
Abstract
Bariatric surgery is now widely reported to ameliorate or resolve type 2 diabetes mellitus in adults. Some clinical investigators even suggest its use as an early therapeutic intervention for type 2 diabetes in patients not meeting standard criteria for bariatric surgery. However, little is known about the exact mechanisms explaining the metabolic consequences, and much active investigation is underway to identify hormonal changes leading to diabetes resolution. This review includes a detailed description of various bariatric surgical procedures, including the latest less-invasive techniques, and a summary of current data providing insight into the short- and long-term metabolic effects. We outline current hypotheses regarding the mechanisms by which these surgical procedures affect diabetes and report on morbidity and mortality. Finally, we discuss the available data on bariatric surgery in adolescent patients, including special considerations in this potentially vulnerable population.
Introduction
Bariatric surgical procedures: (
At the first World Congress on Interventional Therapies for Type 2 Diabetes, held in September 2008, a number of experts in the surgical treatment of obesity and in the field of obesity research called for a consensus on the use of bariatric surgery to treat T2D. 10 Indeed, surgeons and some endocrinologists are now suggesting that clinicians refer patients who have T2D with a body mass index (BMI) below traditional criteria for bariatric surgery, based on limited evidence that even in this subgroup, glucose tolerance improves and oral medications will no longer be necessary for diabetes management. 11 In addition, as the use of bariatric surgery of all types increases in the adult population, it has become more widely accepted as an option for obese adolescents. 12,13
Indications for Bariatric Surgery
Indications for bariatric surgery in the management of obesity were initially outlined by the 1991 National Institutes of Health Consensus Development Panel. 14 Patients potentially eligible for bariatric surgery included those who (1) were well informed and motivated, (2) had a BMI >40 kg/m2, (3) had acceptable risk for bariatric surgery, and (4) had failed previous attempts at nonsurgical weight loss. The consensus statement also suggested that individuals over 18 years of age with a BMI >35 kg/m2 with obesity-related co-morbidities (diabetes, sleep apnea, obesity-related cardiomyopathy, or severe joint disease) may be candidates as well.
