
Abstract
Background:
To self-inject insulin, individuals with diabetes must be able to attach the needle to the injector, recognize the appropriate insulin dosage, detach the needle from the injector, and perform a series of operations necessary for the actual injection. These tasks require a grip strength that is strong enough to hold the necessary devices, eyesight, the use of both hands, and at least a minimum intellectual capacity. Subjects who are unable to grasp or handle the devices required for insulin injection often have difficulties with the self-injection of insulin.
Methods:
We treated four diabetes patients who had trouble grasping objects and using both hands. One patient had lost five fingers in an accident, two patients had suffered from ischemic cerebral infarction resulting in complete one-sided hemiplegia with no movement in one arm, and one patient had limited muscular power in an arm as a result of spinal cord disease. The plasma glucose control was poor, and the initiation of insulin therapy was necessary in each of these patients. In three cases, we used a commercially available self-injection device (HumaHelper™; Eli Lilly Japan K.K., Kobe, Japan) to enable self-injection; in the fourth case, we used a newly manufactured device similar to HumaHelper.
Results:
All the patients were able to inject insulin by themselves using the appropriate supplementary devices. The blood glucose control of all the patients subsequently improved.
Conclusion:
Existing or newly manufactured supportive devices can enable handicapped subjects to self-inject insulin.
Introduction
However, patients face many problems when they first begin insulin treatment to maintain favorable glucose control. To self-inject insulin, individuals with diabetes must be able to attach the needle to the injector, recognize the appropriate insulin dosage, detach the needle from the injector, and perform a series of operations necessary for the actual injection. These tasks require a grip strength that is strong enough to hold the necessary devices, eyesight, the use of both hands, and at least a minimum intellectual capacity. The most common cause of difficulty performing self-injections is ischemic cerebral infarction resulting in complete one-sided hemiplegia; the second most common cause of difficulty is a decrease in muscular power as a result of aging, diabetic neuropathy, or spinal cord disease. Patients who cannot use both hands because of finger or arm amputations also have difficulty performing self-injections. Therefore, performing the series of operations required for self-injection can be quite difficult for subjects who are unable to grasp or handle the standard devices used for insulin injection. These problems can delay the start of insulin treatment or even prevent treatment.
Sohmiya et al. 6 and Harvey et al. 7 reported the design and fabrication of supplementary devices for use with insulin pens that enabled patients who had suffered from an ischemic cerebral infarction resulting in complete one-sided hemiplegia to self-inject insulin. Moreover, three other reports have described the design and fabrication of a supplementary tool for use with vial and syringe-type insulin injection by hemiplegic subjects. 8 –10 In these reports, healthcare professionals designed and fabricated the supplementary devices used by their patients; however, such treatments are very difficult and time consuming. The use of supplementary tools that are commercially available or easily made has not been previously reported. Here, we describe the cases of four patients with diabetes who initially had difficulty injecting insulin by themselves but who were ultimately successful once they began using an appropriate supplementary device. Three of these patients used HumaHelper™, a commercially available self-injection device distributed by Eli Lilly Japan K.K. (Kobe, Japan), with two of the patients using additional supplementary tools. The fourth patient used a supplementary device that was similar to HumaHelper.
Cases
The details of each case are summarized in Table 1.
Case 1 (a 54-year-old woman with type 2 diabetes mellitus who had lost all of her left fingers)
The patient had been diagnosed as having diabetes at the age of 47 years. Sulfonylurea, pioglitazone, and an α-glucosidase inhibitor were prescribed, but her plasma glucose control was poor (hemoglobin A1c [HbA1c], 10.0%). She was admitted to our hospital for the stringent control of her blood glucose level.
Because the patient's endogenous insulin secretion capacity was extremely impaired, we planned to switch her treatment from OHAs to insulin. However, as she had lost her five left fingers in an accident at the age of 49 years, she had great difficulty injecting the insulin by herself. We therefore instructed her in the use of an insulin self-injection device (HumaHelper) to be used with the HumaPen® Luxura™ [HL] (Eli Lilly and Co., Indianapolis, IN), which enabled her to inject the insulin single-handedly. As shown in Figure 1, the HumaHelper device is a cylinder rubber product (outside diameter, 50 mm; height, 50 mm) that can be fixed to the surface of a table. The device has two holes: a small hole, for attaching the needle and turning the insulin unit dial, and a large hole, for the insertion of the insulin cartridge. This device was originally designed for use with the HL insulin doser, but it also works well when used in combination with the FlexPen® [FP] (Novo Nordisk, Copenhagen, Denmark).

