
Abstract
Background:
No recent clinical data on the incidence of catheter-related adverse events under insulin pump therapy have been reported.
Methods:
This was a prospective, two-period, observational, multicenter study in 45 diabetes outpatients (mean continuous subcutaneous insulin infusion [CSII] use, 6 years; mean hemoglobin A1c, 7.7%, at baseline). During the initial 1-month period (P1), the patients used their current catheter model, including a soft cannula in 98% of cases. They moved then to the new Accu-Chek® FlexLink catheter model (Disetronic Medical Systems AG, Burgdorf, Switzerland) for a 3-month period. The primary end point, including insertion failures and unexplained hyperglycemia within the first 6 h after catheter placement, was assessed from logbook records during P1 and the last month of the second period (P2). Secondary end points were catheter replacements for unexplained hyperglycemia and/or events at risk for immediate insulin delivery failure after the first 6 h.
Results:
Forty-five initial infusion failures occurred in 14 patients among 507 catheter insertions (8.9% of cases) during P1, whereas 15 similar events were seen in nine patients during P2 among 488 catheter insertions (3.1% of cases) (P < 0.001). Catheters were replaced for later infusion troubles in 8% of cases during both P1 and P2. The overall rate of late cumulative events was, however, 113 of 507 (P1) versus 66 of 488 (P2) (P < 0.001). The occurrence of pain, skin reaction, or redness at the infusion site was lower during P2.
Conclusion:
Incidences both of initial failures and of premature catheter replacements were 8–9% with current CSII catheters. Significantly reduced failures after insertion and adverse events at the infusion site were observed with the new catheter model.
Introduction
However, the data on IS-related complications, including obstructions, infections, and DKA, reported in the 1980s are outdated. 5 Catheter-related problems were monitored during the recent 5-Nations Trial that reported the only updated complication rate at infusion sites. 6 In this study, no adverse event related to IS was classified as serious, suggesting that advances in CSII catheter technology and/or better experience, including increased patient vigilance (e.g., change of IS after two consecutive high blood glucose values), have lowered catheter issues in CSII use. Nevertheless, this study provided limited data and did not describe the common management of IS under conditions of daily life. While significant technological improvements of CSII catheters have emerged for the last decade, their specific clinical outcomes have not been investigated so far.
The objectives of the multicenter study reported here were to assess the current incidence of catheter-related problems in diabetes patients treated by CSII and to evaluate the effect of a newly designed catheter on these issues.
Subjects and Methods
Subjects
Fifty consecutive experienced diabetes outpatients, treated with an external insulin pump, were enrolled for the present prospective, observational study involving 13 CSII centers. The treatment was conducted according to the French regulatory rules for CSII. 7 Inclusion criteria were age ≥15 years, duration of CSII of >3 months, the ability to attend a visit 4 months after inclusion, and the accepted planning of IS move to the Accu-Chek® FlexLink model (Disetronic Medical Systems AG, Burgdorf, Switzerland) during the study duration. Exclusion criteria were hemoglobin A1c >10% before recruitment, any defect in pump management by the patient, impaired sight, motor or joint impairment of an upper limb that could possibly interfere in insertion of the IS, and a recent history (<6 months) of unexplained DKA or severe hypoglycemia.
Design and methods
During an initial 1-month period (P1) of this two-period study, the patients used their current IS. They moved then to the Accu-Chek FlexLink IS, and the second study period (P2) was defined as the first 3 months after P1. The study visits were scheduled in accordance with clinical practice (i.e., training for the use of a new catheter model and clinical follow-up of patients on CSII). The study included an inclusion visit (V0, in order to record patient characteristics) just before P1 and visits at the end of P1 (V1) and at the end of the second period (V2). In order to obtain relevant prospective data, investigators taught all patients that they had to fill in their CSII logbook every day, which was considered as the source document to assess study end points. All IS replacements and events during P1 and the last month of P2 had to be reported. When each catheter was inserted, pain was graded by patients using the Visual Analog Scale (VAS) (on a scale of 0–10, where 0 = no pain and 10 = great pain). The use of an insertion device was left at the patient's discretion during both study periods. The study was performed in agreement with the institutional ethical board policies.
