
Abstract
Background:
This study assessed the relationship between and risk factors for microvascular complications of diabetes in an urban South Indian type 2 diabetes population.
Methods:
Subjects with diabetes (n = 1,736) were selected from the population-based Chennai Urban Rural Epidemiology Study (CURES) Eye Study conducted on a representative population of Chennai city in south India. Four-field stereo retinal color photography was done, and diabetic retinopathy (DR) was classified according to the Early Treatment DR Study grading system. Neuropathy was diagnosed if the vibratory perception threshold of the big toe using biothesiometry was ≥ 20V. Overt nephropathy was diagnosed if the subjects had persistent macroalbuminuria (urinary albumin excretion ≥ 300 μg/mg of creatinine) and microalbuminuria if it was between 30 and 299 μg/mg of creatinine. Among the 1,715 subjects with gradable fundus photographs, 1,608 individuals who had information on all test parameters were included.
Results:
Overall, DR was present in 282 (17.5%), neuropathy in 414 (25.7%), overt nephropathy in 82 (5.1%), and microalbuminuria in 426 (26.5%) subjects. Eighteen subjects had all three microvascular complications of diabetes. The risk of nephropathy (odds ratio [OR] = 5.3, P < 0.0001) and neuropathy (OR = 2.9, P < 0.0001) was significantly higher among the subjects with sight-threatening DR compared to those without DR. Common risk factors identified for all the three microvascular complications of diabetes were age, glycated hemoglobin, duration of diabetes, and serum triglycerides. DR was associated with nephropathy after adjusting for age, gender, hemoglobin A1c, systolic blood pressure, serum triglycerides, and duration of diabetes (OR = 2.140, 95% confidence interval = 1.261–3.632, P = 0.005).
Conclusions:
This is the first population-based study from India to report on all microvascular complications of diabetes and reveals that the association between DR and nephropathy is stronger than that with neuropathy.
Introduction
Subjects and Methods
Study subjects were recruited from the Chennai Urban Rural Epidemiology Study (CURES), conducted on a representative population of Chennai (formerly Madras) in southern India using the systematic random sampling technique. The details of the sampling and methods of the study have been published elsewhere. 10,11
In brief, in Phase 1, a detailed questionnaire was used to obtain basic demographic data for 26,001 randomly selected individuals ≥ 20 years old from Chennai residents, and fasting capillary blood glucose was measured using a OneTouch® Basic glucose meter (LifeScan, a Johnson & Johnson Company, Milpitas, CA) with self-reported diabetes identified in Phase 1 (n = 1,529), classified as “known diabetes” (KD) subjects.
In Phase 2 of CURES, all the KD subjects (n = 1,529) were invited to our Centre for detailed studies on vascular complications. Of these, 1,274 subjects consented for retinal examination, estimation of microalbuminuria, and biothesiometry studies (response rate, 83.3%). In addition, a 15% random sample each of the newly detected diabetes (NDD) subjects, those with impaired fasting glucose, and a 10% random sample of normal individuals from Phase 1 were subjected to an oral glucose tolerance test using a 75-g oral glucose load (dissolved in 250 mL of water) (n = 2,870). All those identified as having diabetes from any of these groups were treated as NDD subjects and included in the study. Thirty-seven of the individuals with impaired fasting glucose, 14 of the normal subjects, and 320 of the NDD subjects from Phase 1 were confirmed as NDD based on the World Health Organization criteria (2-h plasma glucose ≥ 200 mg/dL [ ≥ 11.1 mmol/dL]). 12 Of the total of 371 NDD subjects, 334 consented to participate in the study (90.0%). Institutional ethics committee approval was obtained for the study, and informed consent was obtained from all study subjects.
Measurements of weight, height, and waist circumference were obtained using standardized techniques. 10 The body mass index was calculated using the formula: weight (in kg)/height (in m) squared. Blood pressure was recorded in the sitting position in the right arm with a mercury sphygmomanometer (Diamond Deluxe Industrial Electronics and Products, Pune, India) and rounded off to the nearest 2 mm Hg. Two readings were taken 5 min apart, and the mean of the two was taken as the final blood pressure reading. Hypertension was diagnosed in subjects who were taking antihypertensive medication or had systolic blood pressure (SBP) ≥ 140 mm Hg or diastolic blood pressure ≥ 90 mm Hg. 13
A fasting blood sample was taken for estimation of plasma glucose and serum lipids after an overnight fast of 8 h using a Hitachi 912 autoanalyzer (Roche Diagnostics GmbH, Mannheim, Germany). Glycated hemoglobin (HbA1c) was measured by the high-performance liquid chromatography method using the Variant® machine (Bio-Rad, Hercules, CA).
