
Abstract
Background:
Incretin-based therapies have provided additional options for the treatment of type 2 diabetes mellitus. The aim of our study was to evaluate the effects of exenatide compared to glibenclamide on body weight, glycemic control, β-cell function, insulin resistance, and inflammatory state in patients with diabetes.
Methods:
One hundred twenty-eight patients with uncontrolled type 2 diabetes mellitus receiving therapy with metformin were randomized to take exenatide 5 μg twice a day or glibenclamide 2.5 mg three times a day and titrated to exenatide 10 μg twice a day or glibenclamide 5 mg three times a day. We evaluated body weight, body mass index (BMI), glycated hemoglobin (HbA1c), fasting plasma glucose (FPG), postprandial plasma glucose (PPG), fasting plasma insulin (FPI), homeostasis model assessment insulin resistance (HOMA-IR) index, homeostasis model assessment β-cell function (HOMA-β) index, plasma proinsulin (PPr), PPr/FPI ratio, resistin, retinol binding protein-4 (RBP-4), and high-sensitivity C-reactive protein (Hs-CRP) at baseline and after 3, 6, 9, and 12 months.
Results:
Body weight and BMI decreased with exenatide and increased with glibenclamide. A similar improvement of HbA1c, FPG, and PPG was obtained in both groups, whereas FPI decreased with exenatide and increased with glibenclamide. The HOMA-IR index decreased and the HOMA-β index increased with exenatide but not with glibenclamide. A decrease of PPr was reported in both groups, but only glibenclamide decreased the PPr/FPI ratio. Resistin and RBP-4 decreased with exenatide and increased with glibenclamide. A decrease of Hs-CRP was obtained with exenatide, whereas no variations were observed with glibenclamide.
Conclusions:
Both exenatide and glibenclamide gave a similar improvement of glycemic control, but only exenatide gave improvements of insulin resistance and β-cell function, giving also a decrease of body weight and of inflammatory state.
Introduction
Glibenclamide is a well-known second-generation sulfonylurea, and like all sulfonylureas, it binds a specific site on the ATP-sensitive potassium channels, subsequently opening calcium channels and thus triggering insulin exocytosis from the pancreatic β-cell. 15
The aim of this study was to evaluate the effects of a 1-year treatment with exenatide compared to glibenclamide in type 2 diabetes patients on body weight, glycemic control, and β-cell function but also on insulin resistance and inflammatory state parameters like resistin, retinol binding protein-4 (RBP-4), and high-sensitivity C-reactive protein (Hs-CRP).
Subjects and Methods
Study design
This multicenter, randomized, single-blind, controlled study was conducted at the Department of Internal Medicine and Therapeutics, University of Pavia, Pavia, Italy; the “G. Descovich” Atherosclerosis Study Center, Department of Internal Medicine, Aging and Kidney diseases, University of Bologna, Bologna, Italy; the Diabetes Care Unit, S. Carlo Hospital, Milano, Italy; the Pesenti Fenaroli Hospital, Alzano Lombardo, Bergamo, Italy; the Metabolic Unit, Regional Hospital, Varese, Italy; the Division of Medicine, Civic Hospital, Cittiglio, Varese, Italy; the RSA Don Leone Porta, Milano; and the Fondazione Ospedale della Carità, Casalbuttano, Cremona, Italy.
The study protocol was approved at each site by institutional review boards and was conducted in accordance with the Declaration of Helsinki and its amendments.
Patients
We enrolled 128 white type 2 diabetes patients ≥18 years old of either sex (Table 1) according to the European Society of Cardiology and European Association for the Study of Diabetes guidelines criteria, 16 with poor glycemic control (expressed as HbA1c level >8.0%) and overweight (body mass index [BMI] ≥25 and <30 kg/m2) receiving therapy with metformin at the mean dosage of 1,500 ± 500 mg/day. They were intolerant to metformin at maximum dosage (3,000 mg/day) with the onset of gastrointestinal disorders like diarrhea and significant meteorism when metformin was titrated to the maximum level.
Data are mean ± SD values.
