
Abstract
Background:
This study evaluated the effect of CSII on hypoglycemia awareness and on glucose profile in type 1 diabetes (T1D) subjects with repeated non-severe or severe hypoglycemia (NS or SH, respectively).
Methods:
We included subjects (1) older than 18 years, (2) with T1D duration of >5 years, (3) on multiple doses of insulin, and (4) without micro- or macrovascular complications and more than four NS events per week (in the last 8 weeks) and more than two SH events (in the last 2 years). NS/SH episodes and hypoglycemia awareness were evaluated. A 72-h continuous glucose monitoring (CGM) was performed before continuous subcutaneous insulin infusion (CSII). A hypoglycemia-induced test was used to evaluate each patient's symptoms in euglycemia/hypoglycemia. Quality of life (QoL) was also evaluated. After 6, 12, and 24 months, all the subjects were reevaluated.
Results:
Twenty subjects were included (34.0 ± 7.5 years old, 12 women, A1c 6.7 ± 1.1%, 16.2 ± 6.6 years of diabetes' duration). At baseline, 19 out of 20 subjects displayed hypoglycemia unawareness, which diminished significantly during the follow-up (3 out of 20). NH episodes per week diminished from 5.40 ± 2.09 at baseline to 2.75 ± 1.74 at the end of the follow-up (P < 0.001). SH episodes fell from 1.25 ± 0.44 per subject-year to 0.05 ± 0.22 after 24 months (P < 0.001). Hemoglobin A1c remained unaltered. With CGM, the percentage of values within 70–180 mg/dL increased (53.2 ± 11.0% to 60.3 ± 17.1%, P = 0.13), and the percentage of values <70 mg/dL decreased (13.7 ± 9.4% to 9.1 ± 5.2%, P = 0.07), after 24 months. Mean amplitude of glycemic excursions diminished after 24 months of CSII (136 ± 28 mg/dL to 115 ± 19 mg/dL; P < 0.02). An improvement in all the aspects of QoL was observed. The basal alteration in symptom response to an induced hypoglycemia improved after 24 months of initiating CSII leading to a response indistiguishable from that observed in a control group of subjects with T1D without repeated NH and SH.
Conclusions:
CSII prevents hypoglycemic episodes, improves hypoglycemia awareness, and ameliorates glycemic profile in T1D subjects with repeated NS/SH. Its use is also associated with an improvement in diabetes QoL.
Introduction
Frequent and repeated episodes of hypoglycemia in subjects with T1D almost invariably result in a reduced ability/failure to recognize hypoglycemia symptoms and signs at the physiological normal threshold (∼55 mg/dL). This syndrome of hypoglycemia unawareness frequently occurs in T1D, and the lack of warning symptoms puts patients at a high risk for SH because they are unable to take measures to prevent it. 5
In the same way a history of hypoglycemia induces unawareness, meticulous prevention of it can reverse hypoglycemia unawareness. Thus, it is essential that intensive insulin therapy for T1D is designed not only to maintain near-normoglycemia, but also to prevent and minimize the burden of hypoglycemia. 6 –9 Although such a goal is feasible, and even including a proper blood glucose monitoring, the use of individualized blood glucose targets, and the implementation of specific education programs, there is no consensus on which is the best rational plan of insulin therapy. 10 –12 A very recent meta-analysis including recent randomized clinical trials found that the use of continuous subcutaneous insulin infusion (CSII) is not associated with a significant difference in hypoglycemia risk. 13
In this context, the use of continuous glucose monitoring (CGM) systems and the evaluation of hypoglycemia awareness could help us to identify these subjects and to decide on a safe approach to optimize the metabolic control for them. 14
The aim of our study was to evaluate the effect of CSII on the frequency of hypoglycemia, hypoglycemia unawareness, and continuous glucose profile characteristics in a group of T1D subjects with repeated NS and SH.
