
Abstract
Background:
Studies investigating the effect of real-time continuous glucose monitoring (CGM) combined with pump therapy on glycemic outcomes in type 1 diabetes are increasing. Pump therapy is well established as a “gold standard” for insulin delivery, offering improvements over multiple daily insulin injections. However, there is still a proportion of subjects using continuous subcutaneous insulin infusion in whom goals for metabolic control are far from achieved or benefits of this type of insulin therapy are transient. The SWITCH (Sensing With Insulin pump Therapy to Control HbA1c [hemoglobin A1c]) study is a multicenter, randomized, controlled, crossover study to evaluate if adding CGM to experienced pump patients with suboptimal metabolic control will provide additional insight enabling clinical and therapeutic benefit.
Methods:
Subjects meeting the inclusion criteria were randomized to Sensor On or Sensor Off arms for 6 months, after a 1-month run-in period. Following a 4-month washout period, the subjects crossed over to the other study arm for 6 months. The primary end point was the between arm difference in HbA1c levels. Among others, additional end points include time spent in different glycemic ranges, percentage of patients with HbA1c <7%, number of hypoglycemic events, glucose variability parameters, safety outcomes, treatment satisfaction, and quality of life.
Results:
Recruitment occurred between January 2008 and February 2009. A total of 153 patients were randomized. Study completion is anticipated in July 2010.
Conclusions:
The results will establish if adding CGM to existing, capable, insulin pump users can enable better metabolic control.
Introduction
Crossover studies of longer duration are not a conventionally applied methodology in diabetes. Benefits of this design include smaller sample size and greater efficiency than in parallel studies, as between-patient variation is removed as a subject acts as his or her own control. Challenges to this methodology include longer study duration and the risks to protocol compliance, dropouts, missing data, or the undesirable effects of carryover. Ludvigsson and Hanas, 7 DeVries et al., 8 and the 5-Nations Trial 9 provided examples of crossover designs, but these studies compared pump therapy to multiple daily injection therapy. Only in the study by Ludvigsson and Hanas 7 was retrospective CGM incorporated in order to facilitate treatment and patient motivation. The authors emphasized that the study was conducted at the introduction of CGM into clinical practice, where device inexperience created challenges for patient education. 7 Similarly, STAR-1, a sensor-augmented pump versus conventional pump study, also attributed failure to show significant metabolic differences to the newness of the device, use of new device features by both treatment groups, and frequency of study visits. 10
The aim of the SWITCH (Sensing With Insulin pump Therapy to Control HbA1c) study is to determine whether patients with T1D with suboptimal glycemic control already using CSII can improve metabolic profile using sensor-augmented pump therapy (SAPT). In this present article the SWITCH study design and methods are described, in particular, the crossover design and a selection process, which includes a run-in period incorporating educational assessment, to augment subject compliance to the protocol. Hence, the methodological design described here intends to control for confounders and elucidate the value of RT-CGM.
Study Design and Methods
The study was conducted in four adult and four pediatric sites in Europe experienced in personal CGM and insulin pump therapy. The total study duration for the patient was 17 months, including a run-in period, two 6-month treatment periods, and a 4-month washout period (Fig. 1). Randomization was done electronically via case report form according to a predefined randomization sequence on a 1:1 ratio within age groups in each center. All HbA1c measurements were sent to a centralized laboratory for analysis (Laboratorium für Klinische Forschung GmbH, Kiel, Germany). A total of 153 subjects were randomized to the study (Fig. 2). The study protocol received institutional Ethics Committee approval at each of the study centers. A written consent was obtained from all participants, with additional parent consent for participants <18 years old.