Suitable patients, identified from review of case notes and/or computerized clinic registers, were contacted by the investigators in person or by telephone.
Patients were excluded if they had a history of ketoacidosis or had unstable or rapidly progressive diabetic retinopathy, nephropathy, or neuropathy, impaired hepatic function (defined as plasma aminotransferase and/or γ-glutamyltransferase level higher than the upper limit of normal for age and sex), impaired renal function (defined as serum creatinine level higher than the upper limit of normal for age and sex), or severe anemia. Patients with serious cardiovascular disease (e.g., New York Heart Association class I–IV congestive heart failure or a history of myocardial infarction or stroke) or cerebrovascular conditions within 6 months before study enrollment also were excluded. Women who were pregnant or breastfeeding or of childbearing potential and not taking adequate contraceptive precautions were also excluded. All patients provided written informed consent to participate.
Treatments
Patients were assigned to receive exenatide 5 μg twice a day or glibenclamide 2.5 mg three times a day and titrated after 1 month to exenatide 10 μg twice a day or glibenclamide 5 mg three times a day for 12 months in a randomized, single-blind, controlled study. Randomization was done using a drawing of envelopes containing randomization codes prepared by a statistician. Medication compliance was assessed by counting the number of pills or syringes returned at the time of specified clinic visits. Throughout the study, we instructed patients to take their first dose of new medication on the day after they were given the study medication. At the same time, all unused medication was retrieved for inventory. All medications were provided free of charge.
Diet and exercise
Subjects began a controlled-energy diet (near 600 kcal daily deficit) based on American Heart Association recommendations 17 that included 50% of calories from carbohydrates, 30% from fat (6% saturated), and 20% from proteins, with a maximum cholesterol content of 300 mg/day and 35 g/day of fiber. Patients were not treated with vitamins or mineral preparations during the study.
Standard diet advice was given by a dietitian and/or specialist doctor. Dietitian and/or a specialist doctor periodically provided instruction on dietary intake recording procedures as part of a behavior modification program and then later used the subject's food diaries for counseling. Individuals were also encouraged to increase their physical activity by walking briskly for 20–30 min, three to five times per week, or by cyclette. The recommended changes in physical activity throughout the study were not assessed.
Assessments
Before starting the study, all patients underwent an initial screening assessment that included a medical history, physical examination, vital signs, a 12-lead electrocardiogram, and measurements of BMI, HbA1c, fasting plasma glucose (FPG), postprandial plasma glucose (PPG), and fasting plasma insulin (FPI). Insulin resistance and β-cell function were evaluated by the homeostasis model assessment method; in particular, we considered the homeostasis model assessment insulin resistance (HOMA-IR) index and the homeostasis model assessment β-cell function (HOMA-β) index. We evaluated body weight and BMI, HbA1c, FPG, PPG, FPI, HOMA-IR, HOMA-β, plasma proinsulin (PPr)/FPI ratio, resistin, RBP-4, and Hs-CRP. We measured these parameters at baseline and after 3, 6, 9, and 12 months. In order to evaluate the tolerability assessments, all adverse events were recorded. All plasma parameters were determined after a 12-h overnight fast with the exception of PPG, which was determined 2 h after a standardized meal. Venous blood samples were taken for all patients between 0800 and 0900 h. We used plasma obtained by addition of disodium EDTA (1 mg/L) and centrifuged at 3,000 g for 15 min at 4°C. Immediately after centrifugation, the plasma samples were frozen and stored at −80°C for no more than 3 months. All measurements were performed in a central laboratory.