Study criteria and statistical analysis
The first study end point was the incidence of catheter insertion failures and unexplained hyperglycemia (UHG) within the first 6 h (UHG<6h) after insertion and was assessed for comparison between P1 and P2. According to the current clinical guidelines, hyperglycemia was considered for blood glucose >250 mg/dL, 7 and UHG was defined as any hyperglycemia not related to a pump failure, an inappropriate diet, or an acute concomitant illness. The incidence of IS replacements for UHG or events at risk of insulin delivery failure (IDF) later than 6 h after insertion was the secondary end point.
Clinical and laboratory data are presented as mean (SD) or median (interquartile ranges), apart from incidence data. Comparative analyses were done on the data of patients having performed V2 using paired Wilcoxon's test and χ 2 test. Statistical analyses were performed with SAS version 8.2 (SAS Institute, Cary, NC), and P values < 0.05 were considered as statistically significant.
Results
Forty-five among the 50 enrolled diabetes patients completed the study. During P1, one patient discontinued CSII, and two were lost to follow-up according to the study criteria; during P2, one patient discontinued FlexLink, and one patient was lost to follow-up according to the study criteria. Only the data from study completers are presented here. The main characteristics of the patients who completed the study are shown in Table 1. Eighty-four percent of patients had type 1 diabetes. All patients were treated with a fast-acting insulin analog, and six models of insulin pump were used by the study patients. Among factors that could interfere with the study end points, two patients were treated with corticosteroids, and an immunosuppressive agent was taken as co-medication in one case; only 21% of patients reported intensive physical exercise less than once a week. Physical exercise four or more times per week was reported by 50% of patients for both study periods, and changes occurred for a few patients (two increased and two decreased physical activity during P2). The currently used IS at V0 was a steel catheter in one case and an IS with soft cannula in 44 of 45, including perpendicular (78%) or angled (20%) insertion. These IS devices were the Quick-set model (Medtronic MiniMed, Northridge, CA) in 68% of cases, Silhouette model (Medtronic-MiniMed), Sof-set model (Medtronic-MiniMed), and Cleo model (Smiths Medical, St. Paul, MN) in about 10% of cases for each model.
Data are mean ± SD or median (interquartile ranges) values.
According to specific catheters used. One of 36 did not use the insertion device at each insertion.
Accu-Chek LinkAssist. Two of 42 did not use the insertion device at each insertion.
CSII, continuous subcutaneous insulin infusion; P1, initial 1-month period (using their current catheter model); P2, last month of the 3-month period after the switch to the Accu-Chek FlexLink catheter model.
Insertion failures and UHG<6h
During the 1-month P1, 11 patients reported at least one catheter insertion failure, and six patients reported at least one UHG<6h, all requiring the immediate insertion of another IS. The proportion of patients who experienced either an insertion failure or UHG<6h (i.e., any event after insertion) was 14 out of 45 (31%). The overall incidence of these events connected to IS insertion was 45 among 507 inserted IS devices (8.9%). Most insertion failures and all UHG occurred in Quick-set model users; only one defect of adhesion, two blood backflows, and one obstruction occurred with the other catheter models.
During the last month of P2, six patients reported at least one catheter insertion failure, and four patients reported at least one UHG<6h, all requiring the immediate insertion of another IS. The proportion of patients who experienced any of these events after insertion was nine out of 45 (22%). The overall incidence of these events connected to IS insertion was 15 among 488 inserted IS devices (3.1%), which was significantly lower than that in P1 (P < 0.0001, χ 2 test).
The patients' reported details that were associated with the insertion failures during the two assessment periods are presented in Figure 1.
