
Abstract
Background:
This study reports on the effectiveness of exenatide compared to insulin glargine or NPH insulin in patients with type 2 diabetes mellitus, unable to achieve glycemic control with oral glucose-lowering therapies in a clinical care setting.
Patients and Methods:
Patients with type 2 diabetes mellitus (n = 47) whose glycemia was not controlled adequately with oral hypoglycemic agents at maximum recommended therapeutic doses were initiated on exenatide therapy. Age-, sex-, and body mass index-matched patients receiving insulin glargine (n = 54) or NPH insulin (n = 23) served as controls. Data analysis included glycated hemoglobin, fasting and postprandial plasma glucose, lipid profile, body weight, and the occurrence of hypoglycemia.
Results:
A statistically significant reduction in glycated hemoglobin value was noted after initiating exenatide (pre-exenatide 9.7 ± 1.4% vs. post-exenatide 8.7 ± 1.5%; P < 0.05), which was comparable to values after insulin glargine (9.8 ± 1.1% vs. 9.0 ± 1.5%, respectively; P < 0.05) and NPH insulin (9.6 ± 1.4% vs. 8.9 ± 1.3%, respectively; P < 0.05). Exenatide therapy was associated with net weight loss (mean, 1.6 kg), but therapy with insulin glargine and NPH insulin was associated with weight gain (1.8 and 2.3 kg, respectively).
Conclusions:
In a group of select Asian Indian type 2 diabetes patients with secondary failure to oral hypoglycemic agents seen at a diabetes center, exenatide treatment in combination with oral drug regimens resulted in significant lowering of glycated hemoglobin similar to insulin glargine or NPH insulin but with the additional benefit of weight loss, albeit a small amount.
Introduction
Abnormalities in the incretin axis as well as elevated glucagon levels have been shown to play an important role in the pathogenesis of T2DM. As glucagon-like peptide-1 (GLP-1) deficiency occurs early in the natural history of T2DM, GLP-1 replacement therapy is a logical choice. 3 Exenatide is the first in the series of GLP-1 receptor agonists approved as adjunctive therapy to improve glycemic control in patients with T2DM who have not achieved adequate glycemic control with oral hypoglycemic agents (OHAs). In controlled clinical trials, exenatide improved glycemic control and significantly reduced body weight in obese patients with inadequately controlled T2DM. 4 –13
Although controlled clinical trials have clearly shown the efficacy of exenatide in type 2 diabetes patients, there is limited information in Asians in general and in particular Asian Indians. 14,15 However, most published data were based on randomized clinical trials in which patients were selected based on rigorous inclusion/exclusion criteria. There are relatively few studies carried out outside of clinical trials in clinical practice setup. 16,17 Moreover, to our knowledge there are no studies in Asian Indians that directly compared exenatide with insulin therapy in secondary OHA failure cases.
The objective of this study was therefore to review the effectiveness of exenatide on glycemic control and body weight compared to insulin glargine and NPH insulin in patients with T2DM with secondary failure to OHAs. Insulin preparations were used as the comparator drug because addition of insulin is a common practice in the face of secondary failure to OHAs. 18
Patients and Methods
Study design
This study was an open-label, non-randomized, retrospective study carried out at Dr. Mohan's Diabetes Specialities Centre, a tertiary care diabetes center in Chennai (formerly Madras), a city in southern India, between March 2008 (the time when exenatide became commercially obtainable in India) and March 2009.
Patients
The charts of patients who were prescribed exenatide for control of T2DM as part of routine care by the physicians of our center and whose glycemia was not controlled adequately by metformin, a sulfonylurea, or a combination of both were reviewed. Age-, sex-, and body mass index (BMI)-matched patients who received either insulin glargine or NPH insulin for secondary failure to OHAs served as the controls.
Medications
Patients who were prescribed exenatide used a multiuse pen (Byetta®, Eli Lilly Co., Gurgaon Haryana, India) to subcutaneously inject (within 15 min before morning and evening meals) a fixed dose of 10 μg twice daily. If frequent nausea developed (daily episodes for >1 week in duration), patients had the option to decrease their dose to 5 μg twice daily. Patients in the comparator group self-injected insulin glargine once daily or NPH insulin once or twice daily. The doses of glargine and NPH were titrated against fasting blood glucose levels. OHA drug doses were fixed at prestudy levels unless patients experienced hypoglycemia when a reduction in dose was recommended.