Patients and Methods
We conducted a prospective study including patients consecutively with the following criteria: (1) >18 years old, (2) T1D duration >5 years, (3) on conventional insulin treatment using multiple doses of insulin (MDI) including rapid-acting analogs (lispro or aspart) as prandial insulins and glargine as basal insulin, and (4) with an absence of micro- or macrovascular complications and presenting more than four NS events per week (in the last 8 weeks) and more than two SH events (in the last 2 years). Absence of microalbuminuria was assured by measuring the 24-h urinary albumin excretion rate (last three samples <20 μg/min). The presence of cardiovascular disease was ruled out considering the following: no history of cardiovascular disease events, no electrocardiogram alterations, normal stress echocardiography, and an ankle-brachial index >0.9. The initiation of CSII treatment was proposed to all subjects following the indications and criteria of reimbursement from the Catalan National Health Service authorities. Contraindications for CSII were ruled out in all subjects, mainly including inability to perform self-management of an intensive insulin therapy program, evidence of poor treatment compliance and failure to attend outpatient clinics, and evidence of a disabling psychiatric disorder. 15 The study was approved by the Hospital Clínic i Universitari (Barcelona, Spain) Ethics Committee, and informed consent was obtained from all the patients. The study has been performed in accordance with the ethical standards laid out in an appropriate version of the Declaration of Helsinki.
Within 1 month before initiation of CSII, data on age, gender, duration of the disease, body mass index, renal function, and hemoglobin A1c (HbA1c) (Menarini Diagnostici, Florence, Italy) (normal range, 3.5–5.5%; where 3.5% = 20.2 mmol/mol International Federation of Clinical Chemistry = 4.0% Diabetes Control and Complications Trial and 5.5% = 42.1 mmol/mol International Federation of Clinical Chemistry = 6.0% Diabetes Control and Complications Trial) were recorded. Patients were questioned regarding the number of hypoglycemic episodes they presented. NS and SH were defined following the American Diabetes Association criteria. 16 SH events were defined as those associated with neuroglycopenia severe enough to require treatment from a third party. The questionnaire of Clarke et al. 17 was used to evaluate hypoglycemia awareness. CGM for 72 h using the CGMS® System Gold™ from Medtronic Minimed (Northridge, CA, USA) was recorded within 2 weeks before initiation of CSII in order to describe the glucose profile. Glucose variability was evaluated calculating mean amplitude of glucose excursions (MAGE) designed by Service et al. 18 from continuous sensor readings. MAGE over 24 h is the mean of the absolute differences between glucose peak and nadir values in excess of at least 1 SD of the mean glucose.
Before initiation of CSII a hypoglycemia-induced test was performed as described previously. 19 Patients answered the Hypoglycemia Symptoms Score Questionnaire first after 30 min of euglycemia (80–120 mg/dL) and then after 30 min of being in hypoglycemia (45–55 mg/dL). 20 The test scores between the two states were compared, and the variation was expressed in a percentage. The same experimental protocol was performed in a control group of 20 subjects with T1D and similar characteristics (age, gender, disease duration, treatment, and absence of micro- or macrovascular complications) but with fewer than four NS events per week (in the last 8 weeks) and no SH episodes in order to compare the response to hypoglycemia.
Quality of life (QoL) assessment was performed using two different questionnaires: the Diabetes Quality-of-Life (DQoL) questionnaire, in which higher scores relate to deterioration in QoL, and the SF-12 health survey questionnaire.
All the subjects included in our study received our specific therapeutic education program for patients beginning CSII. They received a diet adjusted to their age and body mass index, and insulin doses were adjusted to maintain fasting and preprandial glucose levels between 90 and 130 mg/dL, postprandial below 180 mg/dL, and at bedtime between 100 and 180 mg/dL, based on four to six daily capillary blood determinations. Glucose targets and capillary glucose determinations were comparable to those used with MDI. Patients were encouraged to avoid values <70 mg/dL. The same team saw patients as required during the therapeutic education program and every 2–3 months thereafter until 24 months of follow-up. Patients were instructed on glucose goals and self-monitoring glucose control when necessary. All patients were using pumps with preprogrammable variable basal rates. After 6, 12, and 24 months of follow-up, all the subjects were evaluated for the number of hypoglycemic episodes (NS and SH) and with the questionnaire of Clarke et al. 17 At the end of the study, results obtained after 72 h of CGM, the Hypoglycemia Symptoms Score questionnaire during the hypoglycemia-induced test, and results of the DQoL and SF-12 questionnaires were again obtained.