Bariatric surgery is contraindicated in patients with untreated major depression, psychosis, binge eating disorders, current drug and alcohol abuse, or severe cardiac disease or in those who have other major anesthesia-related risks, severe coagulopathy, or an inability to comply with nutritional requirements such as lifelong vitamin replacement. Bariatric surgery in children under 18 years of age remains controversial and will be discussed later in this article.
Surgical Procedures
LAGB
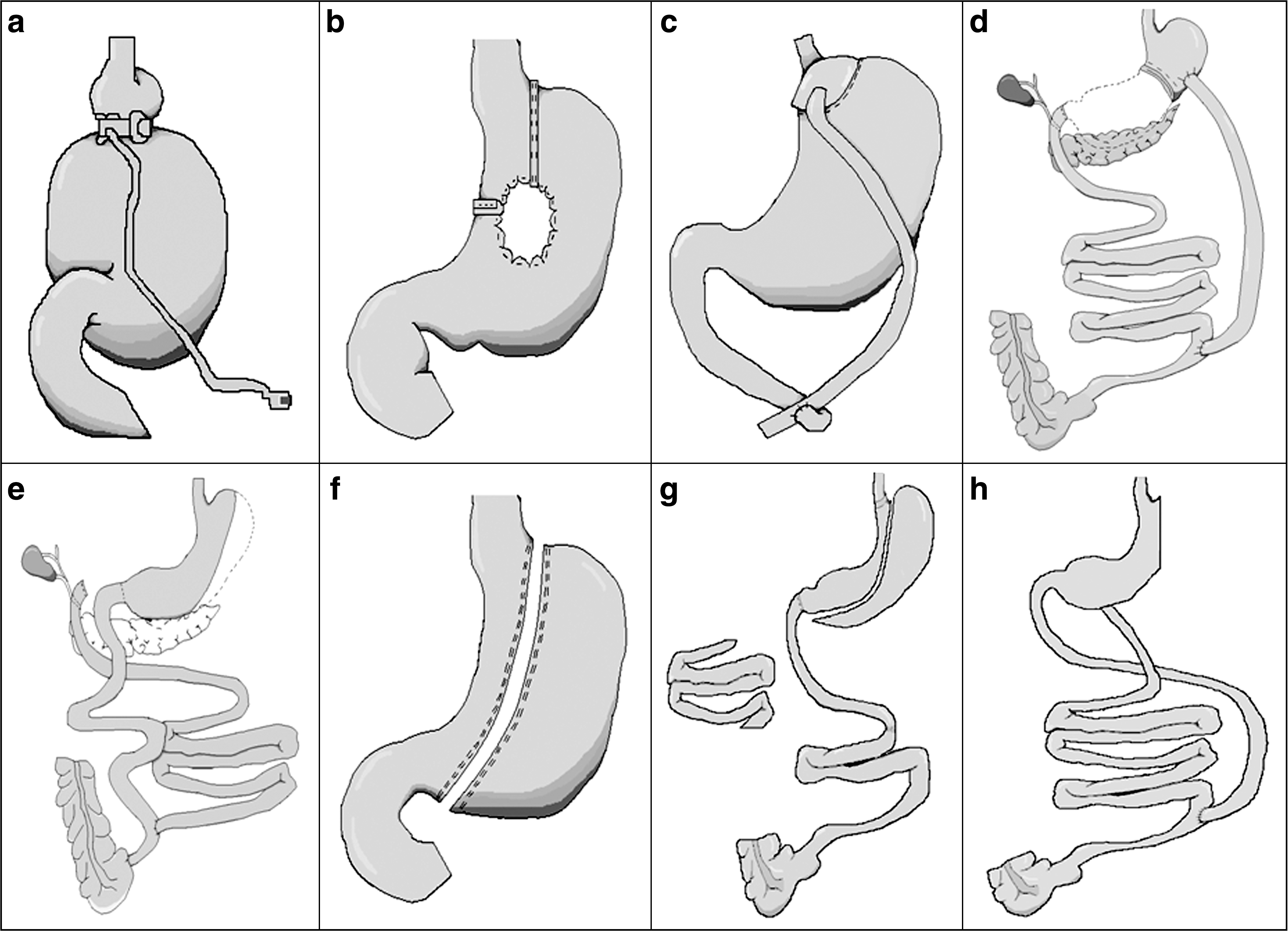
LAGB is a purely restrictive procedure in which a silicone device with a band and inflatable balloon is placed around the upper portion of the stomach (Fig. 1a). The band compartmentalizes the proximal stomach, creating a small gastric pouch (approximately 30 mL), and connects to a subcutaneous injection port. The outlet diameter into the remainder of the stomach is adjusted by injecting or removing fluid from the access port. 15,16 For example, when weight loss plateaus, the band is inflated further, thus impeding the passage of food into the distal stomach. Bleeding, infection, leakage, and gastric perforation are the major risks, requiring reoperation at rates of 2–8.9%. 15 Rarely, the portion of the stomach distal to the band may herniate, causing an obstruction (“slipped” band).
VBG
VBG is another purely restrictive procedure. A small pouch of 50 mL or less is created to reduce the flow of food to the distal stomach (Fig. 1b). The gastric pouch is generally stapled, cut, and divided from the remainder of the gastric fundus, and the stoma is covered with polypropylene mesh to prevent any expansion. 16 The risks of VBG include bleeding, infection, leakage, perforation, anastomotic stenosis, and internal hernia/small bowel obstruction. 15 Patients may also develop a foreign-body reaction to the mesh material, and dilation of the stoma may lead to weight regain.
