
Abstract
Aim:
This study evaluated the feasibility of insulin pump treatment in adolescent girls with type 1 diabetes mellitus (T1DM) and eating disorders (ED).
Methods:
Sixty-three girls >10 years old were included in the study. Forty-eight were treated with pump (no-ED-pump group); 15 had ED, of whom eight were treated with pump (ED-pump group), and seven were treated with multiple daily injections (MDI) (ED-MDI group).
Results:
Girls in the ED-pump group had higher hemoglobin A1c (HbA1c) compared to those in the no-ED-pump group both before and after pump initiation (P = 0.007). In the ED-pump group, levels 0–6 months after pump initiation were slightly but not significantly lower compared to baseline reference values (8.48% vs. 8.84%, respectively; P = 0.42). In the no-ED-pump group there was a significant decrease in HbA1c level 0–6 months after pump initiation (8.03% vs. 7.67%, respectively; P = 0.004). Thereafter HbA1c levels were not different from baseline reference on both groups. The rate of hypoglycemic episodes was similar in the ED pump and no-ED-pump groups (0.9 vs. 1.0 episodes per 100 patient-years, respectively). Prior to diagnosis of ED, mean HbA1c levels in the ED-pump group and the ED-MDI group were similar: 9.24 ± 1.25% versus 8.47 ± 1.30% (P = 0.51). In the time intervals after the diagnosis of ED, mean HbA1c level of all measurements in the eight girls in the ED-pump group was significantly lower compared with the seven patients in the ED-MDI group: 9.07 ± 1.33% versus 10.40 ± 2.01% (P = 0.04).
Conclusions:
Treatment with an insulin pump was feasible in girls with T1DM and ED and resulted in significantly lower HbA1c levels compared to the ED-MDI group.
Introduction
Since the completion of the Diabetes Control and Complication Trial, insulin pump therapy has been widely used. 8 Pump treatment has been shown to lower hemoglobin A1c (HbA1c) levels and to limit excessive weight gain in comparison to treatment with multiple daily injections (MDI), without increasing the risk of DKA. Furthermore, it reduces the frequency of severe hypoglycemic episodes and reportedly improves health-related quality of life. 9,10 In comparison to MDI, pump treatment provides greater flexibility in timing of meals and snacks and enhances patients' ability to control their own diabetes. Although pump treatment appears to be an appropriate option for patients with T1DM and ED, clinicians treating adolescent girls often need to decide whether pump therapy is suitable and safe because it may be associated with an increased risk for DKA or deterioration of metabolic control. We believe that randomized controlled studies lasting for several years will be extremely difficult to pursue, and hence we have aimed to evaluate our experience on the effect of long-term pump treatment on metabolic control in adolescent girls with both T1DM and ED in a retrospective chart review.
Patients and Methods
A chart review was conducted on 176 children and adolescents followed in the Juvenile Diabetes Clinic, Maccabi Health Care Services, Raanana, Israel. The following inclusion criteria had to be fulfilled for each patient entered into the study: diagnosis of T1DM, female, 10 years old or above, consecutive HbA1c measurements within intervals of about 3 months, pump treatment for at least 1 year, and no documented mental retardation or genetic syndromes. Out of 176 subjects followed in the clinic, 97 were girls, nine of whom were younger than 10 years at the completion of the study. Of the 88 eligible female subjects, a further 25 patients without ED treated by MDI were excluded. The final study population thus comprised 63 subjects who were classified as either no-ED group, all of whom were treated by pump (no-ED-pump group) (n = 48), or as ED group (n = 15, of whom eight received pump therapy [ED-pump group] and seven MDI [ED-MDI group]).
ED were diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). 11 Of the 15 girls diagnosed with ED, eight were classified with insulin omission, three with restrictive behavior, and four with binge eating behavior. Additional problematic eating behaviors and attitudes included weight loss or lack of appropriate weight gain according to age, refusal to be weighed in clinical visits, amenorrhea, being vegetarian, discordance between glucometer output and reported glucose levels, refusal to attend appointments with the dietician, and admitting to insulin omission for the purpose of weight loss. Insulin omission alone, without other clinical characteristics noted, was not considered as ED. None of the patients was diagnosed as having full-blown anorexia nervosa and bulimia nervosa. Five were treated or hospitalized in eating disorder/psychiatric units, three of whom with an additional diagnosis of depression. All others received continuous psychological care because of ED.
