subjects with type 2 diabetes.
Methods:
In a single-blinded randomized three-period crossover study (n = 20), repaglinide or nateglinide was given in combination with metformin for two treatment periods over a 1-week period, respectively, separated by a 1-week treatment with placebo. Liquid meal challenge tests (LMCTs) with single preprandial doses of repaglinide (2 mg), nateglinide (120 mg), or placebo were performed at the end of each treatment period. Ten control subjects without diabetes underwent a single LMCT without any medication.
Results:
Fasting ghrelin concentrations were not different between all treatments and between patients with diabetes and control subjects. Subjects with T2DM treated with placebo showed no suppression of ghrelin in the LMCT. After administration of meglitinides a nadir of serum ghrelin was observed at 60 min (8.6% of baseline [P = 0.038] for repaglinide and 7.5% of baseline [P = 0.081] for nateglinide), which was similar to the secretion pattern seen in control subjects. No correlations between postprandial insulin or glucose levels and circulating ghrelin concentrations were observed.
Conclusions:
Treatment with meglitinides reconstructed postprandial ghrelin secretion patterns to those of controls without diabetes. This observation may help to improve the control of feeding behavior in patients with T2DM.
Introduction
Ghrelin is a 28-amino acid peptide with a fatty acid side chain produced and secreted in different parts of the gastrointestinal tract. 6,7 Ghrelin has emerged as an important factor in the control of energy homeostasis that stimulates food intake and promotes obesity. 8,9 Cross-sectional studies showed an increase of circulating ghrelin concentrations in anorexic individuals and a suppression of ghrelin concentrations in obese subjects. 10,11 Ghrelin levels rise in the fasting state 12 and decline sharply following meals. 13 The detailed mechanisms controlling ghrelin secretion in humans remain unclear. The role of insulin in ghrelin regulation has been suggested but was controversial in replication studies. 14 On the other hand, hyperglycemia induces rapid decreases in plasma ghrelin concentrations after intravenous or oral glucose loading. 15 –17 Besides insulin and glucose, some gastrointestinal 18,19 and hypothalamic hormones regulate circulating ghrelin concentrations. 20,21
Despite the rising evidence of potential therapeutic applications of ghrelin and ghrelin analogs in obesity and metabolic syndrome, 22 only a few studies investigated regulation of ghrelin secretion in T2DM. 23 –25 Moreover, metformin decreases postprandial ghrelin levels in subjects with T2DM 26 and in subjects with metabolic syndrome. 27 Controversially, the other insulin-sensitizing agent, pioglitazone, had no effect on the circulating ghrelin level. 28
Repaglinide and nateglinide are structural relatives of meglitinide, the nonsulfonylurea moiety of glibenclamide. 29 Both drugs also bind to ATP-sensitive potassium channels in other tissues. 30 Native gastric ATP-sensitive potassium channels are present in oxyntic cell and gastric mucosal membrane 31 and were shown to interact with tolbutamide. 32,33
Based on these data, we hypothesized that meglitinides may regulate ghrelin production from X/A-like oxyntic cells and affect circulating ghrelin levels in T2DM subjects.
Subjects and Methods
Study protocol
The study protocol was approved by the ethical committee of the Campus B. Franklin, Charité University of Medicine Berlin, Berlin, Germany.
Subjects
Subjects with T2DM
Twenty subjects with T2DM participated in the study. Inclusion criteria were age between 35 and 75 years, body mass index (BMI) between 20 and 45 kg/m2, pre-existing T2DM treated with diet or metformin, fasting C-peptide concentration >1 ng/mL, and negative for glutamic acid decarboxylase-II antibodies. Only subjects with a physician's diagnosis of T2DM (ICD10:E11) were included in the study. Subjects were excluded when they reported infectious, gastrointestinal, or diabetes treatment with insulin secretagogues, insulin, or thiazolidindiones. Subjects with elevations of liver enzymes more than twice upper normal limits, with elevated serum creatinine concentrations (>1.3 mg/dL), or with severe conditions including generalized inflammation, heart failure, or end-stage malignant diseases were excluded from the study. All subjects were instructed to avoid significant physical activity during the 3 days preceding each examination day and to keep records of their nutritional behavior throughout the study period. Three subject with diabetes were treated with diet and/or exercise alone and 17 with metformin as monotherapy.