Urine samples were collected after an overnight fast. Microalbumin concentration was measured using an immunoturbidometric assay (Hitachi 902 autoanalyzer, Roche Diagnostics). Microalbuminuria was diagnosed if the albumin excretion was between 30 and 299 μg/mg of creatinine. 14 The diagnostic criterion for macroalbuminuria or overt nephropathy was albumin excretion ≥ 300 μg/mg of creatinine.
The ocular fundi were photographed using four-field stereo color retinal photography (Zeiss FF 450 plus camera, Carl Zeiss, Oberkochen, Germany) by trained and certified photographers. Photographs were graded by an ophthalmologist using the Early Treatment DR Study (ETDRS) grading system. 15 The minimum criterion for diagnosis of DR was the presence of at least one definite microaneurysm in any field photographed. Photographs were assessed and assigned a retinopathy level, and the final diagnosis for each patient was determined from the grading of the worse eye according to the ETDRS criteria for severity of disease in the individual eye. In brief, according to the ETDRS grading, level 10 represents no retinopathy, level ≥ 20 indicates nonproliferative DR (NPDR), and level ≥ 60 signifies proliferative DR (PDR). 15 Diabetic macular edema (DME) was defined as retinal thickening at or within 1 disc diameter of the center of the macula or the presence of definite hard exudates. Sight-threatening DR (STDR) or severe DR was defined as the presence of NPDR with DME and PDR.
A biothesiometer (Biomedical Instrument Co., Newbury, OH) was used to assess the vibratory perception threshold of the big toes in a standardized fashion. Neuropathy was diagnosed if the vibratory perception threshold of the big toe exceeded the mean + 2SD of the healthy study population without diabetes 20–45 years old (cutoff ≥ 20 V). 9
Statistical analysis
Statistical analysis was done using SAS statistical package version 9.0 (SAS Institute Inc., Cary, NC). Data are expressed as mean ± SD values. Trend χ 2 test was used to compare proportions among groups. The associations of DR with either neuropathy or nephropathy were analyzed using multiple logistic regression analysis with DR as the dependent variable. Different models were constructed to determine the associations by adjusting for common risk variables. Collinearity between nephropathy and neuropathy was assessed by conducting linear regression analysis to obtain the relevant tolerance value and its reciprocal variance inflation factor. Receiver operating characteristics (ROC) curves, which are plots of the sensitivity versus (1 – specificity) was constructed to determine the cutoffs of microalbuminuria measures with optimum sensitivity and specificity for predicting STDR. The area under the ROC curve, which indicates the strength of the association between the test variable and the outcome measure, was obtained, and the 95% confidence intervals (CI) were also calculated. A value of P < 0.05 was considered significant.
Results
This study included 1,608 subjects with type 2 diabetes, of which 1,274 were KD subjects and 334 were NDD subjects, who had gradable retinal photographs, albuminuria estimations, and biothesiometry studies done in Phase 2 of CURES.
Figure 1 depicts a Venn diagram showing the overlap of microvascular complications of diabetes (retinopathy, overt nephropathy, and neuropathy) in the study population. Among the 1,608 subjects with diabetes studied, DR was present in 282 (17.5%), overt nephropathy in 82 (5.1%), and neuropathy in 414 (25.7%) subjects. Microalbuminuria was present in 426 (26.5%) of the study population. From Figure 1 it can be observed that only 18 subjects (1.1%) had all three microvascular complications of diabetes, while 81 subjects (5.0%) had both DR and neuropathy, 14 subjects (0.9%) had DR and overt nephropathy, and finally 11 subjects (0.7%) had overt nephropathy and neuropathy. Among the individuals with DR, 35.1% had neuropathy, and 11.3% also had overt nephropathy. Retinopathy and overt nephropathy were present in 23.9% and 7% of the subjects with neuropathy, respectively, while among those subjects who had overt nephropathy, 35.4% had neuropathy, and 39% had retinopathy. The prevalence of DR without any other complication was 10.5% (169 of 1,608); 5.9% (95 of 1,608) had one additional complication, and 1.1% (18 of 1,608) had two.
