
Abstract
Although European groups have initiated innovative clinical research in the field of insulin pump therapy, insulin pump use remains currently limited in many European countries, and well behind that in the United States. The main reason is the late approval of cost coverage by most national healthcare insurance systems, which is still lacking in some countries. Partly in connection with this delay, the number of trained physicians to pump therapy is low in many countries, while diabetes educators do not exist as an acknowledged entity in many European countries, and pump manufacturers are excluded from the education process of patients in most of them. Pump use in pediatric-age populations has strongly increased during the last years, following the evidence-based demonstrations of the benefits of pump therapy in these patients leading to an international consensus on pump indications and practice. Failure to control type 1 diabetes to target and frequent hypoglycemia under multiple daily insulin injections are consensus-based but restrictive indications for pump therapy in adults in most countries. The economic burden on healthcare insurance systems does not facilitate wider use of insulin pumps, but a significant expansion of pump therapy according to consensus-based indications is still expected thanks to the growing knowledge of physicians in technologies and because of the increasing interest of patients to use technology to improve their control of diabetes and health-related quality of life. More sophisticated technologies connected to pump therapy, such as continuous glucose monitoring or telemedicine, will need specific cost coverage for a true implementation in diabetes care in Europe.
Introduction
Current Clinical Use of Insulin Pumps in Europe
As shown in Figure 1, the analysis of the percentage of type 1 diabetes patients treated by insulin pumps in Europe can lead to identification of three groups of countries according to the penetration of this therapy. The first group includes Nordic, Central, and Western countries where insulin pumps are used by 15–20% of type 1 diabetes patients. A second group comprises countries at various locations in the continent where pumps are used by 5–10% of such patients. A third group gathers another heterogeneous bunch of countries in which close to or less than 5% of type 1 diabetes patients are treated by insulin pumps.
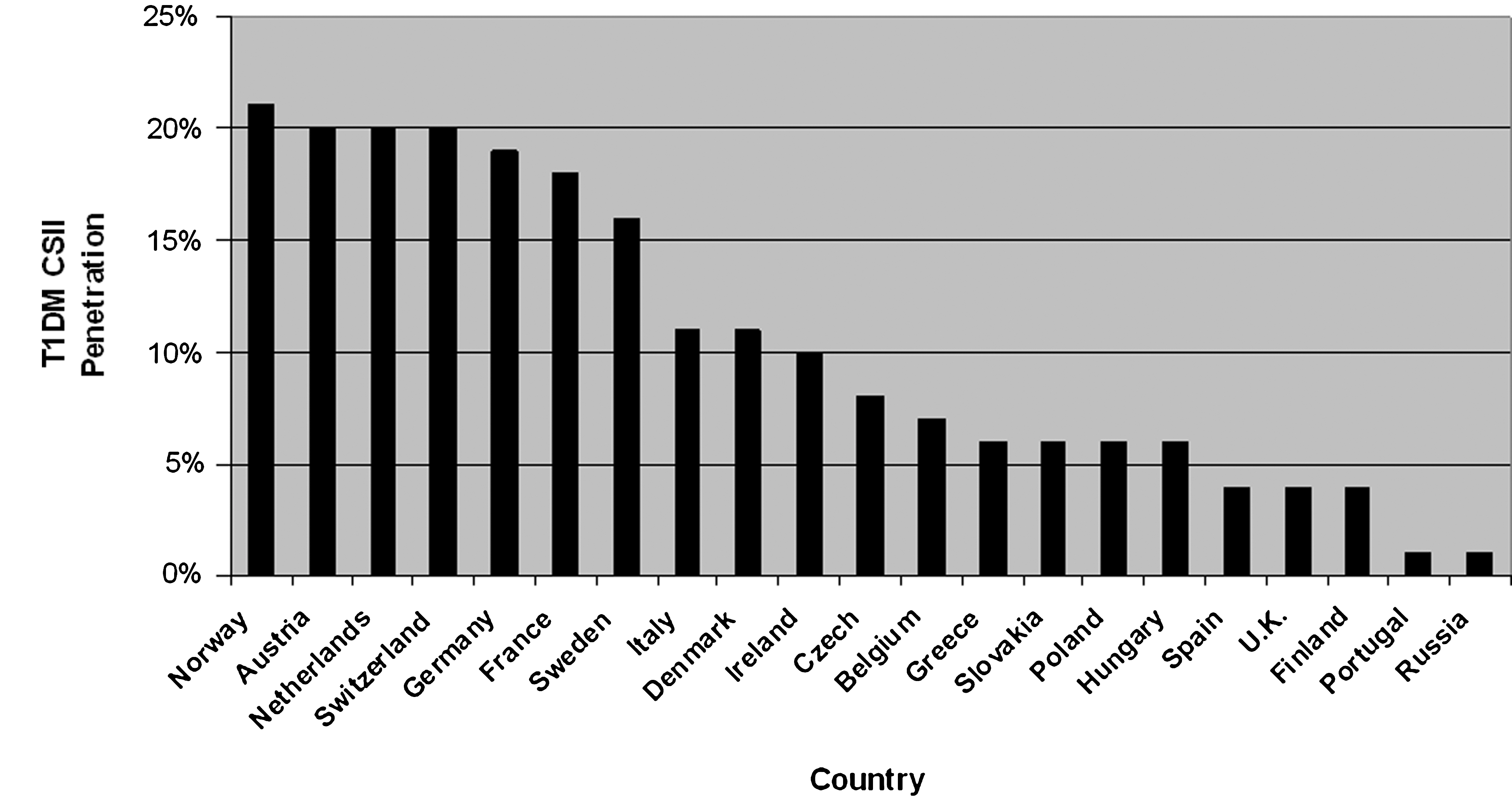
Penetration rates of continuous subcutaneous insulin infusion (CSII) therapy in patients with type 1 diabetes mellitus (T1DM) in European countries.