RYGB
The RYGB procedure has both malabsorptive and restrictive components and remains the gold standard for bariatric surgery in the United States. The procedure consists of three basic steps. First, a 15–30-mL gastric pouch is created, accounting for the restrictive component. A separate biliopancreatic limb is then fashioned, extending about 50 cm from the ligament of Treitz to allow passage of biliary and pancreatic secretions until they are mixed with chyme at the distal anastomosis (Fig. 1c). Finally, part of the jejunum measuring approximately 75–150 cm in length is brought up to the gastric pouch to carry food from the pouch to the distal anastomosis. The malabsorptive aspect arises primarily from the delay in mixing of chyme and digestive enzymes. 16 This surgery is now primarily done laparoscopically. Complications particular to the RYGB include anastomotic leaks and gastric perforation, although these are reported in <5% of cases, and in some centers at rates of <1%. 15 Nutritional problems occur in many patients and include deficiencies of iron (20–49%), vitamin B12 (26–70%), and folate (9–35%); anemia due to these deficiencies may be present in 18–54% of patients who have undergone RYGB. 17
BPD and BPD with duodenal switch
The BPD and BPD with duodenal switch (BPD/DS) procedures also include both malabsorptive and restrictive components. A partial gastrectomy is performed, leaving a 150–200-mL gastric pouch. About 150–200 cm of ileum is used as the enteric limb to carry chyme from this pouch to the distal anastomosis and common channel. The alimentary limb may be anastomosed either to the proximal stomach after distal gastrectomy (BPD, Fig. 1d) or to the duodenal stump, preserving the pylorus (BPD/DS, Fig. 1e). The BPD/DS variant may reduce symptoms of dumping, including epigastric pain, nausea, palpitations, sweating, dizziness, and malnutrition. 16,18,19 Side effects of the procedure are similar to those of other bariatric surgeries and include leakage, anastomotic problems, and nutritional deficiencies at similar rates as with RYGB.
Sleeve gastrectomy
The laparoscopic sleeve gastrectomy was originally conceived as a first stage for achieving weight loss in superobese (BMI >60 kg/m2) patients and those with severe co-morbidities to reduce perioperative morbidity and mortality. 20,21 The procedure is relatively new, initially described in 2003 22 (Fig. 1f). It was often a first step prior to duodenal switch or RYGB, or a rescue after another failed bariatric procedure, 20,23 but it has become the primary choice of some surgeons, replacing gastric banding.
Emerging Technologies
Ileal interposition with sleeve gastrectomy
Ileal interposition with sleeve gastrectomy (or a variant—ileal interposition with diverted sleeve gastrectomy) involves the placement, or interposition, of a segment of ileum into the proximal jejunum (Fig. 1g). After sleeve gastrectomy, a silicone band is placed 3–4 cm below the gastric cardia and adjusted according to the desired diameter of the gastric pouch. The jejunum is then divided from the ligament of Treitz, and a 100-cm ileal segment is removed about 50 cm proximal to the ileocecal valve. This ileal segment, with its vascular and nervous supplies intact, is surgically interposed into the proximal jejunum, greatly increasing the exposure of the ileal segment to relatively undigested nutrients. The operation is hypothesized to be superior to purely restrictive gastric procedures by diminishing associated gastroesophageal reflux and avoiding the significant malabsorption present in procedures that include small intestinal bypass. 24
Santoro III
Initially in 2003 and subsequently in 2006, Santoro et al. 25,26 proposed a new surgical strategy for extreme obesity that combines preexisting surgical procedures. The technique consists of laparoscopic sleeve gastrectomy and enteroomentectomy, reducing gastric capacity to about 150 mL and the small bowel length to just 3 m, and preserving the distal small bowel (Fig. 1h). 13 The principle behind omentectomy is to reduce the amount of visceral adiposity, known to be generally associated with the development of the metabolic syndrome. 27
Additional methods
Other, less invasive techniques such as endoluminal duodenal sleeve placement are currently under study. 10
Morbidity and Mortality
In the comprehensive meta-analysis of bariatric surgery and obesity co-morbidities by Buchwald et al., 3 operative mortality at ≤30 days after surgery was 0.1% for purely restrictive surgeries, 0.5% for gastric bypass procedures, and 1.1% in biliopancreatic diversion or duodenal switch operations. Other published series of the RYGB procedure report postoperative mortality rates as low as 0.25%. 8,28 Thus, there remain major differences between surgical techniques and individual centers.