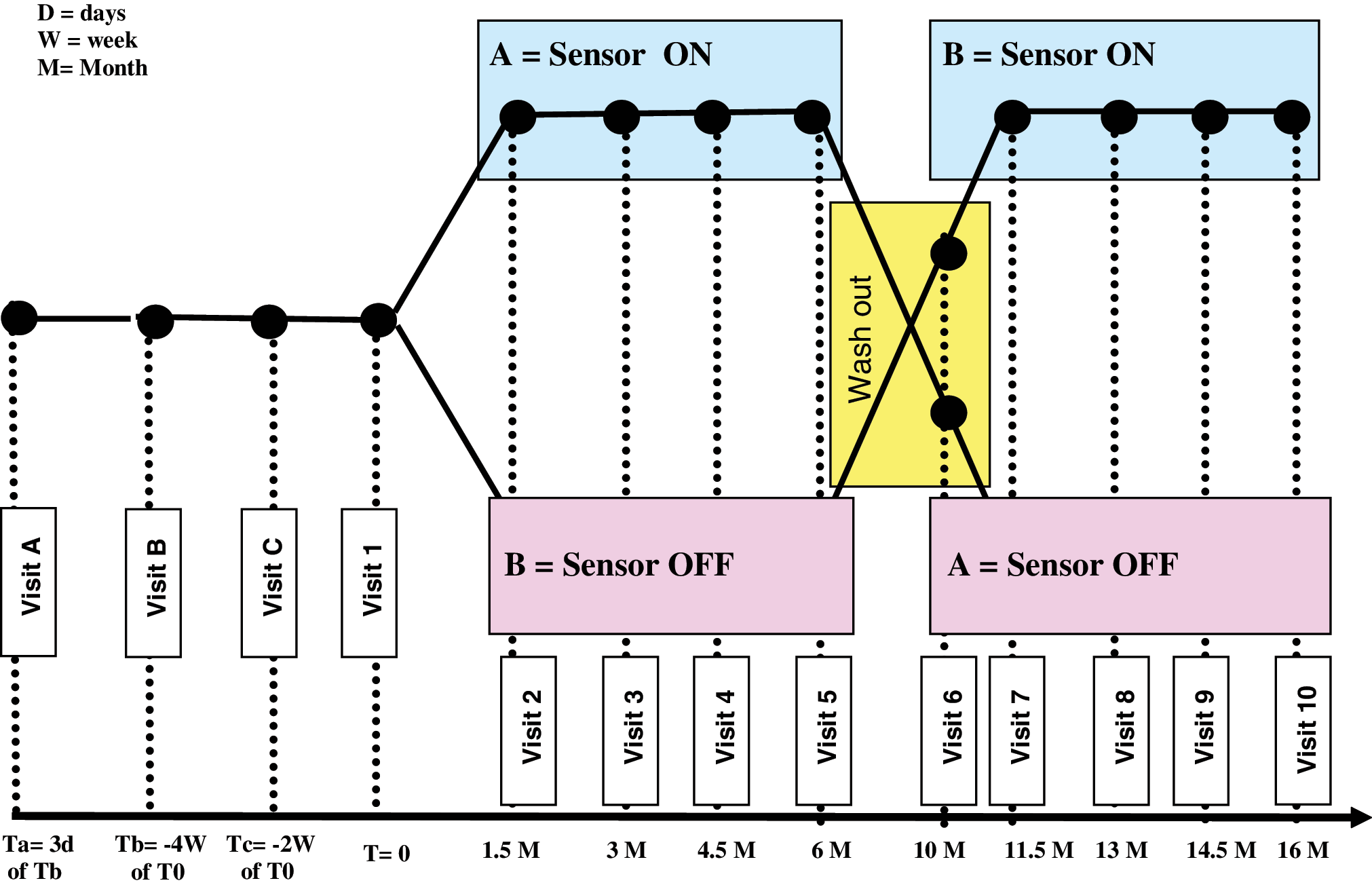
The SWITCH (Sensing With Insulin pump Therapy to Control HbA1c [hemoglobin A1c]) study design and visit plan. Color images available online at
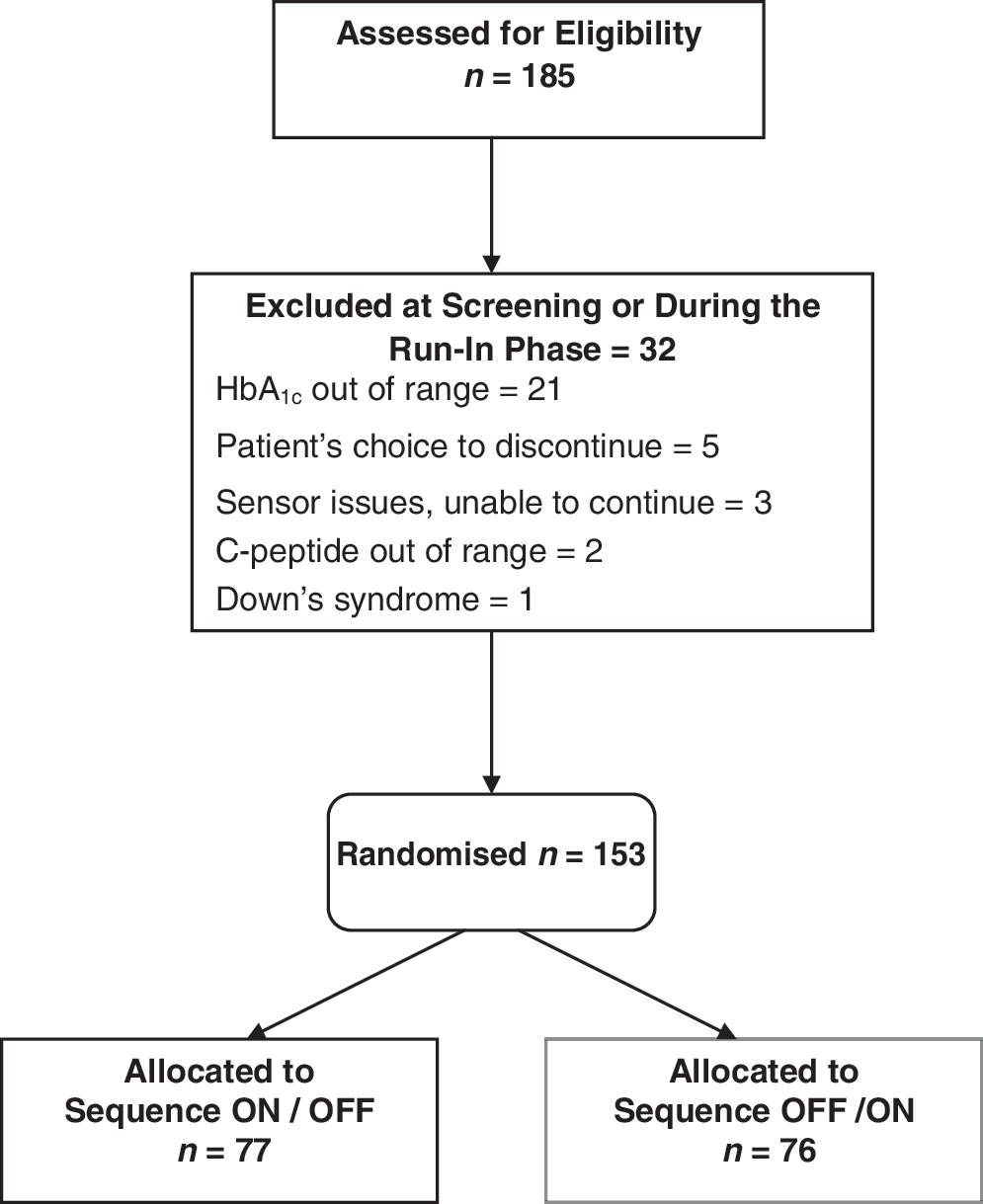
The SWITCH (Sensing With Insulin pump Therapy to Control HbA1c [hemoglobin A1c]) CONSORT flow chart to randomization.
Screening
Subjects between 6 years and 70 years of age with T1D for >1 year and CSII >6 months with suboptimal control (7.5% ≤HbA1c ≤9.5%) who were naive to RT-CGM were invited to take a five-question multiple choice test concerning pump therapy and general diabetes understanding. If the exam was passed with 100% outcome, they were invited to join the study (Visit A). Other inclusion and exclusion criteria are listed in Table 1.
BMI, body mass index; CSII, continuous subcutaneous insulin infusion; DCCT, Diabetes Control and Complications Trial; HBA1c, hemoglobin A1c; PRT, Paradigm REAL-Time; PIC, patient informed consent; SMBG, self-monitoring blood glucose; SWITCH, Sensing With Insulin pump Therapy to Control HbA1c.