Control group
Ten age- and weight-matched control individuals without diabetes were not drug-treated and received single liquid meal challenge test (LMCT) after a 10-h overnight fast. They did not take any medication known to affect glucose tolerance, insulin sensitivity, or insulin secretion. All subjects were instructed to maintain their usual diet and physical activity before the study. In all control subjects diabetes mellitus and impaired glucose tolerance were excluded by a 75-g oral glucose tolerance test (OGTT). 34
Study design
A complete physical examination, OGTT, and laboratory evaluation were performed on each patient during the screening period. If the subjects met the inclusion criteria, they were recruited for the participation in a single-blind randomized placebo-controlled crossover study including three treatment periods of 1 week in duration (Fig. 1). During the 2 weeks of the run-in period, all patients were treated with metformin (2,000 mg/day). For the first treatment period, patients were randomized to one of two treatment groups: repaglinide 1 mg three times daily before meals or nateglinide 60 mg three times daily before meals, with both drugs given in addition to metformin (2,000 mg/day). In the following second treatment period all subjects with diabetes were treated with placebo in combination with metformin (2,000 mg/day). In the third week patients with diabetes were treated in crossover with repaglinide or nateglinide, with both drugs given in addition to metformin.
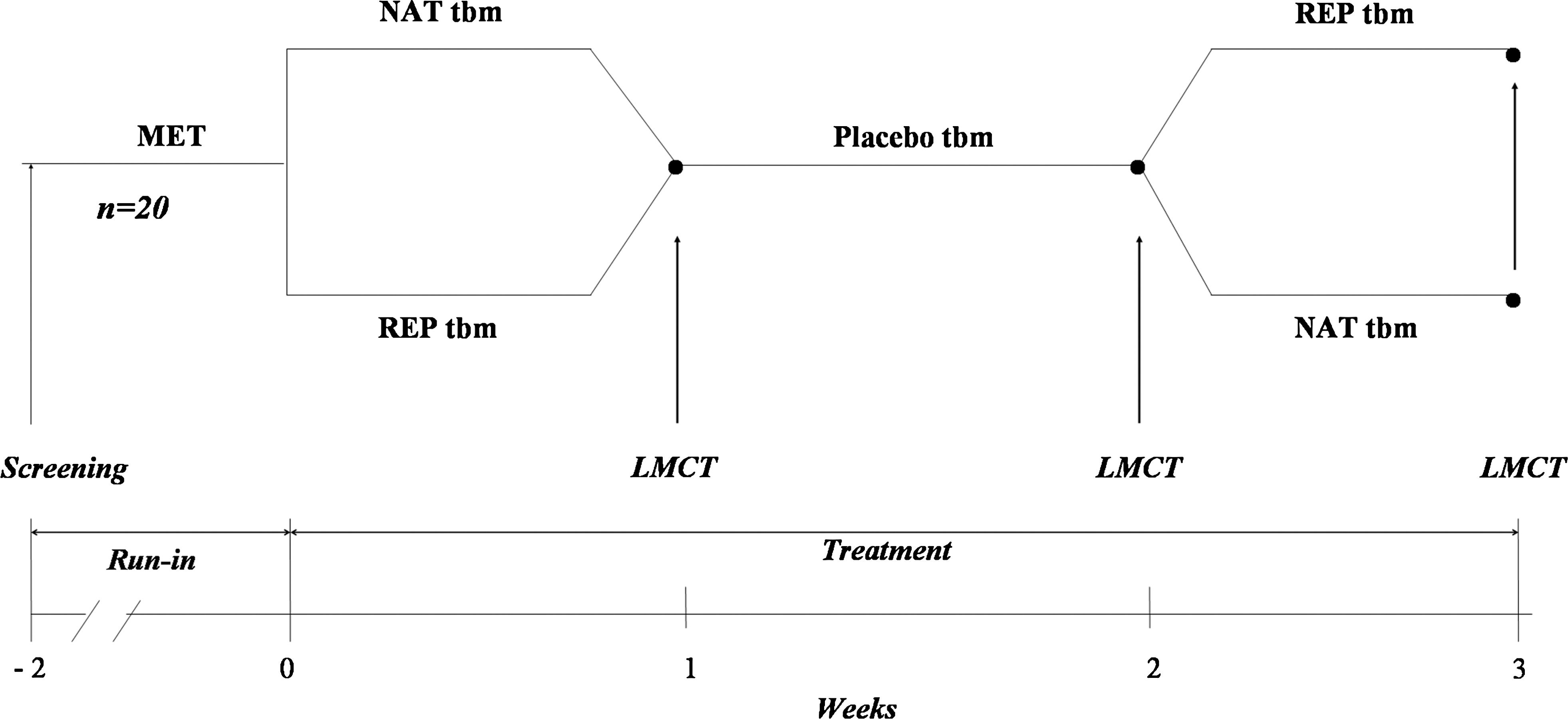