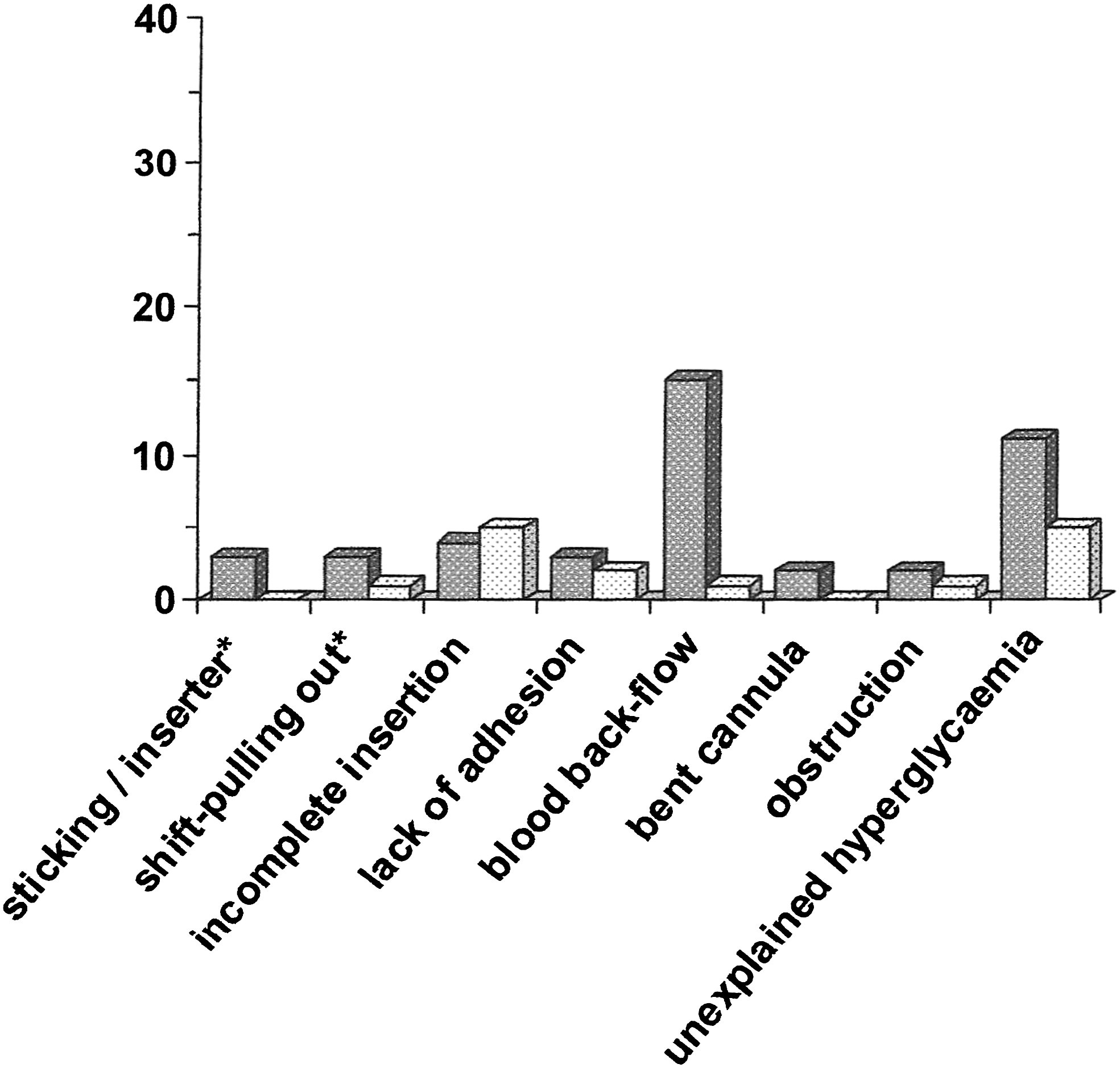
Insertion failures and unexplained hyperglycemia within the first 6 h after catheter insertions in 45 diabetes patients treated by CSII. The data presented correspond to the number of events during the initial 1-month period with their current catheter model (P1, dark histograms, among 507 catheter insertions) and during the last month of the second 3-month period after the switch to the Accu-Chek FlexLink catheter model (P2, light histograms, among 488 catheter insertions). *Events reported by patients using an inserter.