Assessments
Anthropometric measures such as height (cm) and weight (kg) were measured using standard methods. 19 BMI was calculated using the standard formula: weight in kg divided by height in meters squared. The blood pressure was recorded twice 5 min apart in the right upper limb with the patient in the sitting position using a mercury sphygmomanometer, and the mean of the two was taken. A fasting blood sample was taken after ensuring a minimum of 8 h of overnight fasting for the estimation of fasting plasma glucose (FPG) as well as for other biochemical measurements. After stimulation by a standard breakfast 20 a second blood sample was drawn for estimation of postprandial glucose (PPG). All biochemical assays were done on a COBAS C 501 (Hitachi, Mannheim, Germany) using kits supplied by Roche Diagnostics (Mannheim). Glycosylated hemoglobin (A1c) was estimated by high-performance liquid chromatography using a Variant machine (Bio-Rad, Hercules, CA). Low-density lipoprotein cholesterol was calculated using the formula of Friedewald et al. 21
Outcome measures
The primary effectiveness variable was the change in A1c level and body weight from baseline. Effectiveness was assessed as “good” if the A1c level was <7%, “fair” if between 7.1% and 8.5%, and “poor” if >8.5%. The secondary effectiveness variables were the change from baseline in FPG, PPG, and blood pressure, serum creatinine level, and lipid profile.
Responder analyses were performed to determine the number of patients achieving the American Diabetes Association target of A1c <7.0%. In addition, the number of patients whose A1c level decreased by at least 0.5% was assessed.
Safety
Adverse events were assessed at each visit by using an open-ended questionnaire. Patients were also asked whether they had experienced hypoglycemia since their previous visit. Severity of each event (mild, moderate, or severe) and its attribution to therapy (yes or no) were assessed by the physician. Symptomatic hypoglycemia was defined as a blood glucose measurement less than 3.4 mmol/L (≤60 mg/dL) and/or symptoms such as excessive hunger, sweating, shaking, palpitation, or confusion. Severe hypoglycemia was defined as a hypoglycemic episode in which the patient required assistance from another person or had a blood glucose measurement less than 2.8 mmol/L (≤50 mg/dL). The patients were specifically asked about symptoms of acute pancreatitis such as abdominal pain, nausea, and vomiting. Furthermore, we also monitored the levels of serum amylase and lipase at periodic intervals.
All patients had given written permission to use the data for research purposes.
Statistical analysis
Data are presented as mean ± SD values. P < 0.05 was considered statistically significant. Standard descriptive analysis, independent-samples t test, and nonparametric tests were used where appropriate. Baseline was considered the visit when exenatide or insulin glargine or NPH was initiated. The final outcome was 24 weeks later.
Results
Patient characteristics
The baseline demographic characteristics of study patients are shown in Table 1. All three groups were comparable at baseline, and there were no significant differences with respect to age, sex, weight, BMI, waist circumference, or duration of diabetes. Eleven subjects were on once-daily and 12 subjects on twice-daily NPH insulin.
Data are mean (SD) values except for sex [number (%)].
Effectiveness on glycemic control
The effectiveness of treatment on primary efficacy variables is reported in Table 2. Baseline mean A1c, FPG, and PPG levels were comparable among the treatment groups. There was a modest but statistically significant decline in A1c values in all three treatment groups, with the highest reduction occurring in the exenatide group. Although the A1c reduction in exenatide group was marginally greater than the other groups (1.0% vs. 0.8% for insulin glargine and 0.7% for NPH insulin), the differences were not significantly different between groups. There were no significant differences among the reductions achieved in the various groups with respect to FPG levels. PPG values were reduced by 30.5% compared to the baseline values in the exenatide group, which was significant statistically (P < 0.05). The corresponding values were 12.5% in the insulin glargine group (P > 0.05) and 10% in the NPH group (P > 0.05). Thus exenatide use was associated with a greater blunting of the rise in PPG concentration. Comparison of the proportion of participants achieving the American Diabetes Association target of <7.0% indicated that more patients treated with exenatide (seven [14.9%] vs. two [3.7%] in the insulin glargine group and one [4.3%] in the NPH insulin group) reached the American Diabetes Association target of <7%. Furthermore, 26 (55.3%) of the 47 patients treated with exenatide had a reduction of 0.5% in the level of A1c compared to 38.9% in the insulin glargine group and 43.5% in the NPH insulin group.
HbAlc, glycated hemoglobin.
P < 0.05.
Effectiveness on body weight
A mean weight loss from baseline of 1.6 kg was achieved in the patients treated with exenatide (98.3 kg before exenatide vs. 96.7 kg after exenatide), which did not reach the level of statistical significance (Fig. 1). On the other hand, patients treated with insulin glargine and NPH insulin gained weight, resulting in a total treatment difference of 3.4 kg and 3.9 kg, respectively.