Data regarding postoperative re-hospitalization and morbidity outcomes are more difficult to assess. Severe obesity itself is a risk factor for adverse events following surgery 28,29 ; it therefore follows that patients undergoing bariatric surgery are by definition at risk for postoperative complications, even as they reduce their risk of obesity-associated co-morbidities in the long-term. The short-term risk of mortality for the average patient having bariatric surgery (40 years old, 80% female, BMI of 47 kg/m2) may be low, 30 but subgroups of patients may experience a 30-day mortality risk of 2.0% or more. 3 This especially applies to patients with a BMI >50 kg/m2, those over 65 years of age, those with multiple co-morbidities, and patients who are beneficiaries of Medicaid or Medicare. 30 –32 Between 10% and 20% of patients undergoing bariatric surgery may have a perioperative medical or surgical complication. 33 This is countered by evidence of increased longevity following bariatric surgery: obese diabetes patients in the Swedish Obesity Subjects Study had 9% mortality at 9 years; the control group had 28% mortality, most of which could be attributed to cardiovascular disease. 3,28 Table 1 lists potential complications following bariatric surgery.
T2D Outcomes
In general, studies of bariatric surgery and T2D define “resolution” of T2D as the ability of patients to discontinue all diabetes-related medications and maintain blood glucose levels within the normal range postoperatively. In the meta-analysis by Buchwald et al. 3 of studies reporting on diabetes resolution, 1,417 of 1,846 patients (76.8%) experienced complete resolution. Regardless of procedure type, patients experienced significant reductions in hemoglobin A1c, fasting glucose, and fasting insulin in the short-term (<6-month) follow-up period.
In general, restrictive-malabsorptive procedures have higher diabetes remission rates than purely restrictive procedures. Rates as high as 98.9% have been reported for biliopancreatic diversion or duodenal switch, 34 although it should be noted that far fewer patients have undergone this procedure compared to RYGB or gastric banding. In a 2008 study 35 using BPD, the percentage of patients cured of diabetes (fasting serum glucose reduced to ≤110 mg/dL, without dietary restriction and without medical therapy) was 74% at 1 month, 97% at 1 and 10 years, and 91% at ≥20 years. The 26% of patients not cured at 1 month were those with the most severe T2D preoperatively. A more recent randomized controlled trial of medical therapy versus gastric banding for T2D demonstrated a 73% remission rate (defined as hemoglobin A1c levels <6.2%, fasting glucose <126 mg/dL, and cessation of diabetes medications) in the group undergoing gastric banding at 2 years. 36 Other studies have shown that euglycemia and normal insulin levels occur within days after surgery, and these effects persist. 1,2
Hypotheses on the Resolution of T2D
Resolution of diabetes following bariatric surgery is predominately caused by marked weight loss resulting in improved insulin sensitivity. However, the beneficial effects of bariatric surgery on glucose metabolism cannot be accounted for entirely by weight loss. This is best demonstrated by the observation that in many gastric bypass patients, resolution of diabetes occurs within 1 week following bariatric surgery, before any clinically significant weight loss. 37 –41 Rapid resolution of hyperglycemia in these patients may be due in part to acute caloric restriction in the immediate postoperative period. Severe caloric restriction has long been known to improve glycemia control in patients with diabetes and was used therapeutically for type 1 diabetes prior to the discovery of insulin.