Study design. Twenty subjects with T2DM participated in the single-blind randomized placebo-controlled crossover study lasting 3 weeks. During 2 weeks of the run-in period, all patients were treated with metformin (2,000 mg/day) (MET). For the first treatment period patients were randomized to one of two treatment groups: repaglinide 1 mg (REP) three times daily before meals or nateglinide 60 mg (NAT) three times daily before meals (tbm), with both drugs in addition to MET. In the following second treatment period all subjects with diabetes were treated with placebo in combination with MET. In the third week patients with diabetes were treated in crossover with repaglinide or nateglinide, with both drugs in addition to metformin.
LMCTs with single preprandial doses of repaglinide (2 mg), nateglinide (120 mg), or placebo at the end of each treatment period were performed three times during the study. The control subjects without diabetes were not treated with drugs and received a single LMCT.
Experimental procedures
LMCTs were performed in the morning after a 10-h overnight fast. An intravenous cannula was inserted, and the baseline (−30 and −20 min) venous blood sample was obtained. Five minutes prior to liquid meal challenge (Biosorb Energie®, Pfrimmer Nutricia, Erlangen, Germany) (36.8 g of carbohydrate, 11.6 g of fat, 12 g of protein, and 300 kcal per 200 mL), subjects were given, in accordance with the treatment period, 120 mg of nateglinide (Starlix®, Novartis Pharma, Nürnberg, Germany), 2 mg of repaglinide (NovoNorm®, NovoNordisk A/S, Mainz, Denmark), or placebo. Further venous and capillary blood samples were taken at 30, 60, 120, and 240 min after the ingestion of the liquid meal. Serum samples were collected and stored at −40°C until analysis. All samples were measured in duplicate.