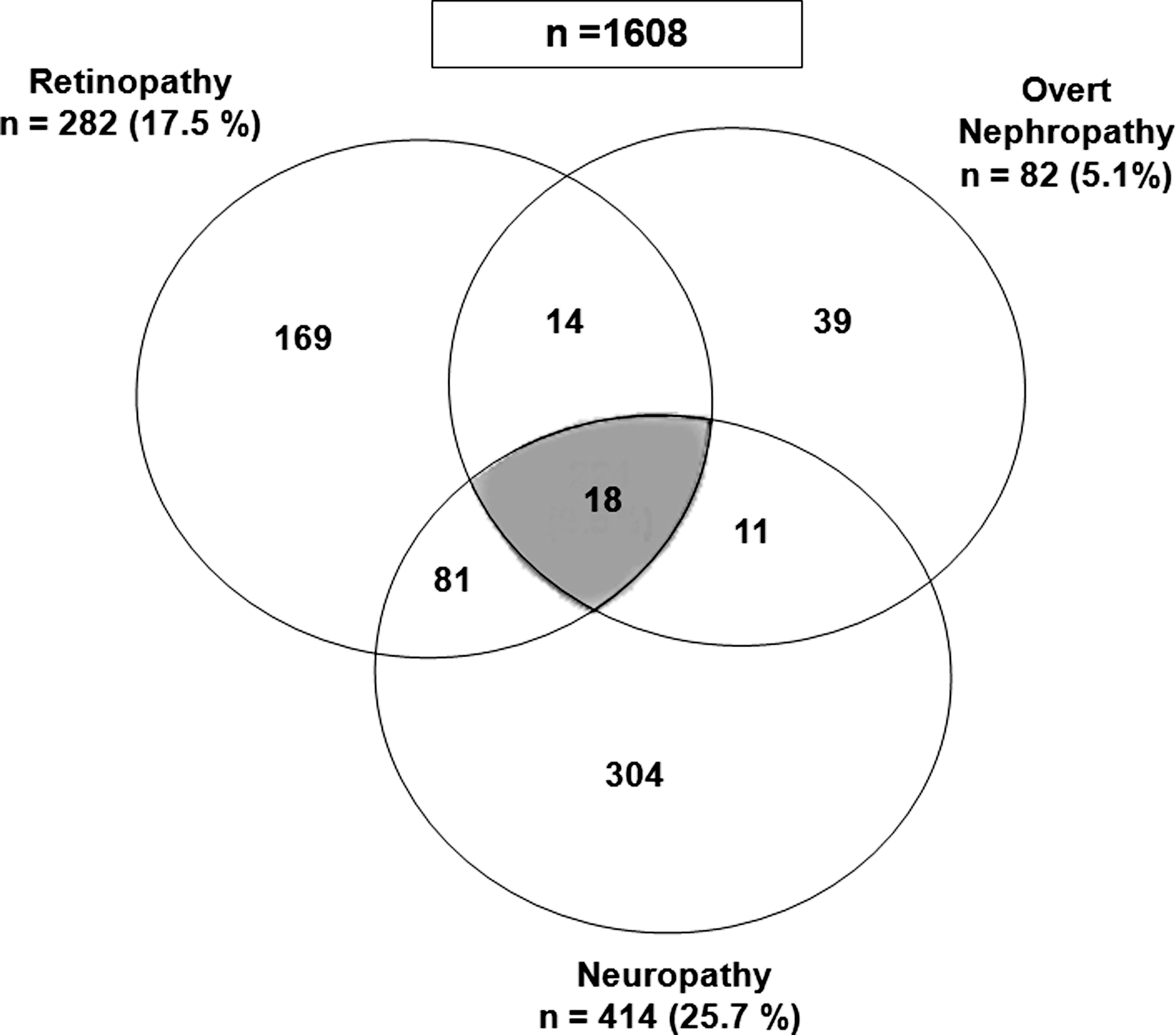
Venn diagram showing the overlap of microvascular complications of diabetes in the study population.