Several researchers have suggested that the rapid resolution of diabetes following malabsorptive bariatric procedures is due to bypass of the proximal small intestine, through as-yet unclear mechanisms (the “foregut hypothesis”). This hypothesis is supported by data showing higher rates of rapid diabetes resolution in patients undergoing malabsorptive bariatric surgery (which involves bypass of the proximal small intestine) versus those undergoing purely restrictive procedures (e.g., gastric banding), in which the flow of nutrients through the small intestine remains intact. 4,42 In addition, there are recent reports of duodenal bypass (without the restrictive component of the surgery) curing T2D in nonobese humans. 43
Another hypothesis (the “hindgut hypothesis”) for rapid diabetes resolution suggests that early contact of distal bowel with relatively undigested food enhances some signal that results in improved glucose metabolism. Incretins (such as glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide), hormones secreted by the gastrointestinal tract that increase insulin secretion in response to oral, but not intravenous, nutrients, are likely candidates accounting for part of this improvement. Our understanding of these changes is complicated by the observation that incretins, as well as other gastrointestinal hormones (oxyntomodulin, cholecystokinin, ghrelin, peptide YY), appear to be affected differently by various surgical procedures due to variations in anatomical rearrangements. Even minor changes in surgical technique, such as differing lengths of connecting jejunal limbs, can affect metabolic outcomes and may explain the, at times contradictory, findings in the existing literature.
The influence of gastrointestinal hormones on insulin sensitivity following bariatric surgery cannot be discounted. This is a subject of much active investigation, although currently no consensus exists on the role of these hormones. Differences in surgical procedures, research methodologies, and hormonal assays all contribute to the discrepancies in circulating gastrointestinal hormone levels observed among studies. 44 However, one highly plausible reason for not only improved insulin secretion, but also higher insulin sensitivity, is the increase in glucagon-like peptide-1 response to oral glucose in gastric bypass patients. The latter is much more pronounced in surgical patients than in individuals with equivalent, diet-induced weight loss. 39 Beyond incretins, increased bile acid reabsorption may also improve insulin sensitivity. 45 Levels of serum bile acids are higher in humans with prior gastric bypass, suggesting a potential contribution to improved glucose and lipid metabolism.
Recently it has been shown in an animal model that improved insulin sensitivity resulted from enhanced gastrointestinal gluconeogenesis following bariatric surgery. 46 In mice, enterogastric anastamosis (an analog to RYGB), but not gastric banding, increased gastrointestinal gluconeogenesis. Thus, enteral glucose was secreted directly into the portal vein, resulting in decreased hepatic glucose production, as well as central nervous system signals to suppress food intake. Whether or not this mechanism plays a significant role in humans remains to be determined. Furthermore, rat studies demonstrated that duodenal exclusion reduced the capacity of the entire remaining intestine to absorb glucose. This may be due to down-regulation of the function of the Na+/glucose co-transporter SGLT-1. 47 Another intriguing area of novel research is the study of the gastrointestinal microbiome and its role in surgically induced metabolic changes. 48
For further reading, we recommend several excellent reviews. 49 –52
Bariatric Surgery in Adolescents
Few reports have described bariatric surgery outcomes in obese patients younger than 18 years of age. Typically, patient cohorts are small (<30 patients), and follow-up periods are short (<5 years). 53 –56 Even fewer data have been published on diabetes resolution in this age group. Much will be learned from a prospective natural history study similar to the Longitudinal Assessment of Bariatric Surgery (LABS), which records bariatric surgery outcomes in adults. Teen-LABS is now collecting coordinated epidemiological, clinical, and behavioral data on adolescent patients undergoing bariatric surgery. 57
Inge et al. 53 reported that extremely obese (mean BMI, 50 kg/m2) adolescents experienced significant weight loss and improvement in glucose tolerance after the RYGB procedure. The study was conducted in 11 adolescents (surgical arm) at five centers, and these patients were compared to 67 adolescents with T2D who were treated medically for 1 year. At 1 year, the surgical group had improved insulin resistance and cardiovascular risk factors compared to the medically treated group. The improvements are encouraging, but the effect of this procedure on patients with lower BMI and over longer follow-up requires further clarification.