Data were obtained by chart review from the diagnosis of T1DM until the end of the study observation period (May 2007). To study the effect of pump treatment we used measurements obtained in the 24-month period prior to pump initiation and subsequently for a minimum of 1 year after start of pump treatment. Information was obtained at each visit (generally every 3 months) both prior to and after pump therapy was started. This information included HbA1c levels, DKA episodes, and episodes of severe hypoglycemia, which were defined according to the Diabetes Control and Complications Trial protocol to include coma, seizures, or any other inability to self-treat. 12 The study was approved by the institutional review board of Maccabi Health Care Services.
HbA1c was measured at each visit either by immunological in vitro assay (Tina-quant®, Boehringer Mannheim Systems, Mannheim, Germany) or by a fingerstick blood sample with the DCA 2000 analyzer (Bayer Inc., Tarrytown, NY) device following the manufacturer's guidelines.
In 25 subjects HbA1c measured from a fingerstick blood sample with the DCA 2000 analyzer was compared to measurements using the Tina-quant method. For each subject, the difference in measured HbA1c values (DCA 2000 value minus Tina-quant laboratory value) was computed. The paired t test was used to compare the mean values. DCA 2000 levels correlated well with laboratory values (r = 0.88, P < 0.001) but tended to be slightly higher (8.74 ± 1.34% vs. 8.56 ± 1.26%). The mean difference of DCA 2000 and laboratory HbA1c values was 0.2% (95% confidence interval, −0.1–0.6 %). Our findings are in correlation with previous works comparing the two methods. 13 In the current study HbA1c values obtained by either of the methods were considered.
Statistical analyses
Statistical analyses were performed with SAS version 9.1 (SAS Institute Inc., Cary, NC). Descriptive statistics are presented as mean ± SD values and were compared by Student's t test. All tests were two-sided, and P values < 0.05 were considered statistically significant. For comparing between the ED group treated by insulin pump with the no-ED group treated by insulin pump, the mean value of all HbA1c measurements for each patient for each time period was used in analyses. The mean HbA1c levels were assessed at three time intervals prior to pump initiation (2 to ≤1 years, 1 year to ≤6 months, and in the 6-month period) and at six time intervals after pump initiation (0 to ≤6 months, 6 months to ≤1 year, 1 to ≤2 years, 2 to ≤3 years, 3 to ≤4 years, and 4 to ≤5 years).
Mean values of HbA1c in Figure 1 were calculated using 345 observations of 56 subjects (68 observations of eight patients in the ED-group and 277 observations of 48 patients in the no-ED group). All differences between mean levels of HbA1c were analyzed with the generalized estimating equations method to account for correlated observations (SAS GENMOD procedure with REPEATED statement using autoregressive correlation matrix).
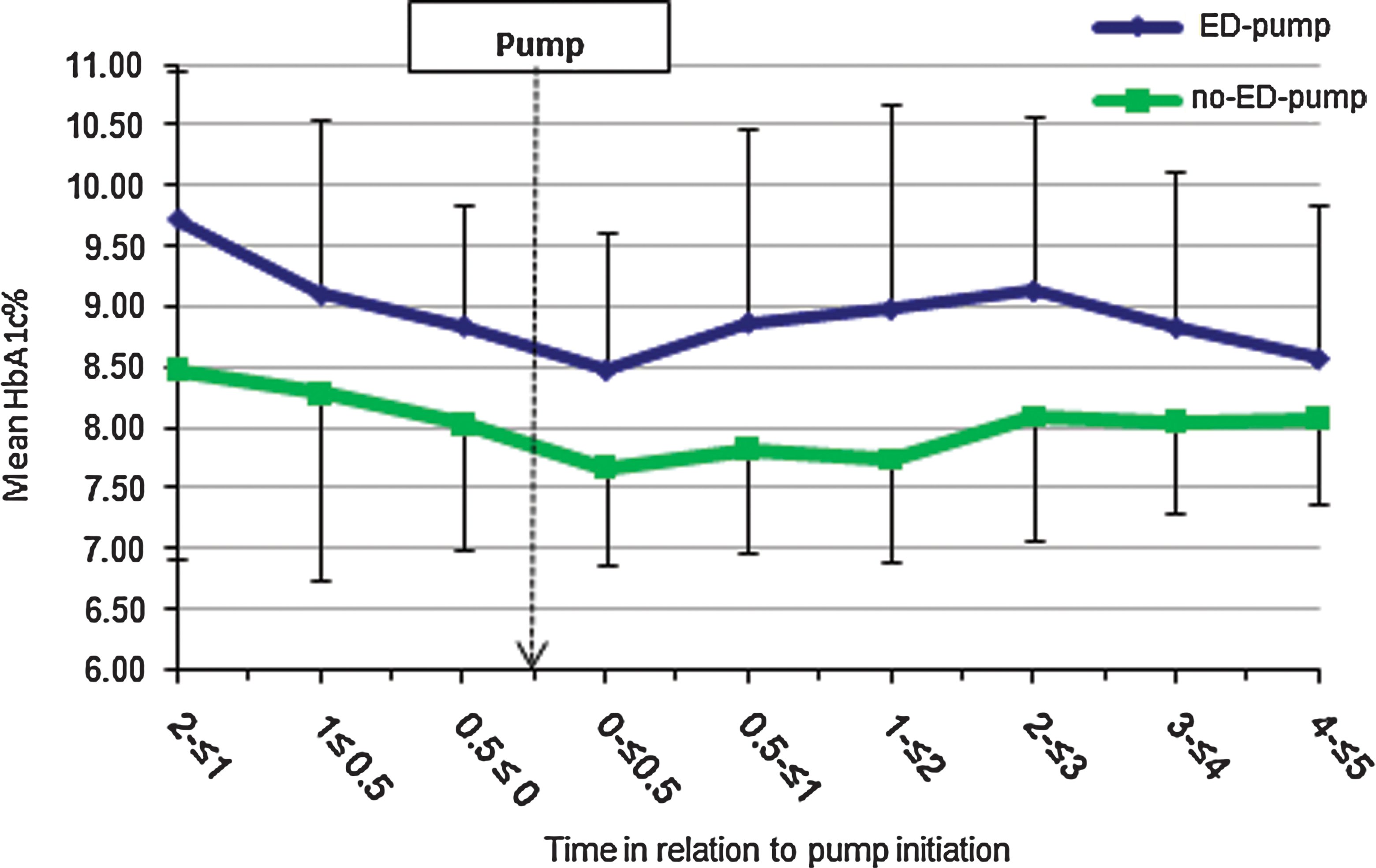
Mean hemoglobin A1c (HbA1c) levels for each time interval prior to and after pump treatment in the eating disorders-pump group (ED-pump group) and the no-ED-pump group. Color images available online at