Laboratory measurements
Capillary blood glucose concentrations were determined using a glucose oxidase method on a Dr. Müller GL glucose analyzer (Dr. Müller Gerätebau GmbH, Freital, Germany). Glycated hemoglobin (HbA1c) was determined using a Hi-Auto A1C HA-8140 system (Menarini Diagnostics, Berlin). Serum triglycerides, total cholesterol, and high-density lipoprotein (HDL)-cholesterol were determined by standard enzymatic assays (certified laboratory for clinical chemistry), and low-density lipoprotein (LDL)-cholesterol was calculated from these data. Serum insulin was measured using a commercial enzyme-linked immunosorbent assay (Insulin ELISA, Mercodia AB, Uppsala, Sweden). Human plasma ghrelin was measured as “total ghrelin” with a commercial radioimmunoassay (Phoenix Pharmaceuticals, Belmont, CA) that uses 125I-labeled bioactive ghrelin as a tracer molecule and a polyclonal antibody raised in rabbits against full-length octanoylated human ghrelin (intra-assay coefficient of variation, 4%). No cross-reactivity with human secretin, human vasoactive intestinal peptide, human galanin, human growth hormone-releasing hormone, neuropeptide Y, or other relevant molecules has been reported. 11
Calculations and statistical analysis
Data are presented as mean ± SE values. A comparison of demographic characteristics between the T2DM group and the control group without diabetes was performed with the Mann-Whitney test for nonparametric, unpaired variables. Insulin sensitivity was quantified using fasting glucose and insulin values with homeostasis model assessment (HOMAIR). 35 In the LMCT, an average of the two consecutive basal samples was calculated (−30 and −20 min) to reduce individual variation in basal levels of blood glucose and insulin. Time-averaged insulin and glucose responses were computed as incremental area under the curve (AUC) values (above baseline) using the trapezoidal rule, divided by the time interval (in h). Comparisons across different treatments were performed using the analysis of variance procedure with post hoc analysis using the Sidak adjustment. Spearman's correlation and simple linear regression analysis were used to examine the correlation among circulating insulin, blood glucose, and ghrelin levels. The ghrelin secretion pattern was analyzed by the nonparametric paired Wilcoxon test. All statistical analyses were performed using SPSS for Windows version 14.0 (SPSS Inc., Chicago, IL).