BMI was calculated as weight in kilograms divided by the square of height in meters. HbA1c level was measured by a high-performance liquid chromatography method (DIAMAT, Bio-Rad, Hercules, CA, USA) (normal values, 4.2–6.2%), with intra- and interassay coefficients of variance of <2%. 18 Plasma glucose was assayed by the glucose oxidase method (GOD/PAP, Roche Diagnostics, Mannheim, Germany) with intra- and interassay coefficients of variance of <2%. 19 Plasma insulin was assayed with the Phadiaseph insulin radioimmunoassay (Pharmacia, Uppsala, Sweden) by using a second antibody to separate the free and antibody-bound 125I-insulin (intra- and interassay coefficients of variance, 4.6% and 7.3%, respectively). 20
The HOMA-IR index was calculated as the product of basal glucose (in mmol/L) and insulin levels (in μU/mL) divided by 22.5. 21,22 The HOMA-β index was calculated as the product of 20 and basal insulin levels (in μU/mL) divided by the value of basal glucose concentrations (in mmol/L) minus 3.5; this formula has been proposed to be a good measure of β-cell function. 22
Proinsulin was determined using an enzyme-linked immunosorbent assay (Mercodia, Uppsala). The intra- and interassay coefficients of variance were 2.4% and 8.9%, respectively. 23
The resistin value was measured by a commercially available enzyme-linked immunoassay kit (BioVendor Laboratory Medicine, Brno, Czech Republic). The intra-assay coefficient of variance was 3.4%, and the interassay coefficient of variance was 6.9%. 24
RBP-4 was measured using an RBP-4 (human) enzyme immunoassay kit (Phoenix Pharmaceuticals, Inc., Burlingame, CA). The intra- and interassay coefficients of variance were <5.0% and <14.0%, respectively. 25
Hs-CRP was measured with use of latex-enhanced immunonephelometric assays on a BN II analyzer (Dade Behring, Newark, DE). The intra- and interassay coefficients of variance were 5.7% and 1.3%, respectively. 26
Statistical analysis
Every patient who had received at least one dose of the study medication underwent a tolerability observation to exclude the presence of acute adverse reactions. After that an intention-to-treat analysis was conducted in patients who had received one or more doses of study medication, did not show any acute adverse reaction, and had a subsequent efficacy observation. Continuous variables were compared by analysis of variance. Intervention effects were adjusted for additional potential confounders using analysis of covariance. Annalysis of variance was also used to assess the significance within and between groups. The statistical significance of the independent effects of treatments on the other variables was determined using analysis of covariance. A one-sample t test was used to compare values obtained before and after treatment administration; two-sample t tests were used for between-group comparisons. The Bonferroni correction for multiple comparisons was also carried out. 27 Statistical analysis of data was performed using the Statistical Package for Social Sciences software version 11.0 (SPSS Inc., Chicago, IL). Data are presented as mean ± SD values. For all statistical analyses, P < 0.05 was considered statistically significant.
Results
Study sample
A total of 128 patients were enrolled in the study. Of these, 116 completed the study, and 59 (50.8%) were allocated to the exenatide group and 57 (49.2%) to the glibenclamide group. There were 12 patients (five men and seven women) who did not complete the study, and the reasons for premature withdrawal included side effects as nausea (two women in the exenatide group, one woman in the glibenclamide group, and one man in the glibenclamide group, after 3 months), diarrhea (one man and one woman in the exenatide group and one man in the glibenclamide group, after 6 months), vomiting (one woman in the glibenclamide group, after 12 months), and lost to follow-up (one man in the glibenclamide group, after 12 months). Moreover, one woman had hypoglycemia (FPG <60 mg/dL) in the glibenclamide group after 3 months, one woman in the glibenclamide group after 9 months, and one man in the glibenclamide group at 12 months. The characteristics of the patient population at study entry are shown in Table 1.
Body weight and BMI
At the end of the study there was a statistically significant decrease of body weight and BMI compared to baseline with exenatide, whereas there was a significant increase with glibenclamide. Furthermore, the body weight and BMI values obtained with exenatide were significantly lower than the values obtained with glibenclamide after 6, 9, and 12 months (Tables 2 and 3).
Data are mean ± SD values.
P < 0.05, **P < 0.01, ***P < 0.001 versus baseline; † P < 0.05, †† P < 0.01, ††† P < 0.001 versus glibenclamide.
Data are mean ± SD values.
P < 0.05, **P < 0.01, ***P < 0.001 versus baseline.
