
Abstract
Background:
The relationship between admission hyperglycemia and adverse outcome in myocardial infarction has been shown consistently. However, achieving and maintaining normoglycemia in ST elevated myocardial infarction (STEMI) patients has proven difficult. This study aimed to investigate the efficacy of sensor-augmented insulin pump (SAP) therapy to treat hyperglycemia.
Methods:
In a randomized controlled pilot trial, we assigned 20 patients, 30–80 years old, admitted with STEMI and hyperglycemia (≥140 mg/dL) to receive either 48 h of strict glycemic control with an subcutaneous insulin pump augmented with a continuous glucose monitor (SAP group) or to treatment according to standard practice (Control group) with glucose measured by blinded continuous glucose monitoring. The main outcome measure was proportion of time spent in hyperglycemia.
Results:
The median treatment time was 47.0 h (interquartile range [IQR], 46.2–48.0 h) in the SAP group and 44.6 h (IQR, 22.0–48.6 h) in the Control group. The median proportion of time ≥ 140 mg/dL was 14.6% (IQR, 10.5–18.5%) in the SAP group and 36.3% (IQR, 26.0–80.4%) in the control group (P = 0.006). The proportion of time ≤ 70 mg/dL was 8.9% (IQR, 8.3–12.5%) in the SAP group versus 0% (IQR, 0–2%) in the Control group (P < 0.001). Plasma glucose decreased significantly in the SAP group compared to the Control group (P = 0.025).
Conclusions:
SAP therapy is effective in reducing hyperglycemia in STEMI patients on the coronary care unit. This is accompanied by a small but significant increase in hypoglycemia. Although a promising tool for in-hospital hyperglycemia therapy, SAP needs improvement before continuing to large-scale randomized controlled trials.
Introduction
Subjects and Methods
Design and patients
We performed a randomized controlled pilot trial including patients admitted to the CCU of the Academic Medical Center (Amsterdam, The Netherlands), a university hospital. Patients with an admission glucose of ≥ 140 mg/dL, measured from a venous blood sample using the Accu-Chek® Inform® (Roche Diagnostics, Basel, Switzerland), 30–80 years old, and with ST elevation myocardial infarction (STEMI), treated by primary percutaneous coronary intervention (PCI), were included. Exclusion criteria were known diabetes mellitus type 1, abdominal abnormalities that might hinder either glucose measurement by the sensor or the continuous subcutaneous insulin infusion, and simultaneous participation in other studies. The study was approved by the ethic committee of the Academic Medical Center and performed in accordance with the Declaration of Helsinki. All patients provided written informed consent.
Procedures
After inclusion, patients were randomized to either 48 h of glucose control with SAP (SAP group) or blinded continuous monitoring only with treatment according to standard practice (Control group). A flow chart is provided in Figure 1.