(
The patient began injecting a biphasic insulin analog (Humalog® Mix50™, Eli Lilly and Co.) twice daily. The HumaHelper made it possible for her to attach and remove the needles and to self-inject the insulin (Fig. 2). Three months after the introduction of the insulin therapy, her HbA1c level had decreased to 6.9%.

Procedure for insulin self-injection (Case 1). (
Case 2 (a 67-year-old woman with type 2 diabetes mellitus who could not move her right arm because of complete right hemiplegia)
The patient had been diagnosed as having diabetes at the age of 60 years. An OHA was prescribed, and her plasma glucose control improved. Her renal dysfunction, however, was exacerbated because of anti-neutrophilic cytoplasmic antibody-related nephritis. She was admitted to our hospital with the intention of switching her treatment from the OHA to insulin. The patient lived alone and had suffered an ischemic cerebral infarction at the age of 63 years, resulting in complete right hemiplegia with no movement in her right arm.
We instructed her in the use of an insulin self-injection device (HumaHelper) to allow her to perform the insulin injections using her left hand. She began injecting a biphasic insulin analog (Humalog Mix50) once daily. However, once she had placed the appropriate number of insulin units in the needle, she was unable to maintain the insulin injector in a stable position because her grip was inadequate. We therefore instructed her in the combined use of the HumaHelper and an HL slipping stop so that she would be able to self-inject the insulin successfully using her non-dominant left hand. The use of the HL slipping stop is illustrated in Figure 3. The combined use of these devices enabled her to self-inject the insulin. Three months after the introduction of the insulin therapy, she was able to self-inject the insulin, and her fasting blood sugar level had improved from 141 ± 35 mg/dL before insulin therapy to 93 ± 5 mg/dL.

General appearance and use of the HL slipping stop (Case 2). (
Case 3 (a 64-year-old man with type 2 diabetes mellitus)
The patient had been diagnosed as having diabetes at the age of 58 years. Sulfonylurea was administered, but his plasma glucose control was poor. He was admitted to our hospital for the stringent control of his glucose level. Because of chronic pancreatitis, the patient's endogenous insulin secretion was markedly impaired. We therefore initiated intensive insulin therapy (Novorapid® [16-7-16-0]/Novolin N® [0-0-0-4] [both from Novo Nordisk]) using an FP. During the course of the patient's hospitalization, the muscles of his left arm were found to be atrophic (Fig. 4A), and the muscular power of his left hand was markedly decreased. He was diagnosed as having cervical spondylotic myelopathy.