Results are presented as mean ± SD values. Comparisons were performed using a paired Student's t test or an analysis of variance for repeated measurements. Comparisons between proportions were made with a χ2 test. A value of P < 0.05 was considered statistically significant. All statistical calculations were performed by the Statistical Package for Social Science (version 14.0) for personal computers (SPSS, Inc., Chicago, IL).
Results
A total of 20 subjects with NS and SH were included in the study, and their clinical and metabolic characteristics at baseline are shown in Table 1.
Data are mean ± SD values. BMI, body mass index; HbA1c, hemoglobin A1c; MDI, multiple daily injections; M/W, men/women; UAE, urinary albumin excretion.
At the time of the inclusion in the study, 19 subjects (one was non-classified) were shown to have hypoglycemia unawareness according to the Clarke test (score: ≥4 = unawareness, 3 = non-classified, ≤2 = awareness), scoring on average 5.45 ± 1.19. Progressively, we observed a decrease in the Clarke test score: 3.70 ± 1.65, 2.74 ± 1.06, and 1.6 ± 2.03 after 6, 12, and 24 months of follow-up, indicating an improvement in the hypoglycemia unawareness towards normal awareness (P < 0.001 for baseline vs. 24 months). At the end of the follow-up, only three of the 20 subjects were classified as having hypoglycemia unawareness. In absolute terms, the evolution of hypoglycemia awareness categories is shown in Figure 1.
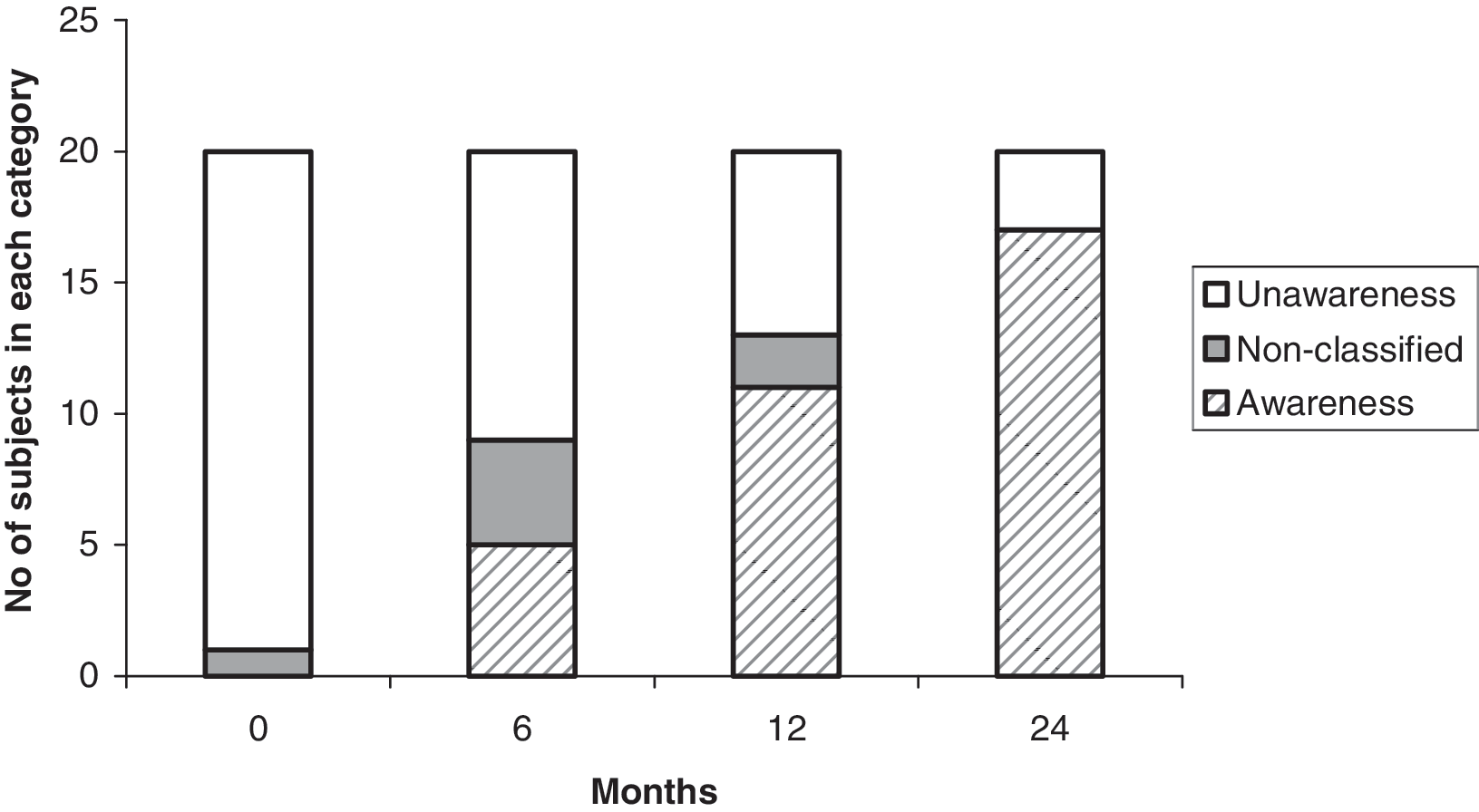
Number of subjects in each category of the Clarke test during the follow-up.