The percentage of IS devices associated with an insertion failure or UHG per patient decreased during the last month of P2 (P = 0.037 vs. P1, paired Wilcoxon's test). Of note is that the intensity of pain related to the catheter insertion was significantly reduced when using the FlexLink versus the usual catheter model: median VAS scores (interquartile ranges) were 2.10 (0.30–3.20) and 0.85 (0.10–1.80) out of 10, respectively (P < 0.02, paired Wilcoxon's test).
Events occurring and UHG>6h after catheter insertion
During P1, 15 patients reported at least one event at risk for immediate IDF, and nine patients had at least one UHG>6h after insertion. The proportion of patients who experienced any of these issues was 40%. The incidence of these issues was 39 among 507 IS devices (7.7%).
During the last month of P2, 11 patients reported at least one event at risk for IDF, and 11 patients had at least one UHG>6 h after insertion. The proportion of patients who experienced any of these issues was 42%. The incidence of these issues was 41 among 488 IS devices (8.4%).
The details of events that occurred at risk for IDF during the two assessment periods are presented in Figure 2A.
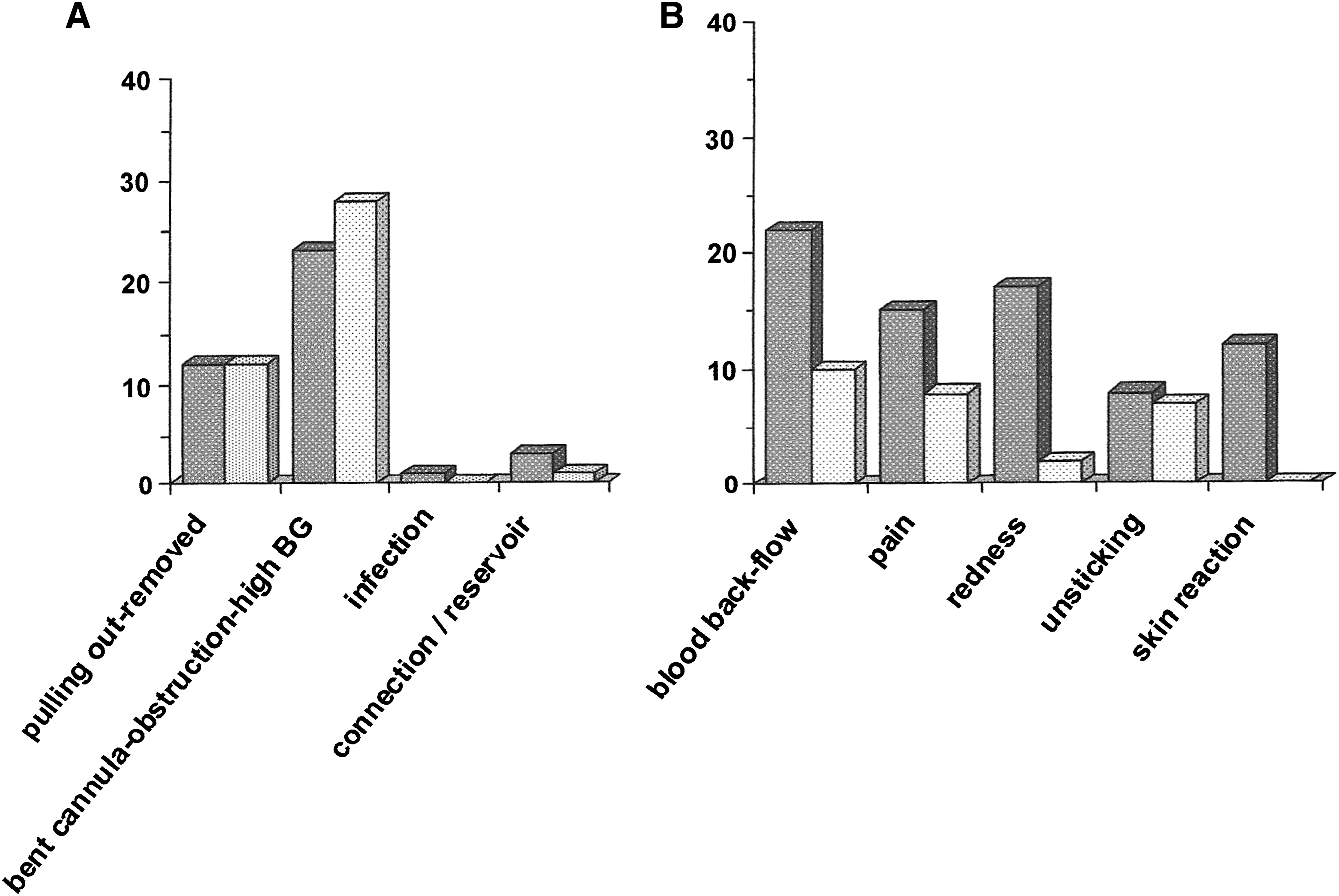
Events occurring later than 6 h after catheter insertion in 45 diabetes patients treated by CSII. The data presented correspond to the number of events during the initial 1-month period with their current catheter model (P1, dark histograms, among 507 catheters) and the last month of the second 3-month period after the switch to the Accu-Chek FlexLink catheter model (P2, light histograms, among 488 catheters). (
Apart from these events at risk for IDF that motivated systematic catheter change, 74 other catheter-related events were reported in P1 versus 27 in the last month of P2. Among those, only 25 in P1 and nine in P2 resulted in catheter change. The detailed list of these other events that prompted catheter change is shown in Figure 2B.
Hence, the overall rate of catheter-related events that occurred more than 6 h after insertion was significantly higher in P1 versus P2: 113 among 507 IS devices versus 68 among 488 IS devices, respectively (P < 0.001, χ 2 test). The lower occurrence of blood backflow, pain, skin reaction, and redness at the infusion site during P2 explained this difference. However, the median intensity of pain while wearing the IS (VAS score) was similarly low in P1 and P2 (0.60–0.80 out of 10 in both periods).
Discussion
This observational study documents the benefits associated with a new IS in 45 diabetes patients treated by CSII. Significant improvements were found on the primary study end point by a more than 50% reduction of insertion failures and hyperglycemic events in the immediate followings of catheter changes and on additional matters such as pain at insertion and overall later reactions at infusion site.