Prevalence of overt nephropathy and neuropathy in subjects with and without DR according to status of diabetes is presented in Table 1. Compared to the NDD subjects, KD subjects had higher prevalence rates of both overt nephropathy and neuropathy (5.6% vs. 3.3% [P = 0.092] and 27.4% vs. 19.5% [P = 0.003], respectively). When subjects with overt nephropathy and neuropathy were categorized based on the status of retinopathy, subjects with KD had a significantly higher prevalence rate of neuropathy with retinopathy compared to NDD subjects (P = 0.007). Although subjects with KD had a higher prevalence rate of overt nephropathy, this did not reach statistical significance compared to NDD subjects.
P values for comparison of newly diagnosed diabetes (NDD) versus known diabetes (KD): overall neuropathy, P = 0.003; neuropathy with retinopathy, P = 0.007.
The prevalence of neuropathy and macroalbuminuria (overt nephropathy) was studied with severity of DR. An increase in the prevalence of neuropathy (no DR, 23.8%; NPDR without DME, 28.4%; STDR, 47.5% [P for trend < 0.0001]) and macroalbuminuria (no DR, 3.8%; NPDR without DME, 8.2%; STDR, 17.2% [P for trend < 0.0001]) with increasing severity of DR was observed in this study.
The risk for neuropathy and overt nephropathy when computed in relation to severity of DR is shown in Figure 2. Regression analysis revealed that risk for neuropathy among subjects with STDR was 2.9 (95% CI = 1.92–4.39, P < 0.0001) compared to those without DR as the reference. In addition, the risk for overt nephropathy increased with severity of DR (NPDR without DME, odds ratio [OR] = 2.3, 95% CI = 1.25–4.14, P = 0.007; STDR, OR = 5.3, 95% CI = 2.92–9.58, P < 0.0001) compared to those without DR as the reference.
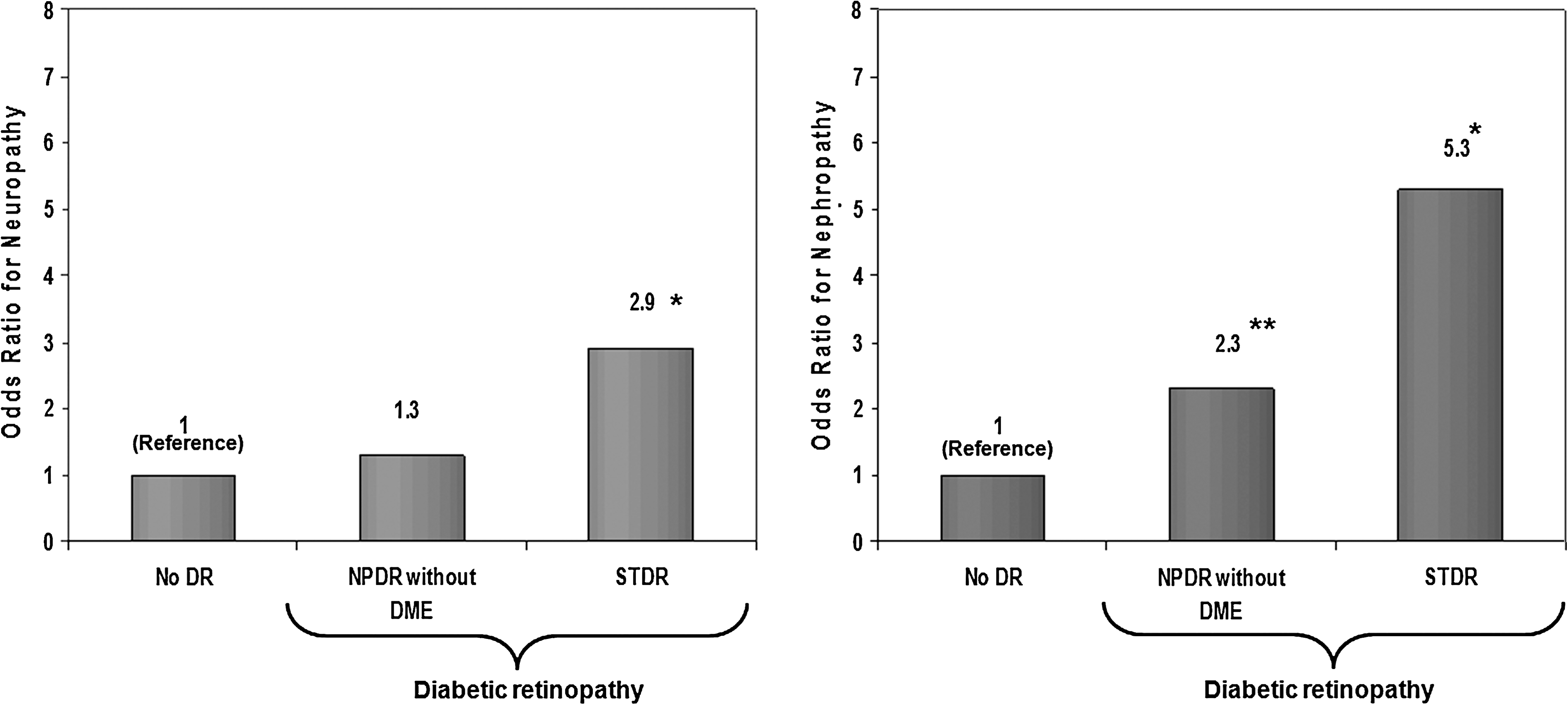
Risk for
Table 2 presents the results of univariate analysis of microvascular complications of diabetes with various risk factors. On regression analysis, the following common risk factors were identified for the three microvascular complications of diabetes: age, HbA1c, duration of diabetes, and serum triglyceride levels. In addition, it was observed that one microvascular complication was associated with the other two microvascular complications in the univariate analysis. However, hypertension was not associated with retinopathy, and cholesterol was not significantly associated with neuropathy in this study.