Glycemic parameters
After 12 months we observed a statistically significant improvement of HbA1c, FPG, and PPG compared to baseline in both groups without any significant differences between the two groups. In contrast, the FPI value was significantly decreased compared to baseline after 9 and 12 months of therapy with exenatide, whereas it was significantly increased with glibenclamide. Furthermore, the FPI value obtained with exenatide was significantly lower than the value obtained with glibenclamide after 9 and 12 months.
β-Cell function
The HOMA-β index increased after 9, and 12 months compared to baseline with exenatide, whereas there were no statistically significant variations with glibenclamide. At the end of the study the HOMA-β index observed with exenatide was significantly higher than the value recorded with glibenclamide.
There was a similar decrease of PPr after 9 and 12 months compared to baseline in both groups, although we observed a significant decrease of PPr/FPI ratio with glibenclamide but not with exenatide. The PPr/FPI ratio obtained with exenatide was significantly higher than the value recorded with glibenclamide after 9 and 12 months (Tables 2 and 3).
Insulin resistance parameters
A statistically significant decrease of HOMA-IR index was recorded after 9 and 12 months compared to baseline with exenatide, whereas we did not observe any statistically significant variations with glibenclamide. Furthermore, the HOMA-IR index obtained with exenatide was significantly lower than the value obtained with glibenclamide after 9 and 12 months (Tables 2 and 3).