Results
Demographic and baseline characteristics of study groups are given in Table 1. In control subjects, no differences between age, BMI, HDL, LDL, triglycerides, and HOMAIR were found compared to the group with diabetes. As expected, HbA1c and fasting capillary blood glucose concentrations were lower and fasting insulin concentrations were higher in the group without diabetes. In subjects with T2DM, basal ghrelin concentrations correlated only with HbA1c (r = 0.51, P = 0.022), but not with BMI, age, duration of diabetes, HOMAIR, and concentrations of triglycerides, fasting insulin, and fasting blood glucose.
Data are mean ± SD values.
Group comparison by Mann-Whitney U test: *P < 0.05 for study group I versus study group II.
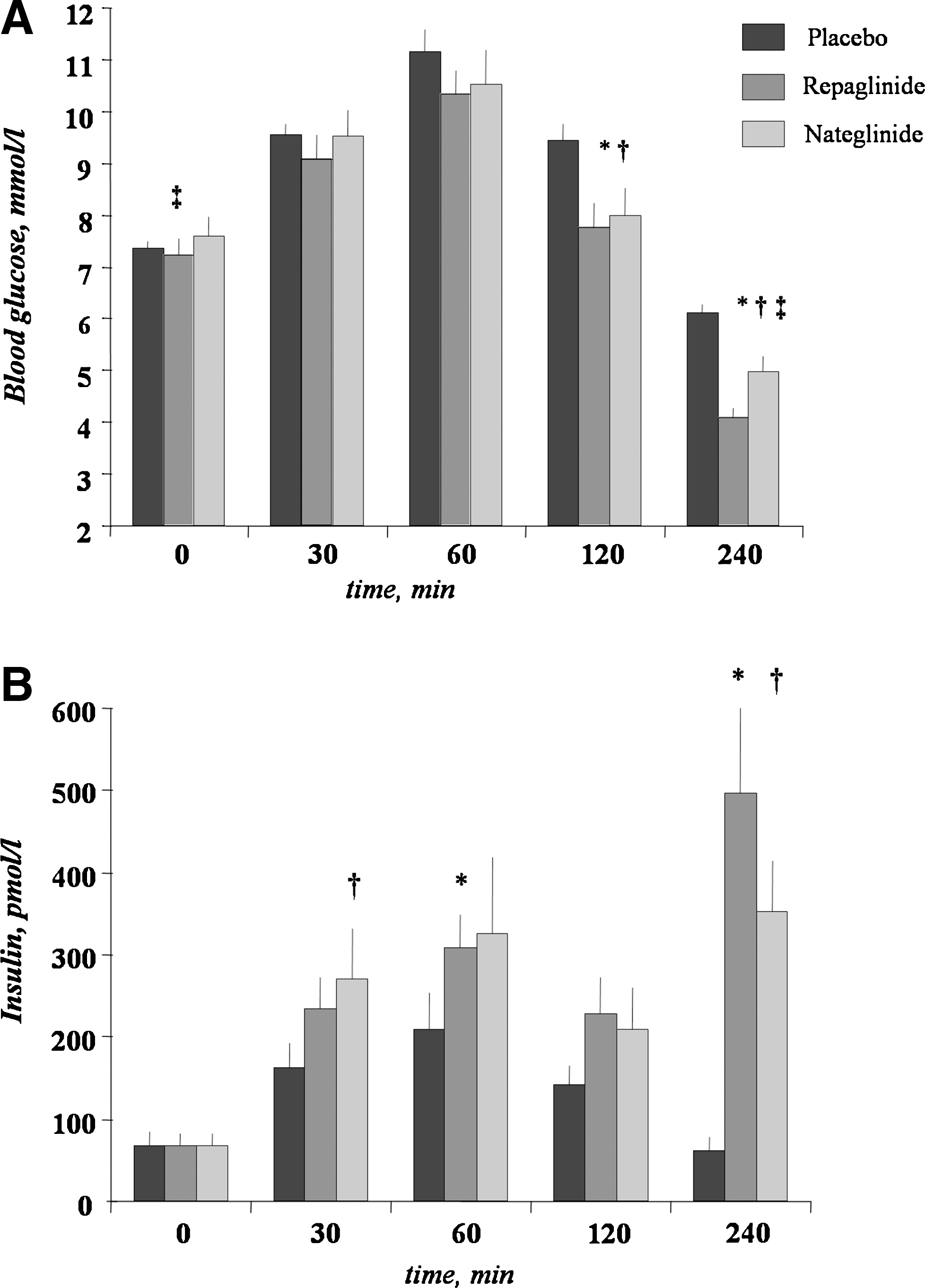
After 1 week of treatment, fasting blood glucose concentrations were lower for repaglinide compared with nateglinide, but not significantly different compared to placebo (Table 2). Incremental AUCs of postprandial blood glucose concentrations were significantly reduced by both drugs compared to placebo (Table 2). Blood glucose concentrations at 120 and 240 min of LMCT were lower with both drugs compared to placebo (P < 0.02) and at 240 min with repaglinide compared to nateglinide (P < 0.02; Fig. 2A). Basal insulin concentrations were unchanged during treatment with placebo or meglitinides (Table 2). Incremental AUCs of postprandial insulin concentrations were higher for repaglinide and nateglinide treatments compared to placebo (Table 2). Post-challenge insulin concentrations were higher at 30 min for nateglinide, at 60 min for repaglinide, and at 240 min for both meglitinides compared to placebo, but not different between these drugs (Fig. 2B).
(
Data are mean ± SD values.
P < 0.003 for the LMCTs with repaglinide and nateglinide versus tests with placebo, † P < 0.05 for the tests with repaglinide versus tests with nateglinide.