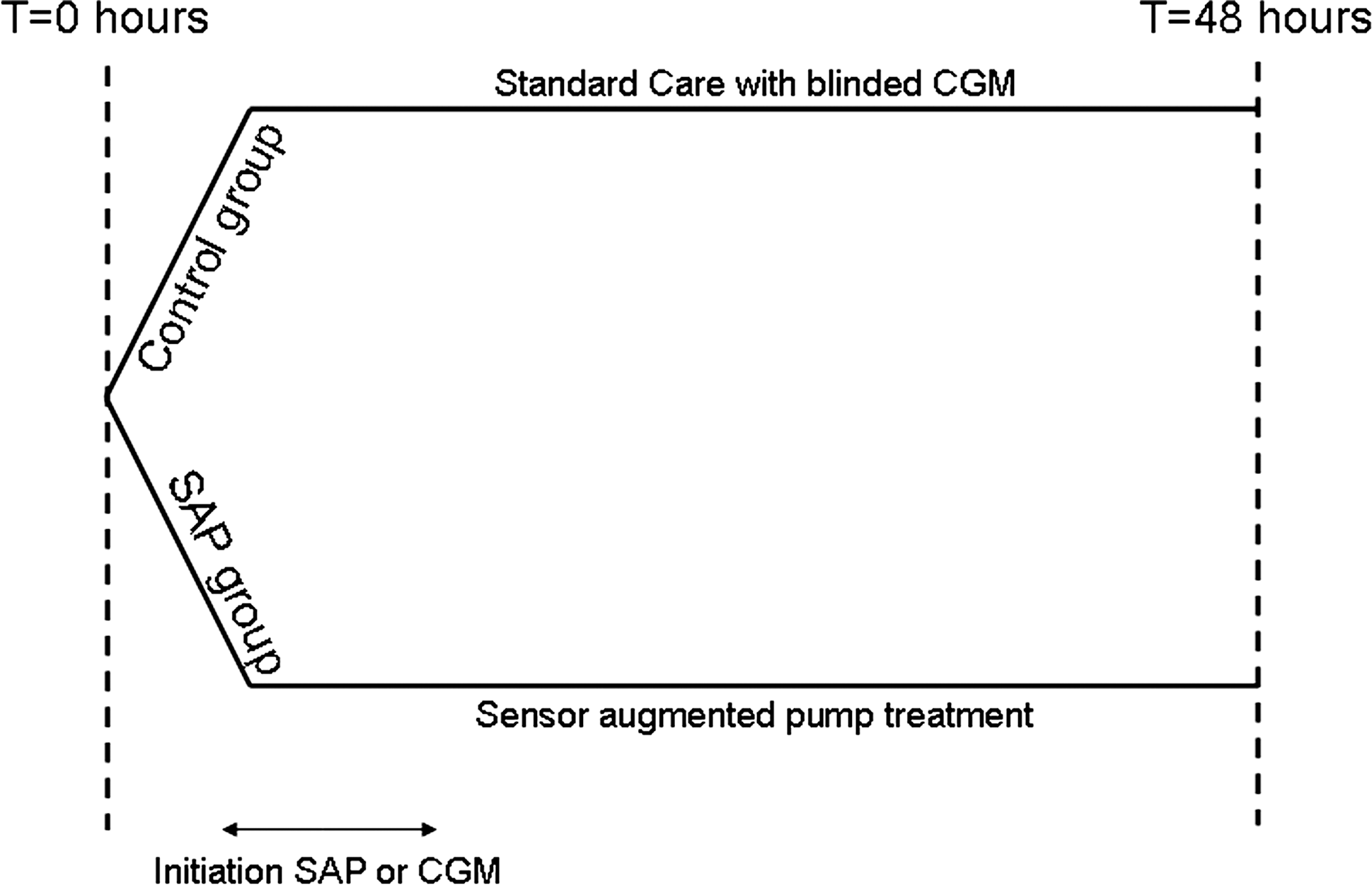
Study flowchart. CGM, continuous subcutaneous glucose monitor; SAP, sensor-augmented insulin pump.
In the SAP group, preceding PCI, an intravenous starting insulin bolus was injected based on the admission glucose, using an adapted standardized algorithm (see Supplementary Appendix at
The nursing staff was instructed to adjust the basal insulin rates responding to alarms according to the algorithm (see Supplementary Appendix at
In the control group the CGM of the Paradigm Real-Time system was inserted before or shortly after PCI. The CGM readings were not made available to the treating physician and the patient. If patients had glucose levels above 270 mg/dL during three consecutive routine glucose measurements, standard practice at our institution indicated that therapy should be started. To minimize bias, responsibility for the initiation or adjustment of insulin remained with the treating physician or consulting internal medicine physician. All patients were instructed not to consume snacks in between the regular meals provided by the hospital.
In both groups the CGM was calibrated according to the manufacturer's instructions using venous blood samples every 6 h. The glucose values for calibration were determined using the Accu-Chek Inform. In the SAP group, additional calibrations were performed if there was a false alarm (see Supplementary Appendix at
Routine venous blood samples for glucose determination were taken before PCI and at 24 and 48 h after admission. Blood was collected in heparin-treated gel tubes and centrifuged for 10 min at 1,600 g and 18°C for immediate glucose determination.
Outcome measures and statistical analyses
The main outcome measure was the proportion of time spent in hyperglycemia (≥140 mg/dL) as measured by CGM during a 48-h period. Also, we calculated the proportion of time spent in hypoglycemia (≤70 mg/dL) and spent in the initial alarm target range (85–110 mg/dL) and the area under the curve (AUC) for hypo- and hyperglycemia.
Differences in plasma glucose values during admittance were assessed. Furthermore, we calculated CGM accuracy with the mean absolute difference (MAD). The standardized venous recalibration samples taken every 6 h were compared with the last sensor value before recalibration (MAD = |CGM value − blood glucose|/blood glucose). Thus, we did not use the additional calibration values performed in the SAP group in case of a false alarm. Finally, the number of alarms to which the nursing staff had to respond in the SAP group was assessed as well as the number of hypoglycemic episodes (plasma glucose ≤ 70 mg/dL) that were followed by oral or intravenous glucose administration.