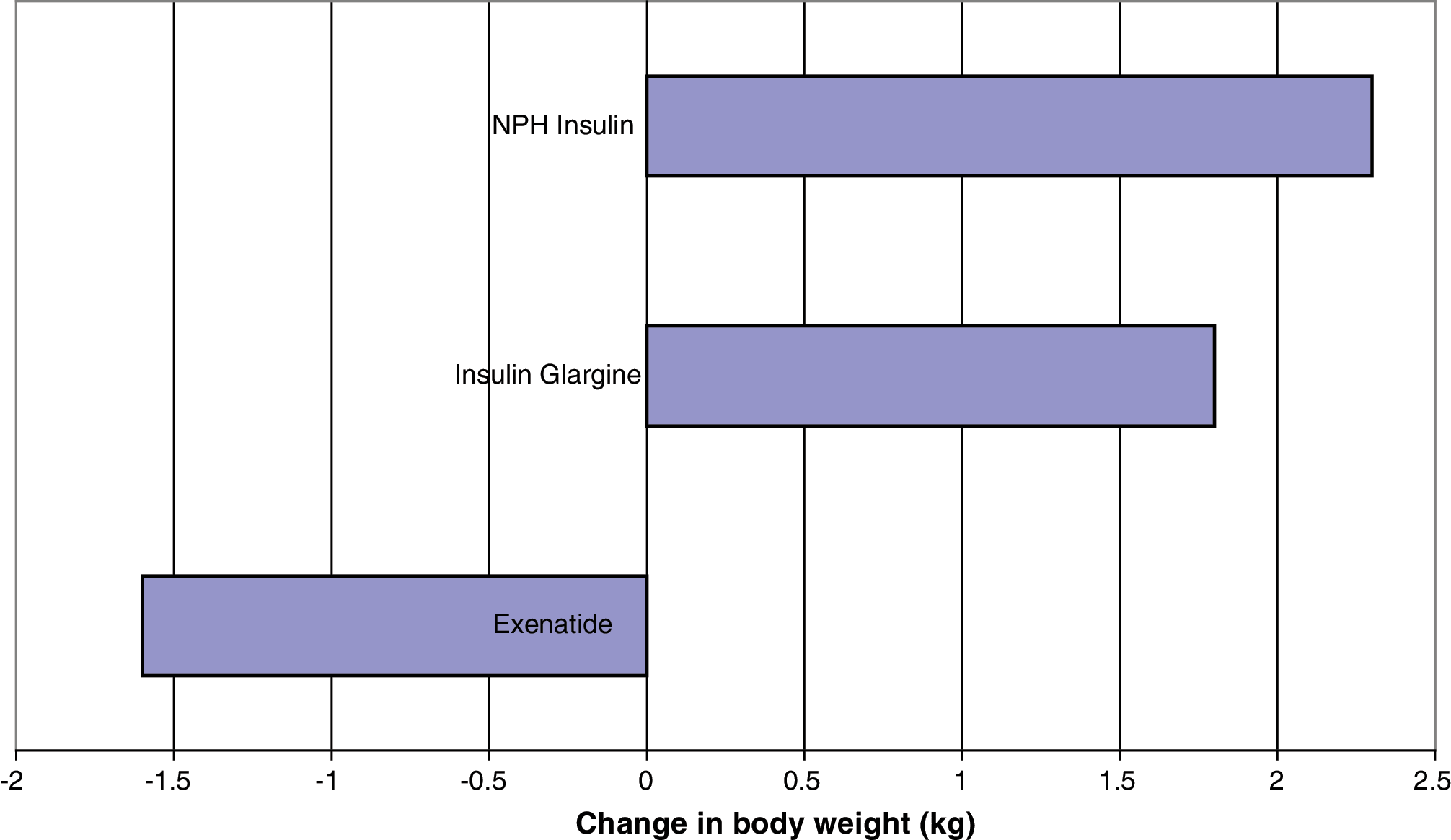
Change in body weight after exenatide, insulin glargine, and NPH insulin therapies. Color image available at
Efficacy on secondary efficacy profiles
Systolic and diastolic blood pressures remained unchanged in the three groups. There were no significant changes in the three groups with reference to lipid profile, although a small reduction in high-density lipoprotein cholesterol level was observed in the exenatide group (Table 3).