HbA1c, glycated hemoglobin.
Table 3 shows the results of regression analysis using DR as the dependent variable. DR was significantly associated with overt nephropathy in the unadjusted model (OR = 3.266, 95% CI = 2.054–5.194, P < 0.0001). On introducing age and gender into the model the association of DR with overt nephropathy persisted (P < 0.0001). Even after adjusting for age, gender, HbA1c, SBP, serum triglyceride, and duration of diabetes, DR was associated with overt nephropathy (OR = 2.140, 95% CI = 1.261–3.632, P = 0.005). In addition, DR was significantly associated with neuropathy in the unadjusted model (OR = 1.736, 95% CI = 1.318–2.287, P < 0.0001) and after adjustment for age, gender, HbA1c, SBP, and serum triglyceride (OR = 1.394, 95% CI = 0.995–1.953, P = 0.054). However, when duration of diabetes was introduced into the model, the significance was attenuated (P = 0.128).
Model 1 was adjusted for age and gender, Model 2 was adjusted for Model 1 plus hemoglobin A1c, systolic blood pressure, and serum triglycerides, and Model 3 was adjusted for Model 2 plus duration of diabetes.
When assessed for collinearity between nephropathy and neuropathy, there was no significant collinearity detected (β coefficient = 0.123, P = 0.07, tolerance = 1.0, variance inflation factor = 1.0).
Analysis revealed that among subjects with STDR, 10.1% of the subjects had microalbuminuria, and 20.7% had macroalbuminuria (P = 0.006). Based on this, an ROC analysis was done to determine the optimal cutoff point of albuminuria for the prediction of STDR with the highest sensitivity and specificity. In Figure 3, the area under the ROC curve was 0.675 (95% CI = 0.615–0.735, P < 0.0001), and a cutoff of an albumin excretion of 34.5 μg/mg of creatinine was the optimum cutoff value for prediction of STDR. The corresponding sensitivity was 60.2%, and specificity was 75.6%.