Analysis of Factors Determining Pump Use in Europe
The disparity of pump use in Europe can be explained mainly by the time when reimbursement of the technique has been obtained and, if it is still lacking, by this non-reimbursement status. By now, in Western Europe, only Belgium, Portugal, and Finland still face some limitations in the funding of pumps and consumables by the healthcare coverage systems. Nordic and German-speaking countries as well as The Netherlands initiated quite early reimbursement for pump therapy, in the 1980s or 1990s; France obtained it from 2000. Italy and Denmark have gotten full reimbursement in the 2000s. The United Kingdom and Spain also obtained it, barely, by this later period. Eastern Europe has obtained insurance coverage in its wealthiest part (Greece, the Czech Republic, Hungary, Slovenia, Slovakia, Lithuania), whereas reimbursement is still not available in Poland, Romania, Bulgaria, Croatia, Serbia, and Russia.
Although Western Europe has been well covered by reimbursement for many/several years, including close to or more than 10 years in some countries, it is noticeable that (1) the higher users are still behind the United States and (2) some significant heterogeneity remains about pump penetration among the various countries. Both the European mode of healthcare delivery and medical behaviors toward the technique are likely involved in these two phenomena. The physicians are still the main driving force of healthcare delivery in most European countries, including education to treatment use. Diabetes educators, as a specific entity of healthcare givers, are still lacking in many countries in Europe. This means that a huge amount of time must be dedicated by European physicians to the teaching and follow-up of diabetes patients treated by pumps. Enrollment of new patients may be dramatically slowed by the limited time that can be available for this task. Hence, even motivated pump recruiters cannot expand at high pace their population of patients treated by pumps unless they benefit from a dedicated and trained nursing team. Besides, manufacturers are in most countries not allowed and/or welcomed to interfere in the process leading to pump therapy, contrary to U.S. practice. Advertising for pumps is forbidden, as for any prescription drug, in most countries; participation of manufacturers in the education of the patients is generally neither allowed nor admitted. A further slowing mechanism of pump prescription in the countries where reimbursement has been allocated for less than 10 years comes from the lack of trained physicians to pump use and follow-up. It has become the habit of many physicians to exclude insulin pump therapy as a common practice. Besides the possible remaining suspicions about the true usefulness of a treatment mode that took a long time to be approved, the intellectual effort and the time needed to become a trained educator to pump use may not be considered as a priority, or even as possible because of the already heavy burden the physicians have to face in many European countries following shortages in the physician population.
A noticeable recent expansion of pump use in Europe can be underscored in children with diabetes. This phenomenon may be explained by the fact that the randomized studies investigating the benefits of insulin pumps versus multiple daily insulin injections (MDI) using only fast- and long-acting analogs have led to clearer conclusions in favor of pump therapy than in adult populations. 7,8 Pump experience in children and adolescents, shared by U.S. and European pediatricians, has also led to a consensus statement that establishes clear rules of pump use and rather globally supports pump use in the pediatric-age population. 9
Such an international consensus has not been reached for adults in Europe, although many views on indications and contraindications of insulin pumps are shared according to national recommendations. The failure to reach diabetes control by MDI therapy used with an appropriate education and follow-up is considered by all European diabetologists as the main indication for considering pump therapy. Of note is that the hemoglobin A1c threshold that should lead to consider pump use is, however, somewhat different between countries: 7.5% in France versus 8.5% in the United Kingdom. 10,11 Frequent disabling hypoglycemia is also acknowledged as a good indication for pump use. Because of the lack of strong scientific evidence, other indications such as the dawn phenomenon, blood glucose variability, unpredictable variations of insulin needs, pregnancy, allergy to insulin, and strong insulin resistance in type 2 diabetes patients are more controversial reasons for pump use according to the experts of different countries. An international survey published in the early 2000s, in which mainly German patients were recruited, showed that “looking for a more flexible lifestyle” was a key reason supporting the choice of pump therapy. 12 Cost-effectiveness of continuous subcutaneous insulin infusion has been investigated versus MDI in at least two U.K. studies. 13,14 Interestingly, both were in favor of pump therapy, but the results were mainly influenced by expected benefits in hemoglobin A1c levels, hence, reduced risk of long-term diabetes complications, and by the reduction in hypoglycemic events requiring medical intervention. Taking the option of pump therapy with no significant expectation of hemoglobin A1c improvement and/or reduction of disabling hypoglycemia would significantly minimize cost-effectiveness of pump therapy, even if quality of life would be better, as shown by other studies. 15,16 As a consequence, reimbursement of pump therapy according to the National Institute for Clinical Excellence should lead to a proven improvement of glucose control in order to be maintained. 11 The French national insurance system is less stringent and allows the coverage of pump therapy for both type 1 and type 2 diabetes patients for whom an adequately managed insulin MDI regimen does not allow the achievement of defined targets of diabetes treatment. 10 Of note is that use of pump therapy in type 2 diabetes patients seems very limited in European countries, but no precise database is available. In Germany and France, less than 5% of pump users have type 2 diabetes, although reimbursement of pump therapy is agreed to in France, and specific funds can be allocated for the coverage of the cost of pump treatment in Germany when argued. In most other countries, insulin pump therapy is not approved for type 2 diabetes, because of the lack of evidence-based benefit. From these examples in addressing the indication and the coverage process of pump therapy, significant discrepancies in the number of patients who could move to pump therapy can be expected among the different European countries. The more flexible U.S. approach of indicating pump therapy, helped by a different process of insurance coverage, and supported in practice by extended educational resources from diabetes educators and pump manufacturers, can well explain the different penetration rate of pump use in the United States versus Europe.