LAGB is now gaining prominence as a means of treating obesity in adolescents. Because T2D remains a relatively rare disease in pediatrics, even among obese children, sufficient data do not exist to come to evidence-based conclusions. Al-Qahtani 55 conducted a retrospective review of all children and adolescents who underwent LAGB in his center between January 2003 and December 2005. Among the 51 patients (mean age, 16.8 years; mean BMI, 49.9 kg/m2), 15 had the metabolic syndrome. Frank T2D was present in seven patients, all of whom had disease resolution after a mean follow-up of 16 months. The author reported no postoperative complications, and patients were compliant with postoperative dietary protocols. A subsequent prospective study 58 in 73 adolescents who underwent LAGB demonstrated similar resolution of co-morbidities; five patients had impaired glucose tolerance that resolved by 1 year postoperatively. A study from the same group 59 focused specifically on improving metabolic status in adolescents who undergo LAGB. None of the patients had diabetes; 23% had impaired glucose tolerance, which resolved postoperatively. As in previous studies of LAGB, the procedure was well tolerated and safe, although emphasis was again placed on the need for adolescents to be well informed and well followed throughout the pre- and postoperative periods.
The first randomized controlled trial investigating LAGB versus lifestyle modifications in adolescents was recently published. 56 Twenty-one of 25 patients (84%) who underwent LAGB lost more than 50% of excess weight, compared to just three of 25 (12%) in the lifestyle group. None of the patients in the study had frank diabetes; 19 of 50 patients (38%) had the metabolic syndrome. LAGB was well tolerated and led to improved quality of life, but seven patients required eight operational procedures (33%) for surgical revision.
Discussion
While the surgical community is eager to adopt bariatric surgery in all patients with T2D who meet criteria, 10,60 there remains no consensus among the rest of the medical community. Part of the skepticism about bariatric surgery may result from the historical record of severe long-term complications caused by now-outdated bypass operations. For example, jejunoileal bypass surgery led to hepatic cirrhosis, thought to arise as a result of bacterial overgrowth in the blind-loop intestinal segment, leading to chronic hepatic inflammation from foreign antigens in the portal vein. 61
Additionally, although morbidity rates have improved, access to bariatric surgery remains sparse. Medicaid patients have limited access to bariatric procedures and had higher body mass and greater incidence of serious co-morbid conditions at outset. 62 Of patients worldwide who meet National Institutes of Health criteria for bariatric surgery, only about 1% undergo a surgical procedure.
For diabetologists and other physicians interested in considering referral for surgical intervention, evidence is growing for its use to promote the resolution or remission of T2D, but questions remain about surgical morbidity. Certainly, hormonal and anatomic considerations play a role in the improvement of glucose tolerance and insulin resistance, as demonstrated by the differential outcomes following various surgical procedures. For adolescent patients, pediatric endocrinologists and others eagerly await the results of the Teen-LABS study, but in the meantime must continue to extract meaningful clinical information from small pediatric and larger adult trials.
Finally, given the knowledge that so few qualified patients have access to bariatric surgery, especially in the developing world, it seems most reasonable to think of bariatric surgery as a model to better understand the physiology of appetite and glucose homeostasis. Elucidating the mechanisms underlying the improvements in obesity and diabetes following various surgical procedures may lead to a better understanding of the interplay between gastrointestinal anatomy and neuroendocrine hormones, potentially leading to the development of novel therapeutic targets for T2D.
Footnotes
Acknowledgments
This work was supported by the Intramural Research Program of the National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. We thank Leann Sutphin for her contributions to this manuscript.
Author Disclosure Statement
The authors have no financial or other conflicts of interest to disclose.