For comparison between the patients with ED treated by insulin pump and patients with ED treated with MDI, we used the mean HbA1c values obtained during each of the following time intervals: 1 year prior to diagnosis of ED, 0 to ≤2 years, 2 to ≤4 years, and >4 years after diagnosis of ED.
Results
The clinical and demographic baseline characteristics of patients with ED (n = 8) or without ED (n = 48) treated by insulin pump are presented in Table 1. There was no statistical difference in disease duration and time to pump initiation between the two groups. Girls with ED were 3 years older at diagnosis of diabetes, and the duration of treatment with insulin pump was shorter compared with the no-ED group.
Data are mean ± SD values.
ED, eating disorders; T1DM, type 1 diabetes mellitus.
Mean ± SD HbA1c levels in patients with and without ED in relation to initiation of pump therapy are shown in Figure 1 from 2 years prior to pump start until 5 years after initiation of treatment. Girls with ED had higher mean HbA1c levels compared to the no-ED group (P = 0.007) both before and after treatment with insulin pump.
In the no-ED pump group, HbA1c levels during the 6-month period after pump initiation were significantly lower compared to the baseline reference value 6 months prior to pump initiation (7.67% vs. 8.03%, respectively; P = 0.004). Subsequently HbA1c levels were not different from baseline reference values. In the ED group, HbA1c levels were similar to baseline reference levels throughout the follow-up period. There was no change in trend of HbA1c levels with time, starting from 6 months prior to pump initiation, either in the no-ED group (P = 0.86) or in the ED group (P = 0.88).
During the mean of 4.7 years of pump treatment, four girls from the ED-pump group each had a single episode of severe hypoglycemia. In comparison, during a mean of 2.5 years 10 girls from the no-ED group had a total of 14 episodes of severe hypoglycemia. The rate of hypoglycemic episodes was thus similar, 0.9 compared to 1.0 episodes per 100 patient-years, in the two groups, respectively. Despite the improvement in HbA1c, girls in the ED-pump group had more episodes of DKA compared with the no-ED group (16 vs. 1.7 episodes per 100 patient-years, respectively).
We further compared HbA1c levels in patients with ED treated by insulin pump with ED patients treated with MDI. The clinical and demographic characteristics of patients with the ED-pump (n = 8) and ED-MDI (n = 7) groups are presented in Table 2. There was no difference in age at diagnosis of T1DM, their current age, duration of diabetes, age of diagnosis of ED, and time between diagnosis of diabetes and diagnosis of ED between the two groups. Prior to diagnosis of ED, the mean HbA1c levels in the ED-pump group and the ED-MDI group were similar (9.24 ± 1.25% vs. 8.47 ± 1.30%; P = 0.51). In the time intervals after the diagnosis of ED, mean HbA1c level of girls in the ED-pump group was lower than that of the ED-MDI group (Fig. 2). After the diagnosis of ED the mean HbA1c of all the measurements in patients treated by insulin pump was significantly lower compared with patients treated with MDI (9.07 ± 1.33% vs. 10.40 ± 2.01%; P = 0.04).