The mean number of episodes of NH per week progressively diminished from 5.40 ± 2.09 at baseline to 4.60 ± 2.33, 3.07 ± 1.39, and 2.75 ± 1.74 after 6, 12, and 24 months, respectively (P < 0.001 for baseline vs. 24 months). When the number of SH episodes were analyzed, they fell from 1.25 ± 0.44 per subject year at baseline to 0.05 ± 0.22 at the end of the follow-up (P < 0.001). Additionally, HbA1c remained unaltered during the follow-up: 6.6 ± 1.0%, 6.7 ± 0.9%, 6.7 ± 0.8%, and 6.3 ± 0.9% for baseline, 6, 12 and 24 months, respectively.
Considering data obtained from the CGMS, after the 24-month follow-up, the percentage of values within target levels (70–180 mg/dL) increased (53.2 ± 11.0% to 60.3 ± 17.1%, P = 0.13), and the percentage of values below 70 mg/dL decreased (13.7 ± 9.4% to 9.1 ± 5.2%, P = 0.07); however, these tendencies did not reach statistical significance. MAGE diminished after 24 months of CSII from 136 ± 28 to 115 ± 19 mg/dL at 24 months of follow-up (P < 0.02).
At baseline, subjects with NS and SH scored 31.6 ± 16.4 on the Hypoglycemia Symptoms Score Questionnaire during hypoglycemia, representing a rise of 52% in comparison to euglycemia (21.0 ± 3.15). At 24 months after initiating CSII, the score was 62.3 ± 23.6 (P < 0.001, in comparison to baseline), an increase of 196% (P < 0.001, in comparison to baseline) with respect to euglycemia (21.05 ± 3.15). These results were compared with those obtained in the control group (33.5 ± 8.7 years old; 12 women; 14.0 ± 6.5 years of duration of the disease; all of them on MDI; HbA1c = 6.7 ± 0.7%; difference not significant) under the same conditions of glycemia levels in the euglycemia and hypoglycemia periods. The score on the Hypoglycemia Symptoms Score questionnaire was 54.5.6 ± 18.4 during hypoglycemia, representing a rise of 163% in comparison to euglycemia (20.5 ± 1.9). This response was not different from that observed in T1D subjects with NS and SH after 24 months of treatment with CSII.
Regarding QoL outcomes, a significant improvement in all the aspects evaluated by DQoL test was observed. This was also the case for the results obtained by the SF-12 health survey questionnaire (Table 2).
DQoL, Diabetes Quality of Life.
Discussion
Our study shows that the use of CSII in T1D subjects with a history of recurrent hypoglycemia and SH leads to a persistent diminution in number of hypoglycemic episodes, as well as to a sustained improvement in hypoglycemia awareness, even though there were no change in HbA1c, and the percentage of glycemic values within target levels and below 70 mg/dL remained without significant change.