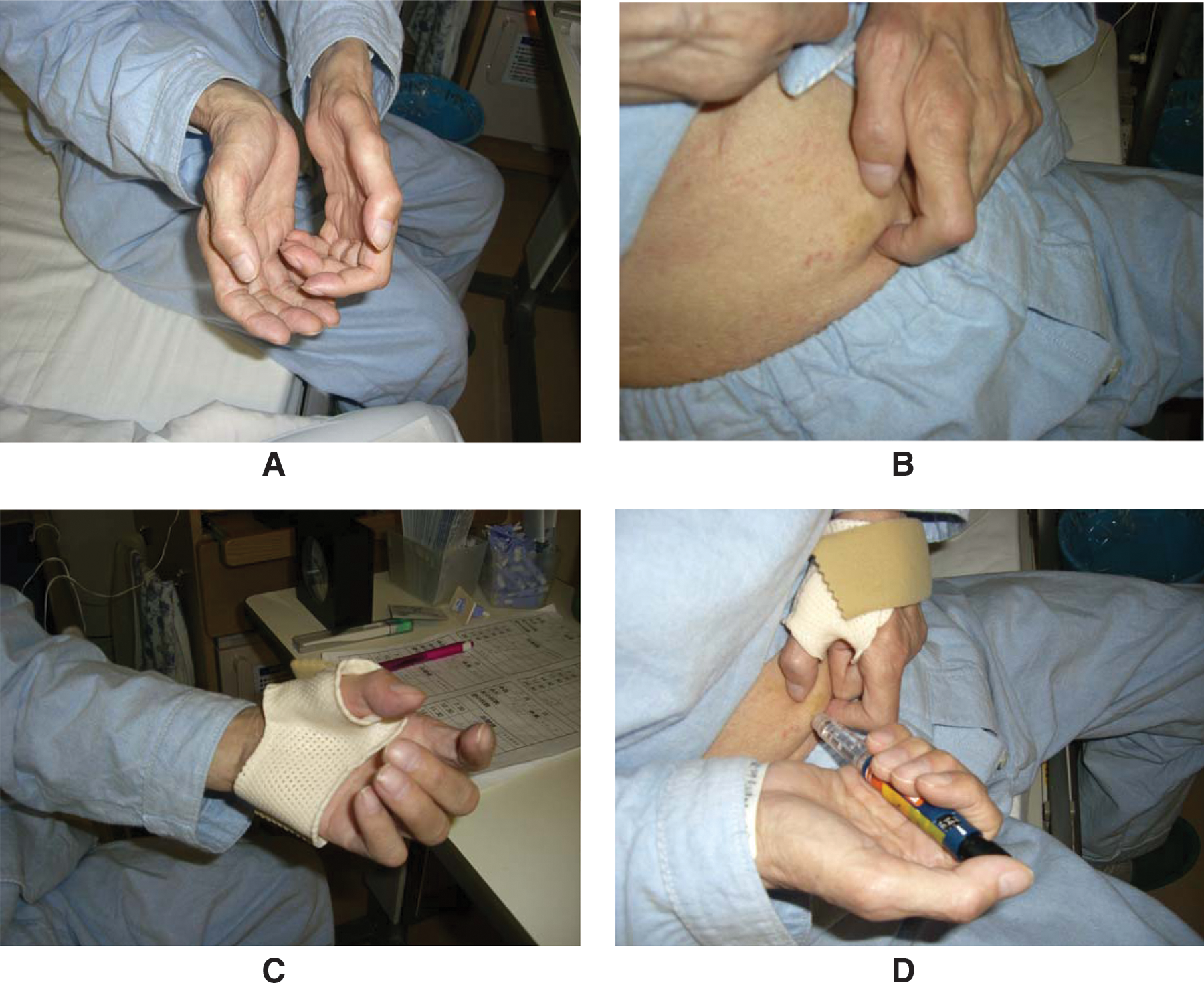
Use of a splint (Case 3). (
We instructed the patient in the use of an insulin self-injection device (HumaHelper) to enable him to inject insulin using only his right hand. The patient commented that he would be able to perform the injection more smoothly if he could lift his abdomen with his left hand (Fig. 4B). This inspired an occupational therapist to make a splint for his left hand, enabling the patient to lift his abdomen using the splint sheet (ORFIT Industries, Wijnegem, Belgium) (Fig. 4C). Through the combined use of this splint and the HumaHelper, the patient was able to master the smooth self-injection of insulin (Fig. 4D). Three months after the introduction of insulin therapy, he was able to self-inject the insulin, and his HbA1c level had improved from 8.1% before insulin therapy to 6.0%.
Case 4 (a 72-year-old man with type 2 diabetes mellitus and complete left hemiplegia)
The patient had been diagnosed as having diabetes at the age of 30 years. His renal dysfunction was severely impaired because of chronic renal failure associated with poor long-term blood pressure control. He was treated at another hospital, and insulin treatment was started. At the age of 68 years, he suffered an ischemic cerebral infarction resulting in complete left hemiplegia with no movement in the left arm. While he was admitted at another hospital, the nurses in charge of his care injected insulin (NovoMix 30) subcutaneously into his abdomen twice a day. Afterwards, he was admitted to our hospital in the hope that he would be able to master insulin self-injection using his injured right hand.
We instructed him in the use of an insulin self-injection device (HumaHelper) with an FP to enable him to inject insulin using only one hand. However, he had difficulty detaching the needle from the device because of his poor eyesight. An occupational therapist made an insulin self-injection device using an empty polyethylene teraphthalate (PET) bottle, modeling clay, and a skid mat. The fabrication of this device is shown in Figure 5. The patient was able to master the self-injection of insulin using this new device because the needle can be detached at eye level (Fig. 5F). This device is useful for subjects with impaired vision because the needle can be detached at a position within their range of vision. Three months after the introduction of insulin therapy, he was able to self-inject the insulin, and his fasting blood sugar level had improved from 148 ± 39 mg/dL before insulin therapy to 106 ± 32 mg/dL.