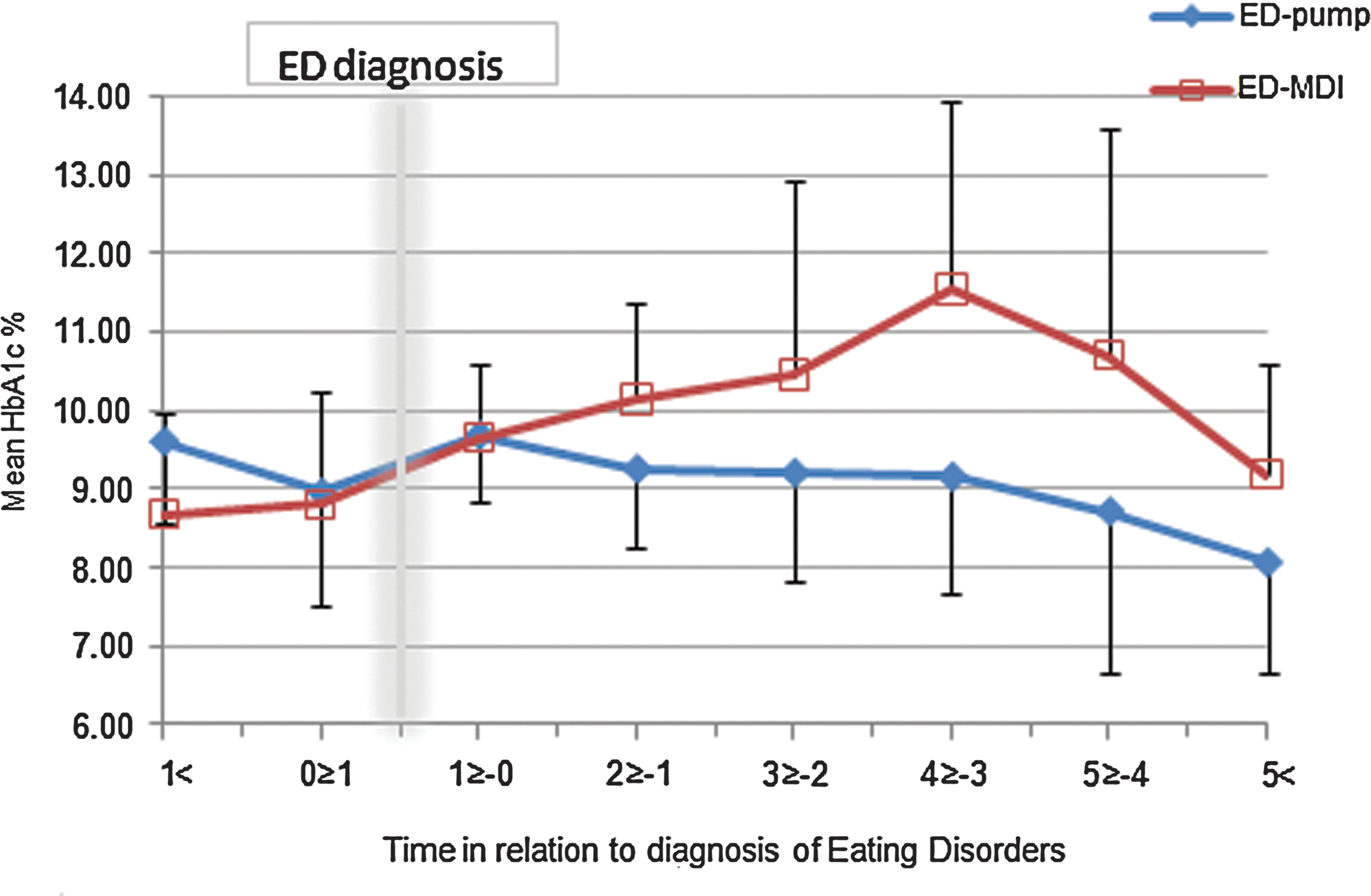
Mean hemoglobin A1c (HbA1c) levels for each time interval prior to and after diagnosis of eating disorders in the eating disorder-pump group (ED-pump group) and eating disorders-multiple daily injections group (ED-MDI group). Color images available online at
ED, eating disorders; MDI, multiple daily injections; T1DM, type 1 diabetes mellitus.