Hypoglycemia in T1D is the consequence of the nonphysiological replacement of insulin even when using the theoretically physiological basal-bolus approach. Since the Diabetes Control and Complications Trial results, there is no doubt that intensive insulin therapy effectively delays the onset and slows the progression of diabetic retinopathy, nephropathy, and neuropathy in patients with T1D. 1,2 However, the price to pay is an increase in NH and SH episodes (two- to threefold). Mild hypoglycemia, if recurrent, induces unawareness of hypoglycemia, which impairs glucose counterregulation and predisposes to SH. A very recent survey of a large hospital-based population confirmed that there is still a significant proportion of people with T1D (around 20%) who suffer from hypoglycemia unawareness. 21 Thus, despite modern patient education and improvements in the strengthening of insulin therapy, hypoglycemia and hypoglycemia unawareness are still far from solved in T1D.
In patients with repeated hypoglycemia and hypoglycemia unawareness, the meticulous prevention of hypoglycemic episodes can reverse the physiological abnormalities associated with this condition. 22 –24 In order to create more successful clinical management of T1D, the implementation of a more physiological pattern of insulin replacement therapy, including the use of real-time CGM, as has been demonstrated in some long-term studies, is necessary. 25 –30 However, there is no consensus on which, if any, should be the preferable, suitable, and efficient approach.
In our study, probably by effectively diminishing the number of hypoglycemic episodes, the use of CSII was associated with a shift from abnormal perception of hypoglycemia to a normal awareness. This is true, not only in experimental conditions of a controlled-induced hypoglycemia but also in clinical assessment using specific tools. It should be underlined that these results were obtained without a deterioration of glycemic control in terms of HbA1c. Furthermore, the results provided from CGM are in agreement with these findings showing a tendency to a diminishing of values of glycemia <70 mg/dL, an increase in the percentage of values within target levels, and a significant improvement in the variability in glucose profile. In addition to this, it should be noted that all these beneficial effects of CSII come not with a detrimental effect but with an improvement in all aspects of quality of life.
Fatourechi et al. 13 in a very recent systematic review and meta-analysis commissioned by the Hypoglycemia Task Force of The Endocrine Society examined the best available evidence about the use of CSII and MDI as intensive insulin replacement therapies and the risk of hypoglycemia. Including 15 recent randomized control trials the authors concluded that CSII was associated with a slightly lower HbA1c without a significant difference in terms of hypoglycemia. Nevertheless, the investigators recognized that these results came from patients at a low risk of hypoglycemia and that therefore they cannot be fully extrapolated in patients with recurrent SH or hypoglycemia unawareness.
In absolute terms, and acknowledging the differences between both studies, the magnitude of restoration of hypoglycemia awareness achieved in our study using CSII is quite similar to that observed by Leitão et al. 31 using islet transplantation. However, it does not seem clear to us if the improvement observed in hypoglycemia awareness in that study is really due to a diminishing of number of hypoglycemic episodes as data on that subject are not described in their article.
We are well aware of the limitations of our study. Mainly, there is no control group, and it includes a relatively small number of high-risk subjects for hypoglycemia in whom the beneficial effect of CSII option could be exacerbated. However, prior to the initiation of CSII, all of our patients had been included in our specific diabetes education program for patients receiving conventional intensive insulin treatment and poor metabolic control with no benefit with regard to hypoglycemia. Considering the very disabling and labile profile of our patients and in light of the indications and criteria from the Catalan National Health Service authorities and guidelines, we did not consider maintaining MDI therapy to any further extent. In this topic, very recently the new guidance from the National Institute for Health and Clinical Excellence on CSII for the treatment of diabetes mellitus recommended this type of therapy as a treatment option in T1D subjects who attempt to achieve target HbA1c values with intensive insulin therapy but experience repeated and unpredictable occurrences of hypoglycemia (
In summary, CSII may persistently prevent hypoglycemic episodes, improve hypoglycemia awareness, and ameliorate the glycemic profile in T1D subjects with repeated SH. Moreover, its use is associated with an improvement in diabetes QoL aspects.
Footnotes
Acknowledgments
We are indebted to all of those involved at any time in the specific therapeutic education program for patients beginning CSII at the Endocrinology and Diabetes Unit of the Hospital Clínic i Universitari of Barcelona (colloquially called “Programa Bombas”). M.G. is the recipient of a grant from the Hospital Clínic i Universitari of Barcelona. This work was supported in part by a grant (PI060250) from the “Ministerio de Sanidad y Consumo” of Spain. Medtronic Ibérica sponsored this work, in part.
Author Disclosure Statement
No competing financial interests exist.