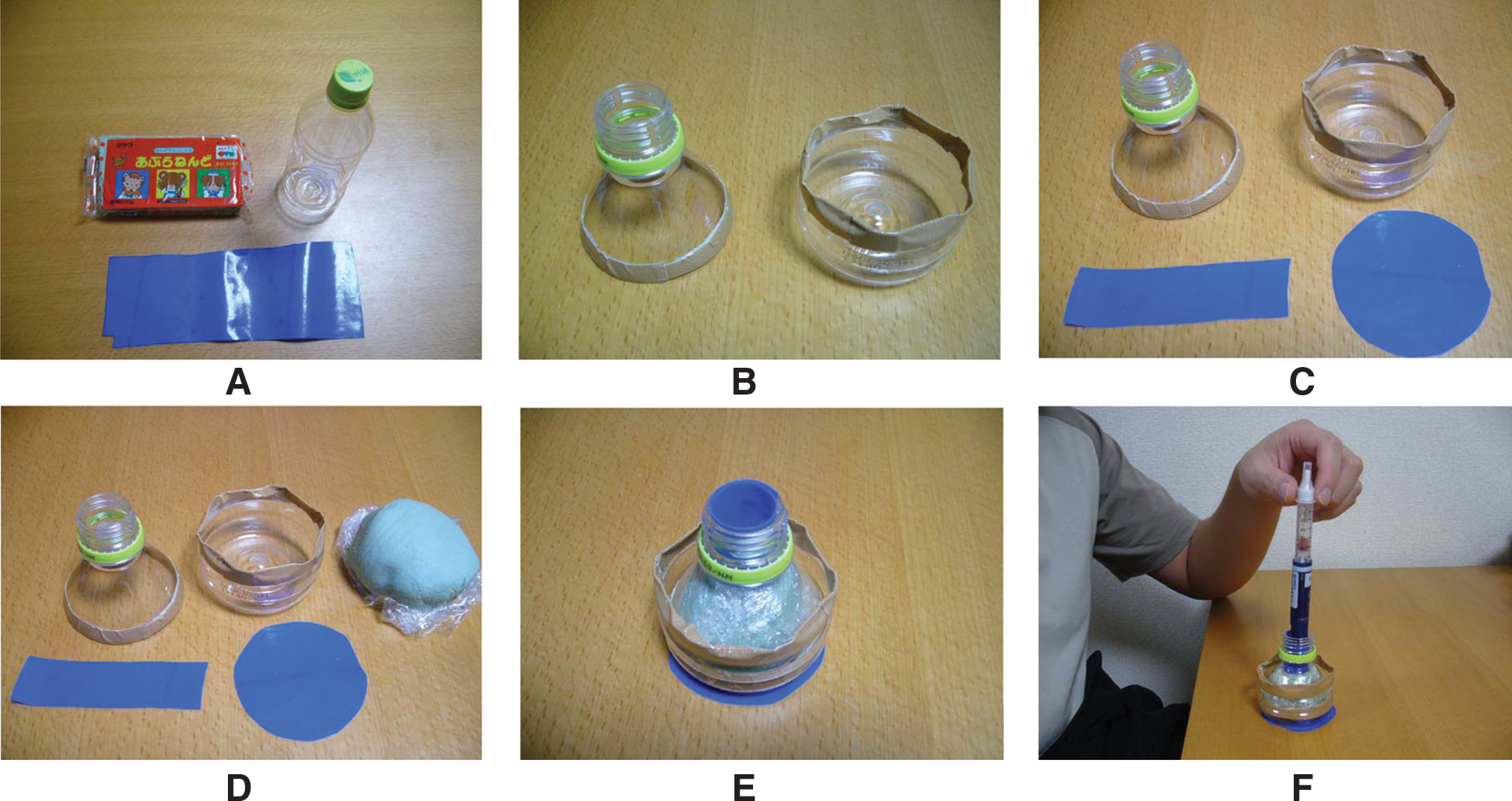
Fabrication method (Case 4). (
Discussion
To self-inject insulin, a grip strength strong enough to hold the necessary devices, eyesight, the use of both hands, and at least a minimum intellectual capacity are needed. Manual dysfunction arising from finger amputation, a cerebrovascular incident, or muscle weakness can make the self-injection of insulin quite difficult, possibly leading to a diminished quality of life. Between April 2007 and February 2008, we treated four diabetes patients who had trouble grasping objects or using both hands. Though the numbers of cases are only four, the most important finding of the present series was that all the patients were able to self-inject insulin using existing or newly made supplementary devices. Blood glucose control was subsequently improved in all the patients. After 3 months on the insulin therapy, HbA1c levels were improved from 10.0% to 6.9% in Case 1 and from 8.1% to 6.0% in Case 3, respectively. Fasting blood glucose levels were improved from 141 ± 35 mg/dL to 93 ± 5 mg/dL in Case 2 and from 148 ± 39 mg/dL to 106 ± 32 mg/dL of Case 4, respectively.