A formal power analysis was not possible because this is the first study applying SAP in the CCU. Therefore, we aimed to include 20 patients to be randomized in a 1:1 ratio. Results were presented as mean ± SD or median with interquartile range (IQR) were appropriate. For the between group differences from the sensor-derived end points, we used the Mann-Whitney U test or Student's t test. The between-group difference for the plasma glucose values were tested using an analysis of variance model for repeated measurements. All analyses were performed in SPSS version 16.0 (SPSS Inc., Chicago, IL).
Results
After screening 45 patients we randomized 20 patients to either 48 h of SAP therapy or standard care. In both the SAP group and Control group one patient dropped out because of transfer to another hospital. In the Control group, one patient withdrew informed consent. Thus nine and eight patients were eligible for analyses in the SAP and Control groups, respectively. All patients resumed eating regular meals after admission. The baseline characteristics are provided in Table 1. The median amount of intravenous insulin given as a bolus before PCI in the SAP group was 3.6 IU (IQR, 3.3–4.8 IU). Hereafter, 102.9 IU (IQR, 67.6–147.3 IU) was given subcutaneously with the insulin pump, of which 82% (IQR, 69–92%) was basal insulin. In the Control group no insulin therapy was initiated by the treating physician. The median treatment time the SAP group was 47.0 h (IQR, 46.2–48.0 h), and in the Control group it was 44.6 h (IQR, 22.0–48.6 h) (P = 0.67).
CAD, coronary artery disease; HbA1c, hemoglobin A1c; IQR, interquartile range; LAD, left anterior descending; LCX, left circumflex; MI, myocardial infarction; RCA, right coronary artery; SAP, sensor-augmented insulin pump.
Figure 2 shows the median glucose values for both groups as measured every 5 min by the CGM system (2 h after initiation). The percentage of time spent in hyperglycemia during the the 48-h period after PCI was significantly smaller in the SAP group: 14.6% (IQR, 10.5–18.5%) versus 36.3% (IQR, 26.0–80.4%) (P < 0.01). The proportion of time spent in hypoglycemia was significantly greater in the SAP group (8.9%; IQR, 8.3–12.5%) compared to the Control group (0%; IQR, 0–1.5%) (P < 0.001), and the percentage of time spent in the initial alarm target range of 85–110 mg/dL was 32.7% (IQR, 28.4–36.0%) in the SAP group and 2.2% (IQR, 0.2–27.7%) in the control group (P = 0.036). The AUC for hyperglycemia was significantly smaller in the SAP group (0.9 mg/dL/min; IQR, 0.5–1.7 mg/dL/min) compared to the Control group (3.6 mg/dL/min; IQR, 1.2–8.2 mg/dL/min) (P = 0.015). When comparing the AUC for hypoglycemia this was 0.1 mg/dL/min (IQR, 0.1–0.3 mg/dL/min) in the SAP group and 0 mg/dL/min (IQR, 0–0 mg/dL/min) in the Control group (P < 0.01).

Median sensor glucose values every 5 min after start of measurements sensor for both groups. SAP, sensor-augmented insulin pump.
The median plasma glucose in the SAP group decreased from 186 mg/dL (IQR, 162–236 mg/dL) pre-PCI to 86 mg/dL (IQR, 72–133 mg/dL) after 24 h and 83 mg/dL (IQR, 76–128 mg/dL) after 48 h (Fig. 3). In the Control group, the median glucose pre-PCI was 164 mg/dL (IQR, 155–205 mg/dL), which decreased to 139 mg/dL (IQR, 114–189 mg/dL) after 24 h and 124 mg/dL (IQR, 110–207 mg/dL) after 48 h. The plasma glucose in the SAP group decreased significantly more compared to the Control group (P = 0.025).