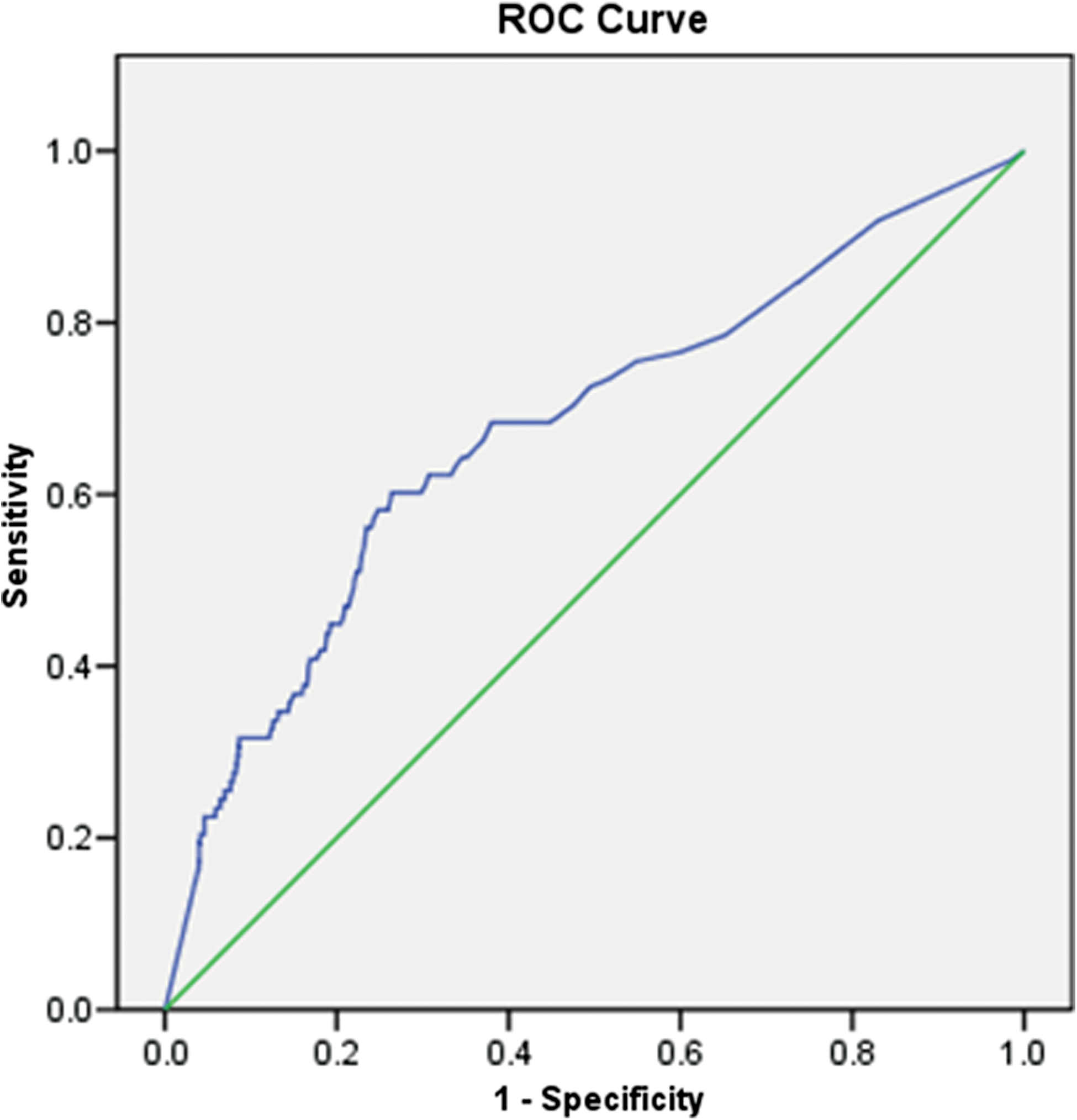
Receiver operator characteristic curve of urinary albumin excretion for prediction of severe diabetic retinopathy gives a cutoff point of ≥ 34.5 μg/mg of creatinine with sensitivity of 60.2% and specificity of 75.6%. Area under the curve = 0.675 (95% confidence interval = 0.615–0.735); SE = 0.031; P < 0.0001. Color images available online at
Discussion
People of South Asian descent living in the Indian subcontinent, West Indies, South East Asia, Africa, and the United Kingdom have some of the highest diabetes prevalence rates in the world. 16 Studies have reported that South Asians with diabetes have a higher prevalence of established microvascular disease, which contributes to serious morbidity and mortality 17 compared to Europeans, as demonstrated by follow-up 18 of the Southall diabetes survey, a population-based study conducted among South Asians and Europeans in 1984. Recently, Potluri et al. 19 have reported that the prevalence of microvascular complications such as retinopathy (India, 16.3%; Mauritius, 2.3%; United Kingdom, 2.6%), nephropathy (India, 20.5%; Mauritius, 10.5%; United Kingdom, 2.3%), and neuropathy (India, 8.4%; Mauritius, 1.2%; United Kingdom, 5.1%) complications to be significantly higher in India compared to Mauritius and the United Kingdom.