Following the diagnosis of ED, five of the eight girls with ED treated with insulin pump had a total of seven episodes of DKA, compared to five of the seven girls with 10 episodes of DKA in the MDI group (24 vs. 29 events per 100 patient-years, respectively). Four of the eight girls with ED treated by insulin pump had a total of eight episodes of severe hypoglycemia compared to only one episode in the MDI group.
Discussion
Our data show that insulin pump treatment in girls with T1DM and ED is feasible and is not associated with impaired metabolic control. Females with T1DM are especially vulnerable to develop disordered eating because of several factors. First, insulin treatment and improved metabolic control are associated with weight gain. 14 Second, dietary restraint may induce desire for certain foods, 15 and, finally, recurrent low blood sugar levels may promote uncontrolled eating. 16 Eating disturbances in females with T1DM tend to increase in frequency during adolescence and to persist thereafter. 17 Girls with diabetes and ED generally present with less well-recognized features of the eating disturbance and have less florid symptoms. 17 They are more likely to be of normal weight or overweight, rather than underweight, and thus confirmation of the diagnosis is often delayed.
ED in T1DM generally results in poor metabolic control and subsequent complications, and therefore any treatment modality aimed to improve metabolic control should be strictly enforced. Among patients with long-standing poor glycemic control insulin pump treatment resulted in a 0.84% reduction in HbA1c compared with intensive insulin injection treatment. 18 Similarly, in a case series study it was demonstrated that pump treatment can be used safely in young patients with poorly controlled diabetes to diminish DKA, reduce number of hospitalizations, and reduce healthcare costs. 19 Moreover, patients treated by insulin pump despite classic contraindications for pump treatment had significant falls in HbA1c levels. 20
In our study, longitudinal follow-up of HbA1c levels of adolescent females with T1DM and ED treated by insulin pump showed that their mean HbA1c level decreased prior to pump initiation and that the decrease persisted for approximately 6 months. Thereafter a gradual increase in HbA1c levels occurred. The response to pump treatment was similar to that seen in patients in the no-ED-pump group. Our results are consistent with other studies where improvement lasted only for a short time. 21,22
It is important to emphasize that the occurrence of episodes of severe hypoglycemia was similar in girls in the ED-pump group compared to girls in the no-ED-pump group. However, girls in the ED-pump group had more episodes of DKA compared with the no-ED-pump group, probably reflecting the poorer glycemic control as well as the impact of the underlying behavioral disorder. 5
Mean HbA1c levels of adolescents with ED treated by insulin pump were lower compared to adolescents with ED treated with MDI. In our study subjects with ED treated by insulin pump had slightly fewer events of DKA and more events of severe hypoglycemia, probably reflecting the improvement in glucose levels. Although these numbers are small, our results suggest that the introduction of pump therapy had no adverse effect on metabolic control in these complex cases.
Several limitations of our study deserve consideration. First, this is a retrospective observational chart review study, and the treatment of the patients with ED has not been randomized. Patients who opted for pump therapy may have been ready to attempt to improve their metabolic control and thus may not be comparable in many respects to the MDI-ED group. Furthermore, the time of diagnosis of ED is not always clearly defined, and symptoms and signs might have been mild or not noted prior to our purported age of diagnosis. In addition, we did not assess several other potential confounders, such as depression and family issues, that may influence treatment decisions, compliance, and outcome. However, we are unaware of any reports on pump therapy in girls with ED and believe that our observations suggest that this treatment can be undertaken in these complex patients. Our study can be regarded as a pilot design that calls for the initiation of prospective longitudinal studies with a larger sample of patients.
Early and intensive treatment of ED in young women with T1DM is important to prevent long-term morbidity and mortality. The insulin pump is an important tool for treatment; however, it apparently is not enough. Group therapy and psychological education, incorporating a nondeprivational approach to eating, may prove effective. In patients with longstanding T1DM there is a need for continued diabetes education and for close follow-up. 23 Recently it has been shown that a diabetes personal trainer intervention program resulted in significant effects on HbA1c among adolescents, 24 and additional modes of treatment should be incorporated in the treatment of adolescents with T1DM and ED.
In conclusion, the implications of this study are that treatment by insulin pump in girls with T1DM and ED is feasible and was effective in lowering mean HbA1c levels, albeit for a short time, and maintaining more stable levels thereafter. This observational study justifies further assessment of pump treatment in order to determine the optimal management program for this complex group of children.
Footnotes
Acknowledgments
The authors are in debt to Mrs. Avital Tene for her secretarial assistance.
Author Disclosure Statement
No competing financial interests exist.