The first study period also provides updated information on the occurrence of catheter issues in the daily life conditions of diabetes patients treated by CSII. Overall, insertion failures of the commonly used models of infusion catheters were found in almost 9% of catheter changes, either documented by patient reports or suspected from UHG in the immediate interval following catheter insertion. Once the catheter was in place, anticipated replacement was motivated by conditions leading to insulin delivery failure or UHG in 8% of cases, while any of various reported troubles occurred with 22% of catheters. The metabolic outcomes of the catheter complications only included one episode of DKA (P1), two minor ketosis events, and four UHG episodes with borderline ketonemia (capillary blood β-hydroxybutyrate = 0.6–0.7 mmol/L). These data underscore the importance of a good adherence to self-monitoring of blood glucose with CSII in order to detect early infusion troubles. 8 Of note is that only one case of nonsevere infection at infusion site was reported during P1, which is also in agreement with an adequate management of CSII by the study patients. During the study periods, only a few patients exceeded the recommended rate of catheter change every 2–3 days, and no patient used more than 15 IS devices per month (data not shown). Seventy percent of patients reported no insertion failure with their current catheter use. Nevertheless, the report of various catheter issues in 40% of patients indicates that more severe outcomes could be encountered in less adherent patients. Hence, proper education to catheter use and safety measures of self-examination of infusion sites while on CSII appear as crucial factors to reduce deleterious adverse events of this mode of therapy. 3,7 Technological improvements of catheter technology do not change these recommendations because, in a recent study performed in healthy volunteers, soft Teflon cannulas have been associated with increased adipose tissue blood flow and bolus mean infusion pressure after a wear time of 48 h versus steel cannulas. 9
Interestingly, insertion failures and UHG after catheter change were reduced by 71% and 55%, respectively, when patients moved to the use of Accu-Chek FlexLink, including that of the Accu-Chek LinkAssist inserter in most cases. This improvement was unlikely biased by the recent education of the patients about the insertion of the new catheter because the handling of the insertion of their usual catheter had been examined when they were included in the study. Any significant handling error would have been identified and corrected at this time. The noticeable reduction of blood backflows after catheter insertion suggests that either the design of the cannula itself or the inserter mechanism could minimize the subcutaneous trauma associated with FlexLink insertion in comparison with other catheter and inserter models. The significantly reduced pain grading while using this new catheter model is in agreement with this hypothesis. The sustained tolerance at the infusion site further contributes to the overall reduced number of adverse events that were reported during insulin infusion via the FlexLink. However, the need for premature catheter changes due to patient-estimated risk of insulin delivery failure remained unchanged versus other catheter models. Whether these events motivating catheter changes were due rather to the patient's lifestyle mode than to the catheter itself may be speculated.
The relevance of the results reported in this observational study is supported by the prospective design, the lack of specific selection of patients to be enrolled in the study, the very low rate of dropout, and the rather high level of physical activity performed by the patients. Although the presented data come from a cumulated assessment of only 90 patient-months, details on close to 1,000 IS devices have been provided by experienced patients. We cannot exclude, however, that the patients paid more attention to the use of the new IS. This potential bias could contribute to the better results obtained during the second study period.
Conclusions
The reported observational study provides updated information on adverse events occurring with currently used catheters in diabetes patients treated by CSII. While no severe outcomes on glucose control could be identified, still 9% of catheters present initial infusion failures, and 8% need premature replacements. The new FlexLink IS is associated with a significant reduction of initial failures that is likely related to a minimized trauma at insertion. In spite of an apparent better tolerance at infusion site, premature replacements are not significantly reduced. Further studies with a randomized control design could be valuable to better document the benefits of the new IS.
Appendix
Members of the Accu-Chek FlexLink Study Group are: A. Brac de la Perriere (University Hospital, Federation of European Private Establishments, Lyon, France), S. Clavel (Hôtel Dieu, Le Creusot, France), G. Di Pietro (Princesse Grace Hospital Center, Monaco), B. Guerci (University Hospital, Nancy, France), M.J. Haardt (Paris, France), P. Jan (Hospital Center, Bar le Duc, France), A.M. Leguerrier (University Hospital, Rennes, France), R. Leroy (Lille, France), C. Lucas-Croisier (University Hospital, Reims, France), A. Penfornis (University Hospital, Besançon, France), M. Pinget (University Hospital, Strasbourg, France), E. Renard (University Hospital, Montpellier, France), A. Solla-Gazagnes (Western University Hospital Group, Hôtel Dieu, Paris), and E. Verlet (Hospital Center, Dunkerque, France).
Footnotes
Acknowledgments
Funding support was provided by Roche Diabetes Care (Meylan, France).
Author Disclosure Statement
Honoraria were paid to the investigating teams for their participation in the study. R.B. is a part-time employee of Roche Diagnostics SAS.