Resistin and RBP-4 values were significantly decreased after 6, 9, and 12 months compared to baseline with exenatide, whereas they increased with glibenclamide after 12 months. Moreover, resistin and RBP-4 value obtained with exenatide were significantly lower than the values recorded with glibenclamide after 9 and 12 months (Tables 2 and 3).
Inflammatory state
A significant decrease of Hs-CRP value was obtained after 6, 9, and 12 months compared to baseline with exenatide, whereas there were no statistically significant variations with glibenclamide. Furthermore, the Hs-CRP value obtained with exenatide was significantly lower than the value observed with glibenclamide after 12 months (Tables 2 and 3).
Correlations
There was a significant correlation between BMI value decrease and RBP-4 (r = 0.64, P < 0.001) (Fig. 1) and resistin decrease (r = 0.59, P < 0.001) in the exenatide group after 12 months of therapy (Fig. 2). In contrast, there was no correlation between RBP-4 or resistin with BMI in the group treated with glibenclamide.
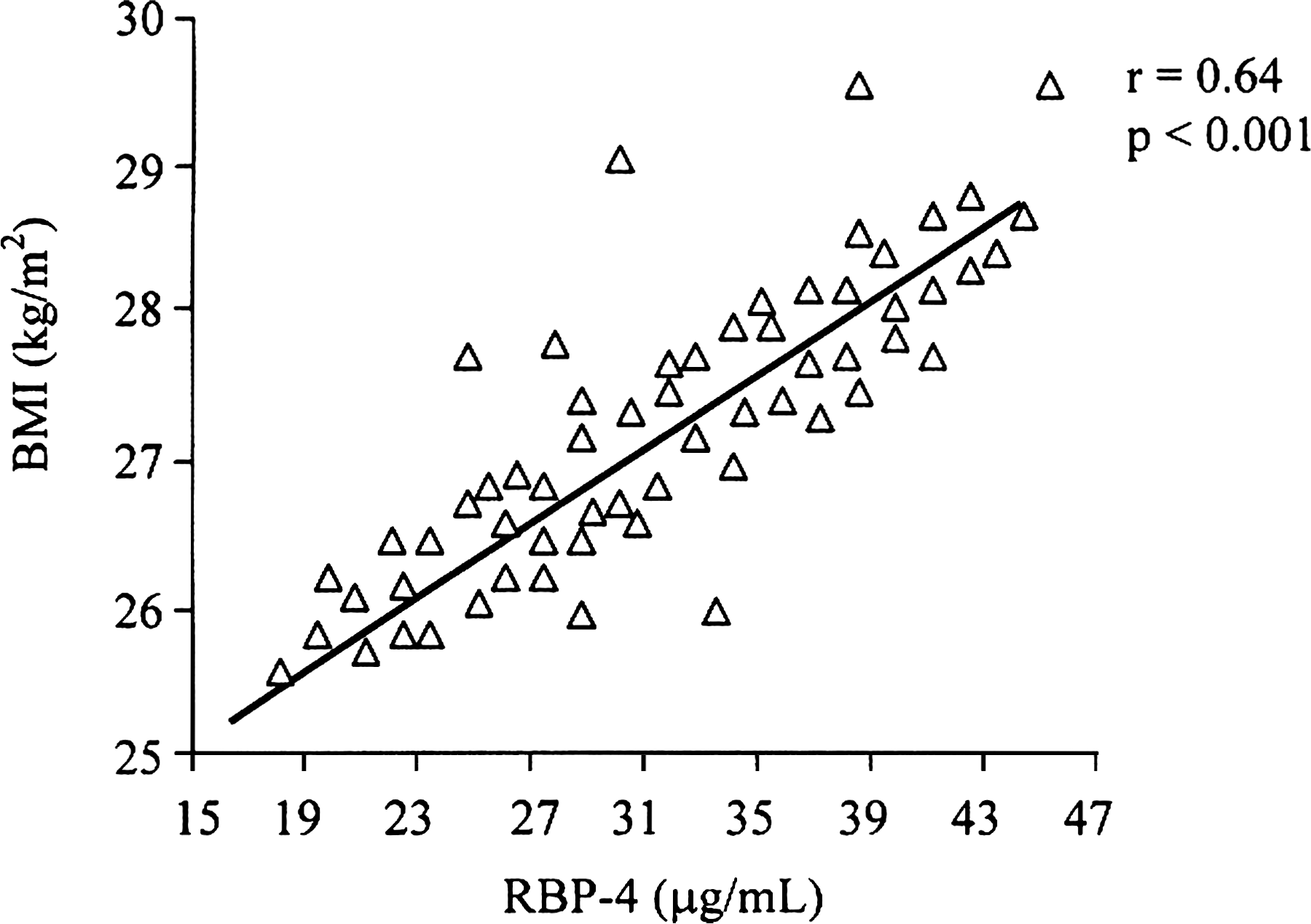
Correlation between BMI and RBP-4 after 12 months of exanatide treatment.
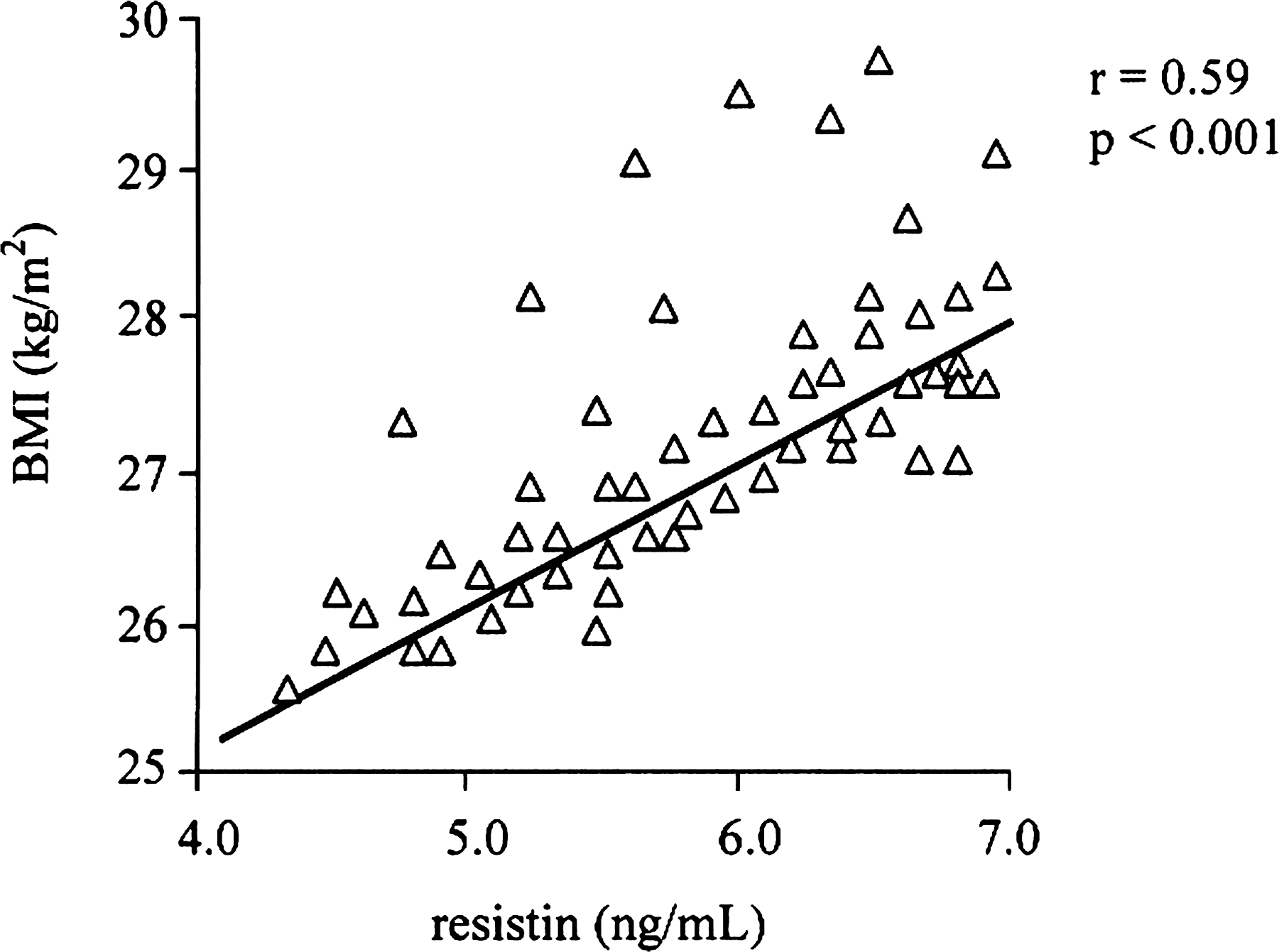
Correlation between BMI and resistin after 12 months of exanatide treatment.
Discussion
Results from three large 30-week trials testing the addition of exenatide to metformin alone, 10 sulfonylurea alone, 11 or metformin and sulfonylurea together 12 as well as three trials that compared exenatide with insulin glargine or biphasic insulin 28 –30 are available in the literature. A reduction from baseline levels of approximately 1.0% in HbA1c was noted in all trials, whereas weight decreased by 0.9–2.5 kg, depending on the study. The data emerging from our study showed that both exenatide and glibenclamide gave a similar improvement of glycemic control, improving HbA1c, FPG, and