In Case 1, the patient was able to self-inject insulin using only the HumaHelper. In Case 2, the patient was able to self-inject the insulin using a HumaHelper, but she often dropped the injection device because of her poor grip when using her left hand. Therefore, we instructed her in the combined use of HumaHelper and an HL slipping stop. This kit was also commercially available. In Case 3, the patient was able to self-inject the insulin using a HumaHelper; however, as this patient wished to perform the procedure more smoothly, an occupational therapist made him a splint. In Case 4, the patient's poor eyesight made it difficult for him to detach the needle; consequently, an occupational therapist made a device that enabled the patient to detach the needle close to his eyes. This device enabled the patient to master the self-injection of insulin.
Proper use of the HumaHelper requires some training. If other problems are noted during the training period, supplementary tools can be used to provide a solution.
The HL is a durable insulin pen that contains a replaceable insulin cartridge, and patients can replace empty cartridges with the aid of a HumaHelper. The dial of this device can be easily manipulated. On the other hand, the FP is a disposable and prefilled insulin injector that is lighter than the HL but somewhat expensive in Japan. We selected either the HL or the FP according to the patients' preferences. Compared with vials and syringes, insulin pens offer substantial improvements in compliance, freedom, and flexibility for all insulin-using patients. 11 –13 Consistent with these results, many studies have reported a preference for pen devices over traditional syringes. 14 –16 The insulin pen has made independent insulin delivery among blind patients with diabetes easier by eliminating the need to visually draw up insulin from a vial. 17 The clarity of the click when setting a dose on an insulin delivery device also reportedly affects a patient's confidence in selecting the correct dose. 18
In Japan, a newly made supplementary device for use with an insulin pen has been reported; this device was designed for use by hemiplegic patients, 6 and several case reports on such supplementary devices have been published in Japanese. On the other hand, only a few similar reports have been made in Europe and North America. 7 –10 One report 7 described a device for use with an insulin pen, while three other reports 8 –10 described devices for use with vial and syringe-type insulin injections. These differences might reflect differences in the methods used for the self-injection of insulin between Japan and other countries. In Japan, up to 90% of all insulin injections are reportedly performed using pen-type devices, whereas insulin pens account for only 14% of all insulin injections in the United States. 19
In all of these reports, the healthcare professionals designed and fabricated the supplementary devices used by their patients. The use of an existing supplementary tool has not been previously reported. In the present report, we used a commercially available self-injection device (HumaHelper) for three patients and a newly made device similar to the HumaHelper for one patient.
Healthcare professionals must ensure that appropriate supplementary devices are available for patients who have trouble grasping objects or using both hands. However, it is not easy for healthcare professionals to fabricate such devices from scratch within the period of an individual patient consultation. Therefore, self-injection devices should be available commercially. Much to our regret, however, the HumaHelper has been discontinued; in Japan, however, a similar rubber product is being sold for another use under the name “AORI-GOMU” (Waki Sangyo Co., Ltd., Osaka, Japan). The AORI-GOMU is a rubber band that can be applied to the leg of a chair and the gate in a truck bed. Healthcare professionals can purchase this product and instruct patients who have trouble grasping objects or using both hands to use this product to self-inject insulin according to the instructions in the pamphlet provided with the HumaHelper. However, few healthcare professionals are aware that the AORI-GOMU can be used in such a manner. We hope that a self-injection device similar to the HumaHelper will become commercially available worldwide, as such a product would greatly benefit diabetes patients and their families. We also hope that patients who have trouble grasping objects or using both hands will be able to use such devices to self-inject insulin without requiring the help of another individual.
Conclusions
To self-inject insulin, a series of actions are required: the needle must be attached to the device, a dial must be turned or set to select the insulin dose, a series of operations must be performed for the actual injection of the insulin, and the needle must be detached. We treated four patients who had difficulty grasping objects or using both of their hands, complicating the self-injection of insulin. Appropriate supportive devices, either existing or newly manufactured, enabled the handicapped subjects to self-inject insulin. Such devices would greatly benefit handicapped subjects with diabetes throughout the world.
Footnotes
Acknowledgments
This work was supported in part by the Yokohama City University Center of Excellence Program and a grant for the 2007 Strategic Research Project (K19004) of Yokohama City University.
Author Disclosure Statement
No competing financial interests exist.