It has been demonstrated that along with the presence of external risk factors, some associations have also been noted between microvascular complications of diabetes themselves. 3 –5,17,20,21 In addition, studies have shown that the presence of DR itself may reveal patients at risk of diabetic nephropathy 4,22,23 and neuropathy. 6,24 –26
This is the first population-based study from India to look at the prevalence and overlap of the various microvascular complications of diabetes. This study demonstrates an association among all the three microvascular complications in a representative sample of individuals with type 2 diabetes. Morgan et al. 27 found evidence to show that although not all people with diabetes developed complications, multiple complications occur in almost one-fifth of individuals. In this study, 18 subjects (1.1%) had all three microvascular complications of diabetes, and, in addition, among the individuals with DR, over 35% had neuropathy, and nearly 11% also had overt nephropathy.
This study demonstrates that the common risk factors identified for the three microvascular complications are age, HbA1c, duration of diabetes, and triglycerides. Hypertension was not associated with DR; however, this conclusion should be interpreted with caution as this is a cross-sectional study. The United Kingdom Prospective Diabetes Study results have established that retinopathy, nephropathy, and possibly neuropathy are benefited by lowering blood glucose levels in type 2 diabetes with intensive therapy, which achieved a median HbA1c of 7.0% compared with conventional therapy with a median HbA1c of 7.9%. The United Kingdom Prospective Diabetes Study has shown that the overall microvascular complication rate decreased by 25%. 28 Recently, in the Fenofibrate Intervention in Event Lowering in Diabetes study, fenofibrate treatment demonstrated a significant 30% reduction in the need for laser therapy in patients with and without known DR, and more particularly in the first course of laser treatment for both DME and PDR; in addition, fenofibrate treatment was associated with less albuminuria progression and reduced risk of nontraumatic distal amputations from the use of a lipid-lowering agent in type 2 diabetes mellitus. 29 These data underline the importance of glycemic, blood pressure, and lipid control in type 2 diabetes in order to prevent microvascular complications.
The severity of DR also appears to have an effect on the prevalence of diabetic neuropathy and overt nephropathy. In this study it was observed that the prevalence of neuropathy and overt nephropathy increased significantly with increasing severity of retinopathy. This observation is consistent with a cross-sectional study done by El-Asrar et al. 4 in 2001, conducted in patients with type 2 diabetes to determine the predictive value of DR. They reported the prevalence of diabetic nephropathy to rise with increasing severity of DR, and the prevalence rate of diabetic neuropathy was significantly higher among patients with DME than among those without DR. 4
An association between the presence of DR and risk of developing an abnormally high urinary albumin excretion rate among subjects with diabetes has been reported. 30,31 The association between DR and macroalbuminuria could be explained by the fact that elevated urinary albumin excretion is a marker of generalized disease in the vascular wall of small blood vessels. Alternatively, macroalbuminuria and DR may share common determinants. It has also been shown that the prevalence of nephropathy also increases in relation to the severity of DR in a study conducted in 210 and 438 patients with, respectively, type 1 and type 2 diabetes. 4 This is consistent with the findings of this study, where the prevalence of macroalbuminuria also increased in relation to the severity of DR.
Long-term prospective observational studies have documented that DR is one of the most important risk factors responsible for the development of kidney disease due to diabetes in both type 1 and type 2 diabetes. 22,32,33 Further support of the close relationship between renal and retinal complications comes from other studies 34,35 that have reported that DR may independently predict the development of microalbuminuria and hence be a powerful predictor of the progression of renal damage in diabetes patients. A study done in type 2 diabetes by Savage et al. 21 provided evidence that overt nephropathy, but not microalbuminuria, was independently related with the presence of retinopathy and nephropathy. In our study, logistic regression analyses revealed a similar association: when compared with those without retinopathy, individuals with NPDR and no DME were two times likely to have overt nephropathy, and subjects with STDR were five times more likely to develop overt nephropathy.