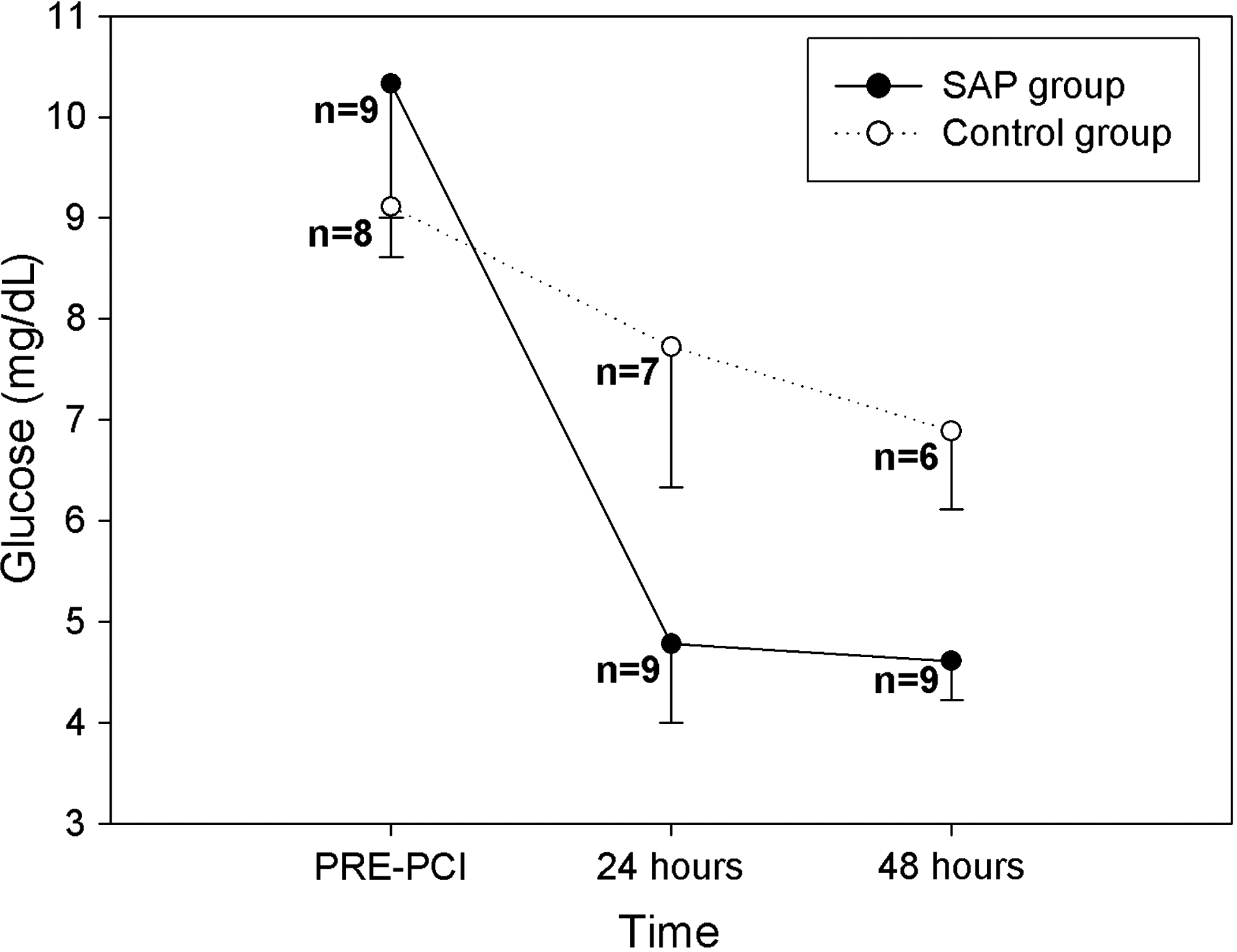
Median plasma glucose values for both groups. The plasma glucose decreased significantly more in the sensor-augmented insulin pump (SAP) group (P = 0.025). PCI, primary percutaneous coronary intervention.
In total, we measured 7,620 valid sensor values during the study. In 6% of the monitoring time the sensor did not generate a signal. On four occasions a sensor had to be replaced because of sensor failure. The mean number of calibrations per 24-h period was nine (±four) in the SAP group and four (±one) in the Control group, and the median number of paired regular calibration values (every 6 h) per patient was five (IQR, four to 6.5). The accuracy of the CGM based on the regular calibration values did not differ significantly between both groups with an MAD of 21.6% (±9.6%) in the SAP group and 18.5% (±8.8%) in the control group (P = 0.50).
In the SAP group, the nursing staff responded 11 times (± six) per 24-h period to an alarm, with an equal distribution between the hypo- and hyperglycemic alarms. In the majority of the cases, the patient needed to indicate that the alarm was going off because the acoustic signal was too weak to be heard by the nurse on the CCU. The basal rate was adjusted nine times (± five times [mean ± SD]) per 24-h period. The BolusWizard advice was followed 75% of the time; in 25% of the time the advised amount of insulin was lowered by the study staff.
In the SAP group, hypoglycemia (plasma glucose ≤70 mg/dL) followed by glucose administration occurred 11 times in six patients. Of these, three patients had known diabetes. All events were without clinical sequelae and occurred at least 23 h after admission with a median temporary distribution of 31.4 h (IQR, 26.7–36.6 h) after admission. In the Control group, no hypoglycemia was observed. No other device-related adverse events occurred.