PPG, even if exenatide had more positive effects compared to glibenclamide on body weight, β-cell function, insulin resistance, and inflammation state. We observed that after 12 months of treatment there was a body weight decrease of 8.0 kg with exenatide and an increase of 4.3 kg with glibenclamide, partially confirming what already reported by the United Kingdom Prospective Diabetes Study about sulfonylureas giving a weight gain of about 5 kg over 10 years. 31 We observed a greater decrease in body weight with exenatide compared to the previously reported studies, probably because we placed diet and exercise therapy as a high priority. Furthermore, the previously reported studies lasted 30 weeks, whereas our study lasted 52 weeks; the greater weight loss we observed can also be partially due to the continued weight loss of patients on exenatide between 30 and 52 weeks. The positive effects showed by exenatide on body weight need to be underlined because despite the emphasis placed on weight loss in the management of T2DM and the association of excess weight with poorer metabolic control and cardiovascular risk profile, many antidiabetes treatments are associated with weight gain. 32 Insulin treatment, for example, is typically associated with an increase in weight, and, with the exception of metformin and acarbose, oral agents are also responsible for a certain degree of weight gain. It has been already reported in the literature that obesity worsens hyperglycemia, hyperinsulinemia, insulin resistance, and dyslipidemia 33 ; obesity is also a risk factor for nonalcoholic fatty liver disease, hypertension, and cardiovascular disease, 34,35 and reducing body weight with exenatide has positive effects also on these factors.