The situation of pump use for diabetes therapy is even worse in Asia because of the lack of national health insurance coverage. Insulin pump therapy is limited to cases of individuals who mostly have type 2 diabetes and have sufficient resources to cover its cost.
Current Trends and Issues of Pump Use in Europe
The economic situation will likely drive more than ever pump use in Europe. Because of the growing deficits of national healthcare insurance systems in Western Europe, one may expect a reinforced attention paid to the conditions of cost coverage of insulin pump therapy. The price list for the coverage of pump therapy has already been revised in France. The German authority for healthcare costs has underscored the need for scientific evidence to allow sustained coverage of diabetes therapy, including the use of insulin analogs. However, enough evidence has been brought on the advantages of fast-acting analogs versus regular insulin in pumps, so that 80–90% of patients treated by pumps in Germany benefit from reimbursed use of fast-acting analogs. 17 It may be expected that the criteria for pump cost coverage will be subjected to reviews in forthcoming years in the countries where full reimbursement has been obtained. In contrast, the improved economic and social welfare in Eastern Europe, especially in the countries that joined European Union recently, will likely lead to approved reimbursement of pump therapy where it is still lacking.
More than ever, scientific evidence will have to be shown to support the reimbursement for pump use in the less consensus-based indications. This context should foster clinical research initiatives, including cost-effectiveness studies. International consensus will also be strongly valued, albeit also needing to be supported by scientific evidence rather than consensus-based expert agreements.
However, even in spite of this trend for more thorough examination of indications, true possibilities of extension of pump use still remain in Europe. As already mentioned, an important limiting factor is the number of trained physicians and healthcare givers to pump therapy. Younger generations of physicians are more exposed to technology in diabetes care and have been confronted by pump use during their teaching process. Many type 1 diabetes patients would benefit from pump therapy since not at target although using MDI and adhering to the recommended follow-up. The patients themselves are now better informed about pump therapy through chats with their peers, including on the internet. They are also keener to use technological tools in their daily life. Moreover, therapeutic education for costly chronic diseases is increasingly promoted by the healthcare insurance entities, and it should result in a reorientation of human healthcare resources toward patient education. The pharmaceutical and medical device industry may well be approached by the health authorities to dedicate more efforts and funds to support therapeutic education in the near future.
A noticeable issue remains about the way to get coverage of even more sophisticated technologies connected to insulin pump therapy. The most important current topic is continuous glucose monitoring. Scientific evidence is growing to support the benefit of continuous glucose monitoring in pump users. 5,6,18 However, except in Sweden (recently), continuous glucose monitoring has not received reimbursement coverage in Europe so far. The poor financial balance of national healthcare insurance systems in Europe is deeply responsible for this lack, and the close horizon is not rosy. Besides further clinical research on this topic to identify the best beneficiaries of these technological advances, new approaches will have to be considered by the healthcare insurance systems in order to promote the prevention of complications of diabetes. Long-term views will have to be adopted to implement new strategies for a better financial coverage of efficient technology dedicated to diabetes care instead of huge expenses dedicated to advanced complications of diabetes. Combined efforts from the scientific and healthcare professionals and from the patients themselves will be needed to hopefully reach this goal.
Footnotes
Acknowledgments
The author thanks Medtronic Europe (Tolochenaz, Switzerland) for the information provided on the distribution of pump use and cost coverage in Europe and in the United States.
Author Disclosure Statement
E.R. is a consultant for Roche Diagnostics, Novo-Nordisk, Disetronic Medical Systems, and Sanofi-Aventis. He has received honoraria from Eli Lilly, Roche Diagnostics, Medtronic, Sanofi-Aventis, and Novartis for lectures and development of educational presentations.