Data are mean (SD) values. HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Safety
A total of seven patients had hypoglycemic episodes (two in the exenatide group, three in the insulin glargine group, and two in the NPH insulin group), but none was a severe episode. Ten patients in the exenatide group had nausea, in two of whom it was severe; however, in all patients nausea disappeared on continued treatment. None of the patients taking exenatide presented with symptoms or signs of acute pancreatitis.
Discussion
Our study reports on the results of the addition of exenatide to patients with T2DM with secondary failure to OHAs in a clinic practice setting in comparison with glargine or NPH insulin. Our findings are in agreement with the results of randomized clinical trials comparing the effects of exenatide and insulin glargine on glycemic control in patients with type 2 diabetes. 8,10 Because comparative effectiveness studies are a valuable tool for assessing the effectiveness and safety of drugs in a wide and heterogeneous population, away from the confines of randomized controlled clinical trials, 22,23 the present study provides complementary information to physicians about the usage of exenatide in a select group of Asian Indians.
Exenatide and insulin glargine use was associated with improved glycemic control in type 2 diabetes patients with inadequate glycemic control and a BMI of around 31 kg/m2. 8,10 A modest reduction in A1c was observed after treatment with exenatide in the present clinical care setting study in type 2 diabetes patients with very poor glycemic control but with higher BMI. Similar observations were made by Davies et al. 24 while evaluating exenatide in a population of overweight patients (BMI, 34.6 kg/m2) with type 2 diabetes who were at high risk of cardiovascular disease and not adequately controlled by two or three oral antidiabetes drugs, but with a lower basal A1c (8.7%).
Even though physicians continue to rely on FPG and A1c levels to guide management, 25 the role of postprandial hyperglycemia in the development of complications is becoming increasingly recognized. 26 –28 Reduction in postprandial hyperglycemia in T2DM patients has been shown to be associated with regression of carotid intima-media thickness, a validated surrogate cardiovascular end point. 29 Thus the greater blunting of postprandial hyperglycemia observed in the present study is an additional benefit of the drug.
Most of the established therapies for T2DM (e.g., sulfonylurea, thiazolidinedione, insulin) promote weight gain. 30 However, studies with exenatide have demonstrated significant reductions in body weight. 5 –7 It is gratifying to note that this body weight reduction was also observed in this study. Because the majority (80–90%) of the patients with type 2 diabetes are overweight or obese and because both type 2 diabetes and obesity are independent risk factors for cardiovascular disorders, this would be a distinct advantage for the usage of exenatide compared to insulin in patients with secondary failure to OHAs.
Treatment with GLP-1 and GLP-1 receptor agonists has been reported to increase blood pressure and heart rate in animal models. 31,32 Conversely, continuous infusion of GLP-1 produced small nonsignificant decrease in blood pressure in patients with T2DM. 33 Blonde et al. 34 reported a significant reduction in diastolic blood pressure while analyzing the effects of exenatide treatment on cardiovascular risk factors in 314 overweight patients with type 2 diabetes over a period of 82 weeks. Similarly, progressive reduction in blood pressure was reported by Buse et al. 35 while studying the metabolic effects of 2 years of exenatide treatment on patients with T2DM. However, there was no change in blood pressure in our study; it remains to be seen whether this is probably due to shorter duration of follow-up.
It is disappointing to note that the control of glycemia remained poor in all the three groups. This could be probably due to the fact that because our center is a tertiary center, patients who were uncontrolled with routine therapies get referred here. Second, it shows that even at our center physicians were not aggressive enough with the treatment. It should be noted that this study is a clinic-based retrospective study and not a “clinical trial” where every effort is made to achieve target. Patient-related factors, e.g., lack of adherence to diet or exercise, could also have played a part.
The major strength of this study is that it is the first Indian experience with exenatide. One limitation of our study is that it spans only a few months, and long-term studies are needed. The benefits of exenatide if any need to be assessed in terms of cost, quality of life, and reduction in diabetes complications. It is pertinent to note that exenatide is an expensive drug with an average monthly cost of ranging from 7,000 rupees ($150 US) for 5-μg doses to 14,000 rupees (approximately $300 US) for 10-μg doses. As most patients in India have to pay for medicines from their pocket, in the absence of insurance and social security, this might seriously limit the number of people who can be offered exenatide therapy.
Conclusion
Exenatide in combination with existing oral drug regimens helps to improve glycemic control in patients with T2DM to some extent with the additional benefit of weight loss, albeit a small amount.
Footnotes
Acknowledgments
The authors wish to thank Mr. S. Santhanakrishnan of the Information Technology Department for extracting the data for this study.
Author Disclosure Statement
The authors declare no conflict of interest exists.