In the control subjects, ghrelin levels significantly decreased at 30 min and reached a nadir at 60 min after the liquid meal load (239.9 ± 22.8 pg/mL at baseline vs. 181.6 ± 15.8 pg/mL at 60 min, 22.9 ± 3.5% of baseline; P = 0.001; Fig. 3A). In the placebo-treated subjects with diabetes, no suppression of circulating ghrelin levels was observed in the LMCT (Fig. 3B). However, fasting and postprandial levels of ghrelin were not significantly different between patients with diabetes and control subjects. After administration of meglitinides, a nadir of serum ghrelin was observed at 60 min for repaglinide (197.8 ± 14.5 pg/mL at baseline vs. 180.7 ± 13.5 pg/mL, 8.6% of baseline; P = 0.038), and a trend to decrease of the circulating ghrelin concentration was detected at the same time for nateglinide (190.0 ± 16.7 pg/mL at baseline vs. 175.7 ± 14.9 pg/mL at 60 min, 7.5% of baseline; P = 0.081). Moreover, a subsequent increase of circulating ghrelin levels at 240 min after the meal was observed for both meglitinides (P = 0.016 for repaglinide, P = 0.002 for nateglinide; Fig. 2C and D) and was similar to the pattern in control subjects (Fig. 2A). Fasting and postprandial ghrelin concentrations were not significantly different among the three (placebo, repaglinide, and nateglinide) treatments. No correlation was demonstrated between ghrelin and insulin responses in the meal test with drug and placebo in patients with diabetes and in obese controls (data not shown).
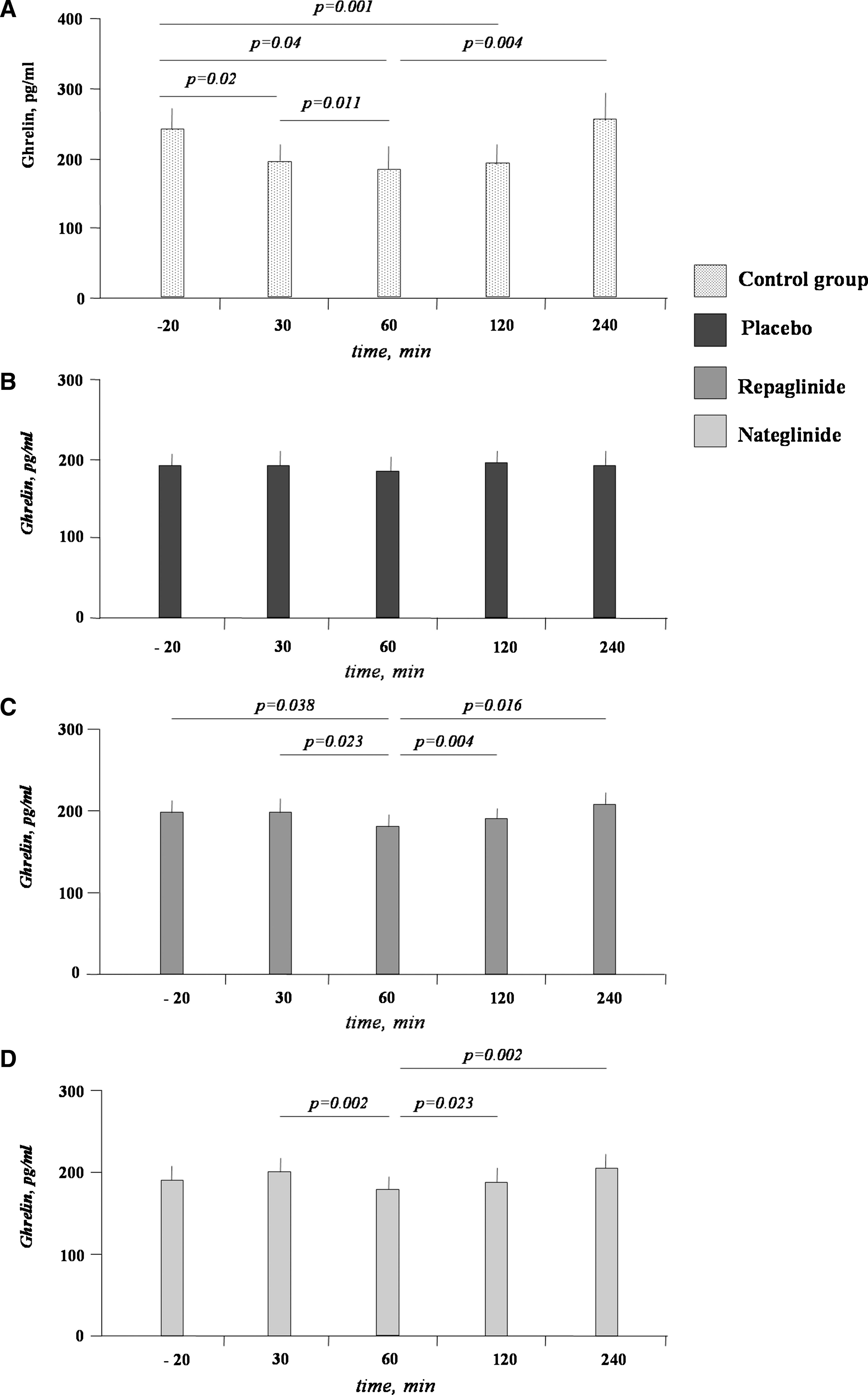
Patterns of postprandial ghrelin secretion in (
Discussion
The present data showed that, in contrast to healthy moderate obese subjects, patients with T2DM fail to suppress ghrelin after meal intake. Short-term treatment with meglitinides had no effect on the absolute values of fasting and postprandial ghrelin concentrations in subjects with T2DM. When changes in ghrelin levels were measured in the relation to basal values, we observed clearly reconstructions