Discussion
In this randomized controlled trial we showed that SAP therapy in patients with STEMI and admission hyperglycemia lowered the proportion of time spent in hyperglycemia. This was accompanied by a significant increase in the percentage of time in normoglycemia, but also an increase in hypoglycemia and workload.
The (CREATE)-ECLA, Pol-GIK, and GIK trials all aimed to deliver high concentrations of insulin in glucose-insulin-potassium solution to patients with AMI, without lowering the mean glucose levels. 19 –21 All of these trials yielded negative results. In patients with diabetes mellitus, the first DIGAMI trial successfully lowered the glucose during admittance and thereafter, thereby improving survival. 6 Targeting the mean glucose in the CCU seems more important than the administration of insulin, as also indicated by Kosiborod et al. 9 In contrast with the DIGAMI 2 and HI-5 trial, we were able to lower median glucose values during CCU admittance after STEMI. 7,8 The reduction of the proportion of time spent in hyperglycemia that we found was also shown in the trials investigating SAP therapy in diabetes mellitus type 1 patients. 14 –16,22 An increase in hypoglycemia is not a consistent finding in these trials; however, they all concern intensively insulin-treated type 1 patients, with hypoglycemia occurring in both arms of the studies. In our study, only the SAP group received strict glucose control with ensuing hypoglycemia.
The use of a continuous glucose sensor in a CCU setting was investigated before in an exploratory study by Rowen et al. 23 They concluded that the use of CGM was helpful to the nursing personnel, without an increase in workload. This is in contrast with our findings, as most of the personnel indicated that the workload substantially increased because of SAP treatment. Besides paying attention to CGM alarms and checking the plasma glucose, the nursing staff had to follow the treatment algorithm and perform calibrations at set times. The number of alarms to which the nursing staff had to respond was experienced as high (11 times [± six]) per 24-h period). To decrease the workload, we changed the alarm thresholds for the hyperglycemic alarm during the trial. One important explanation for the false-positive or -negative alarms is the inaccuracy of the interstitial glucose measurements compared to the plasma glucose. In our trial we found the MAD to be 18.5–21.5%. It should be noted that we used venous plasma samples to determine the glucose calibration values, whereas the usual outpatient practice is to calibrate against capillary blood. However, our results are in line with previous studies investigating the CGM in the ICU. 24,25
The somewhat higher calibration rate in the SAP group did not lead to a different accuracy of CGM measurements in both groups, which may be due to the fact that sensor accuracy is more influenced by the timing rather than the frequency of the calibration. 26 We only calibrated the sensor when glucose values were stable and the patient was not eating.
On many occasions, the patient had to alert the nurse that an alarm was signaling. It is therefore likely that not all alarms were addressed immediately, and this could have contributed to the hypoglycemia developed in six patients. The observation that the acoustic signal of the SAP is not loud enough in the hospital setting has also been made by Logtenberg et al. 24 We have, however, used a device designed for treatment in the outpatient setting, and necessary adjustments for the in-hospital setting were to be expected.
Because of logistic reasons we were not always able to complete the 48 h of treatment time. Figure 3 clearly shows that the median sensor value lines meet before completion of the preset 48 h of intervention. Although this is a limitation of the trial, plasma glucose in SAP was lower compared to the Control group up to 48 h.
Because this was a pilot trial, it was limited by its relative small sample size. Therefore, despite appropriate randomization procedures, the percentage of patients with diabetes mellitus was almost twice as high in the SAP group (44%) compared to the Control group (25%), which was also reflected in a higher admission glucose and hemoglobin A1c in the SAP group. However, despite this baseline difference putting the SAP group at the disadvantage, glucose in the SAP group was significantly lower compared to the Control group in the first 48 h. Notably, there was also a spontaneous glucose decrease in the Control group from baseline to 48 h.
This is the first randomized controlled pilot trial showing that in hyperglycemic STEMI patients, SAP clearly significantly reduces the duration of hyperglycemia as well as plasma glucose levels, compared with hyperglycemic control patients.
This is, however, accompanied by a small but significant increase of hypoglycemia and considerable workload for the nursing staff. Although a promising tool for in-hospital hyperglycemia therapy, SAP needs improvement, especially with regard to sensor accuracy and the alarm function of the device, before continuing to large-scale randomized controlled trials.
Footnotes
Acknowledgments
We thank Medtronic International Trading Sàrl for providing the sensors for this investigation free of charge.
Author Disclosure Statement
J.H.DeV. received speaking fees and research support from Medtronic and Abbott and is a member of the advisory board of Medtronic. The other authors have no competing financial interests.
The study is registered with
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.