Regarding insulin resistance and β-cell function parameters, it has been observed that a high HOMA-IR index and a low HOMA-β index were independently and consistently associated with an increased diabetes risk in a multiethnic cohort of U.S. post-menopausal women. 36 Furthermore, in T2DM patients the HOMA-β index was reduced compared to the normal glucose tolerance subjects, in which the HOMA-IR index was increased. Also, both the fasting PPr concentration and the ratio of fasting PPr/FPI of the T2DM patients were significantly higher compared to normal glucose tolerance subjects 37 because of the defective conversion of proinsulin to insulin. Data from our study showed that exenatide gave a decrease of HOMA-IR index, an increase of HOMA-β index, a decrease of FPI, and a decrease of PPr, confirming what has already been reported in the literature 10 –13 that exenatide improved the insulin resistance and protected β-cell function. Moreover, PPr has also been demonstrated to be an independent cardiovascular risk factor by stimulating plasminogen activator inhibitor-1 secretion and blocking fibrinolysis 38 ; exenatide, by reducing PPr levels, might also give a decrease of cardiovascular risk.
Our data confirmed what has already been reported by Moretto et al. 39 : exenatide was associated with an improvement of HbA1c, fasting and postprandial glucose control, and β-cell function (HOMA-β index), with a reduction of body weight, and was well tolerated. Compared to the other studies reported in literature, our study also showed the positive effects of exenatide on insulin resistance and inflammatory state parameters like resistin, RBP-4, and Hs-CRP. We observed an increase of resistin and RBP-4 in the glibenclamide group, wheres there was a decrease of resistin, RBP-4, and Hs-CRP in patients treated with exenatide. In humans, resistin is produced by mononuclear cells and activated macrophages; it has been demonstrated that overexpression of resistin decreases the ability of insulin to suppress hepatic glucose output or increase glucose uptake by muscle. 40 –42 Available data support also a role of resistin in determining an increase of inflammation and atherosclerosis. 43 Also, RBP-4 concentration has been reported to be increased in subjects with obesity, insulin resistance, or type 2 diabetes compared with lean subjects, 44 even if the mechanisms by which RBP-4 induces insulin resistance are not well understood. Hs-CRP is a marker of inflammation, which has been shown in several prospective studies to independently predict myocardial infarction, stroke, and peripheral artery disease. 45 Exenatide decreased resistin, RBP-4, and Hs-CRP; considering what is reported above about these parameters, we can safely assume that their improvement can be related to a reduction of inflammatory state, atherosclerosis, and insulin resistance in patients with diabetes.
Regarding adverse reactions to exenatide, nausea and gastrointestinal complaints were the most common side effects reported in literature 10 –13 and were often temporary in nature; in our study there were no statistically significant differences between the exenatide and glibenclamide groups.
Of course, our study has some limitations: for example, we did not evaluate if the beneficial effects on β-cell function, glycemic control, body weight, and inflammatory parameters were sustained after the cessation of therapy, even if it has already been reported 46 that active treatment is necessary to maintain these beneficial effects of exenatide in patients in whom oral blood glucose-lowering therapy has failed. Another limitation is that we evaluated a limited number of inflammation biomarkers, concentrating our attention on a few of these. However, at the best of our knowledge, this is the first study investigating the effect of exenatide on inflammation parameters.
Conclusions
Both exenatide and glibenclamide gave a similar improvement of glycemic control, but only exenatide was associated with improvements in measures of insulin resistance and preserved β-cell function, giving also a decrease of body weight and a decrease of some inflammatory parameters. We can safely say that exenatide was effective and well tolerated in patients with T2DM compared to glibenclamide.
Footnotes
Author Disclosure Statement
The authors certify that they have no affiliation with, or financial involvement in, any organization or entity with a direct financial interest in the subject matter or materials discussed in the article.