of the ghrelin secretion pattern with treatment with meglitinides. In the presence of both drugs, decrease in the postprandial ghrelin had a nadir at 60 min after the meal and was comparable to the ghrelin suppression pattern in subjects without diabetes. The observed effect of meglitinides on ghrelin secretion was independent from circulating glucose levels and insulin responses in these patients.
Ghrelin was reported to be down-regulated in common obesity, 10 and obese subjects did not exhibit a meal-induced decline in plasma ghrelin. 36 In our study, we clearly observed suppression of postprandial ghrelin levels after the meal load in obese control subjects. This difference from previously published reports may be explained by the rather moderate extent of obesity in our study. In contrast, the T2DM subjects with similar BMI had no meal-induced decrease of postprandial ghrelin levels in our study. Moreover, fasting ghrelin concentrations correlated significantly with HbA1c but not with BMI or other biochemical markers such as fasting glucose or insulin in the subjects with diabetes studied here.
Only limited data concerning the regulation of ghrelin secretion in T2DM have been published. 25,37 In the large cohort of obese patients with diabetes and subjects without diabetes, the meal-induced decrease of ghrelin levels was observed. 37 However, all subjects studied had newly diagnosed T2DM, and the ghrelin response was investigated in a solid meal test, which may explain differences compared to our data. Moreover, the insulin-induced ghrelin decrease was less pronounced in patients with T2DM during the euglycemic clamp. 25 Given the orexigenic property of ghrelin, the meal-induced fall of circulating ghrelin concentrations could well limit the intake of additional food. 38 Thus, the impaired suppression of circulating ghrelin during the meal intake in subjects with T2DM might contribute and possibly account for the ongoing weight gain in T2DM.