A prospective, observational study of a cohort of white, type 2 diabetes patients followed for a median period of 5.8 years showed that presence of DR was one of the major determinants of progression to incipient or overt diabetic nephropathy. 36 This study also reports an association between DR and overt nephropathy in subjects with type 2 diabetes; this association was present even after adjusting for age, gender, HbA1c, SBP, serum triglycerides, and duration of diabetes. This is consistent with the study done by El-Asrar et al., 4 which showed an association between retinopathy and nephropathy in subjects with diabetes. However, Kanauchi et al. 36 reported lack of association between retinopathy and nephropathy in Japanese type 2 diabetes patients.
Lunetta et al. 37 reported that increased urinary albumin excretion is a marker of risk for retinopathy in patients with type 2 diabetes mellitus. This is consistent with the present study, in which, based on the sensitivity, specificity, and ROC calculations, the data suggest that an albumin excretion level of 34.5 μg/mg of creatinine, with sensitivity of 60.2% and specificity of 75.6%, may independently predict the development of STDR. Nevertheless, more studies are needed to clarify this association.
The results of our logistic regression analysis revealed that individuals with STDR were nearly three times more likely to have neuropathy compared with those without retinopathy. These results extend upon the findings of other studies that have found a relationship between retinopathy and neuropathy in people with diabetes. 24 –26,38 El-Asrar et al. 4 also reported that patients with mild to moderate NPDR or PDR, besides from being a predictor of diabetic nephropathy, are at an increased risk of having diabetic neuropathy as indicated in the present study. Jennings et al. 3 also showed an association between retinopathy and severity of neuropathy.
In our multiple logistic regression analysis DR was associated with neuropathy even after adjusting for age, gender, HbA1c, SBP, and serum triglycerides. However, when duration of diabetes was introduced into the model, the association between DR and neuropathy was lost. This could be attributed to the fact that microangiopathy is dependent on the duration of diabetes. 39,40 However, in a cross-sectional study done in Saudi Arabian subjects with type 1 and type 2 diabetes, 4 multivariate logistic regression analyses did not reveal an association that was statistically significant between retinopathy and neuropathy. This study also shows that the three microvascular complications are interrelated, with one being a risk factor for another as suggested by Girach et al. 2 and Sicree et al. 16
The strengths of this study are that it is the first population-based study to report on the prevalence and association of all microvascular complications of diabetes from India. The limitation of the study is that because it is a cross-sectional study, no inferences on cause and effect between risk factors and the presence of microvascular complications can be drawn. Prospective studies are required to examine the temporal relationships between risk factors and further understanding of the relationship of the pathophysiological events responsible for these microvascular complications.
In conclusion, in this cross-sectional population-based study of type 2 diabetes in south India, it is observed that the prevalence of, and risk for, neuropathy and overt nephropathy increased significantly with increasing severity of retinopathy. An association between DR and overt nephropathy is also observed. This association appears to be independent of age, gender, HbA1c, SBP, serum triglycerides, and duration of diabetes. However, an association is not observed for neuropathy and DR as the significance is lost when duration was introduced into the model. Any conclusions regarding these associations must be made with caution as this is a cross-sectional study. The data suggest that the presence of one microvascular complication increases the risk of having another. Overall, the association between DR and diabetic nephropathy seems to be much stronger, compared with the association between DR and diabetic peripheral neuropathy. Thus prevalence of one complication in an individual with diabetes should alert the healthcare provider to screen for other microvascular complications in order to further reduce morbidity and mortality due to these complications.
Footnotes
Acknowledgments
We acknowledge gratefully the help of the epidemiology team for the fieldwork, the eye technicians for performing preliminary eye testing and retinal photography, the technicians for performing biothesiometry, and most importantly the subjects who participated in the study. The CURES field studies were supported by the Chennai Willingdon Corporate Foundation, and this is the fifth study from the CURES Eye Study and the 92nd study from CURES.
Author Disclosure Statement
No competing financial interests exist.