A novel finding of our study was the reconstruction of the postprandial ghrelin secretion pattern after short-term treatment with meglitinides in T2DM subjects. We observed a suppression of ghrelin at 60 min of the LMCT after treatment with repaglinide, but only the trend to a decrease in ghrelin levels at 60 min of the LMCT with nateglinide. This finding is consistent with the ghrelin secretion pattern in healthy individuals, in which ghrelin levels fall to baseline levels between 60 and 120 min after eating. 25 Mechanisms of how meglitinides may affect ghrelin secretion require further investigation. The gastrointestinal endocrine cells consist of two cell types: opened-type cells, which are in contact with the glandular lumen, and closed-type cells, which do not have a luminal connection. 39 In the oxyntic mucosa of the stomach, ghrelin-producing cells show no connection with the lumen, 40 and a possible modulation of ghrelin secretion by hormones, neuronal stimulation, or mechanical distension has been suggested. 39 Repaglinide and nateglinide are structural relatives of meglitinide, the nonsulfonylurea moiety of glibenclamide. 29 Both drugs, in common with sulfonylureas, act via the closure of ATP-sensitive potassium channels in pancreatic β-cells, 41 but the binding site and molecular kinetics of nateglinide and repaglinide differ considerably. 42 Both drugs also bind to similar channels in other tissues. ATP-sensitive potassium channels have important functions in neuroendocrine tissue, in smooth and skeletal muscle, and in the heart. 43 Repaglinide was reported to inhibit recombinant ATP-sensitive potassium channels of β-cells, cardiomyocytes, and nonvascular smooth muscle, 44 and nateglinide stimulates growth hormone release. 45 Similarly, nateglinide was shown to enhance glucagon release in contrast to repaglinide. 46
Native gastric ATP-sensitive potassium channels are present in oxyntic cells and gastric mucosal membrane 31 and were shown to interact with tolbutamide. 32,33 Whether ATP-sensitive potassium channels are involved in the regulation of ghrelin secretion or ghrelin production is still unclear. For example, a greater glucose flux/uptake by X/A-like ghrelin-producing cells under meglitinides might be responsible for the inhibition of intracellular ghrelin synthesis and/or secretion. Another possible mechanism is the modulation of insulin sensitivity of the X/A-like ghrelin-producing cells by meglitinides. Regarding the skeletal muscle, a role of meglitinides in the regulation of insulin sensitivity was proposed that appears to be directly related to the regulation of potassium channels in this tissue. 47 In healthy subjects, the close relationship between insulin sensitivity to glucose and ghrelin suppression was observed. 23
As a result of the study design, we cannot entirely exclude that effects observed here are independent from the metformin action. Of the two already published studies regarding the effect of metformin on ghrelin levels in T2DM, one showed a prolongation of the decrease of postprandial ghrelin levels, 26 and the second study observed a decrease of postprandial ghrelin levels during the OGTT. 28 In our study, a placebo control was analyzed 3 weeks after the high-dose metformin treatment, and we observed no suppression of ghrelin in the LMCT in subjects with diabetes. In contrast, the decrease of post-meal ghrelin concentration was observed after only 1 week of treatment with repaglinide. It should be pointed out that fasting and postprandial concentrations of ghrelin were not significant different among the three treatments by the comparison of absolute values. Moreover, we observed no differences in the fasting or postprandial concentrations of ghrelin between control subjects and patients with diabetes. The question whether meglitinides in combination with metformin or as a monotherapy may be useful to avoid the weight gain in T2DM requires the further investigation on the large cohort or meta-analysis of published data. In the two large clinic studies, no effects on body weight were observed for repaglinide and nateglinide compared to placebo during the period of 4 and 8 months, respectively. 48,49
Some limitations of this study should be mentioned. In our crossover study including 20 subjects with T2DM, we were able to detect an effect size (f) of 1/4 standard deviation (s) of a quantitative trait with a power of 98%. Effect sizes of 1/10 s were still detected only with 28% power. 50 Thus, given the observed differences in the ghrelin responses between treatments, our study was underpowered to detect the strong significantly effect of meglitinides on ghrelin secretion, and our data require further replication in a larger cohort of subjects with T2DM.
Taken together, short-term treatment with meglitinides reconstructs the postprandial ghrelin secretion pattern in subjects with T2DM and may help to improve the control of body weight in subjects with T2DM. Observed effects were independent from the circulating insulin and/or glucose levels.
Footnotes
Acknowledgments
This work was sponsored by NovoNordisk AG, Mainz, Germany.
Author Disclosure Statement
The authors declare that there is no duality of interest associated with this article.