Run-in phase
Following inclusion, patients were switched to the Bayer Ascensia® Contour glucose meter (without radiofrequency communication capability) [Bayer Suisse (AG) Diabetes Care, Zurich, Switzerland] and the Medtronic MiniMed Paradigm® REAL-Time System (Medtronic Inc., Northridge, CA) and received retraining on the principles of diabetes therapy and practical aspects of the pump system (Visit B). The system was worn for 2 weeks, after which blinded CGM data were collected over the next 2 weeks using the Guardian® REAL-Time System Clinical (Medtronic Inc.) (Visit C). Centers provided training on sensor insertion and device use. Evaluation of the subject's understanding of this training and incorporation of training given at Visit B were assessed by getting nine correct answers in a 10-question test. Failure to pass this test resulted in a screening failure. (See Supplementary Appendix [Supplementary Data are available online at
Treatment periods
Subjects were randomized at Visit 1 to either Sensor ON or Sensor OFF arms for 6 months. The Sensor ON arm received additional training and passed the Paradigm REAL-Time Comprehension exam (90% result on a 12-question test). Failure to pass this test resulted in re-education in the challenging areas. Subjects were advised to wear the sensor 85% of the time in the first 3 weeks to go through the “learning curve” and any potential challenges with the technology at this early stage. Subsequently, the subjects were advised to wear the sensor “continuously” or at minimum 80% for the duration of the treatment period. The Sensor OFF arm received this training and testing at Visit 6, after crossover following the washout period. Investigators were given a technical training checklist, and patients were provided optional diaries. For all subjects, study visits occurred every 6 weeks, when devices were uploaded by the medical team using the Medtronic CareLink® Therapy Management System and results were reviewed for treatment optimization. Visit frequency was determined by the memory capacity of the device, for example, if all features of the pump were used at maximum for the Sensor ON arm it would ensure no loss of data from memory overload. The RT-CGM and pump profiles for the Sensor ON arm were reviewed to make therapy adjustments, whereas SMBG data and pump profiles were used in the Sensor OFF arm. Patients were requested to perform more than four SMBG tests per day. Additionally, blinded CGM was collected from the Guardian REAL-Time Clinical device for 2 weeks prior to each visit in Sensor OFF arm. No treatment protocols or fixed algorithms were provided to the centers, and therapy adjustments were made in partnership with subjects at clinic visits. It remained the medical responsibility of the treating physician to guide the subject in reaction to RT-CGM values and hyper- and hypoglycemic alerts. Subjects were encouraged to make self-adjustments to their treatment, and examples of therapy changes were provided in the optional patient diary. Treatment satisfaction questionnaires 11 (Diabetes Treatment Satisfaction Questionnaires, subjects >18 years) and quality of life questionnaires 12 (PedsQL subjects ≤18 years old) are given to the subject at the start and end of each treatment period (Visit B, Visit 5, Visit 6, and Visit 10).
Washout
During this 4-month period, subjects continued with the provided study devices and wore the blinded device to collect CGM data 2 weeks before the end of the washout period. No RT-CGM was used by the subjects during this period. No other protocol was given to the subject in order to affect similar conditions between Visit 1 and Visit 6. As we found no published data on carryover in RT-CGM, the SWITCH study controlled for a possible carryover effect with a 4-month washout period, which we defined from unpublished data from previous studies and the half-life of the HbA1c measurement. Device uploads following the washout period (Visit 6) were reviewed for evidence of RT-CGM use, and if necessary the washout period could be extended to ensure compliance.
Sample size estimation and statistical analysis
Sample size of 124 subjects (62 randomized to sequence ON/OFF and 62 randomized to sequence OFF/ON) was calculated assuming a two-tailed matched-pairs t test and a type I error of 5%. With this sample size the study is powered at 90% to detect a mean difference of 0.3% in HbA1c. An SD of 1.0% has been assumed. In order to account for the duration of the study and possible dropouts or nonevaluable subjects, the sample size is increase by approximately 20%, giving a sample size of 160.
The primary end point is the difference in HbA1c level between the Sensor ON and the Sensor OFF after 6 months of follow-up. Mean, SD, and 95% confidence intervals for the 6-month HbA1c level will be reported.
The two groups will be compared using an analysis of variance adjusting for period effect and declaring subject as random effect. Period will be included in the model regardless of statistical significance. A 95% confidence interval and a P value will be given for the difference of the study arms based on the analysis of variance model. It is known that preliminary testing for carryover has harmful effects and should be avoided; 13,14 therefore this has been already addressed in the design phase of the study by using a 4-month washout period. Data will be analyzed using Per Protocol as well as Intent to Treat principles. The Intent to Treat population consists of all randomized patients irrespective of their compliance to the planned course of treatment or deviations from the protocol. In case of missing data in the Intent to Treat analysis, measurements from the same study period will be carried forward to substitute for missing end-of-period values, if they originate from at least 3 months from start of the period (Visit 3 in the first period and Visit 8 in the second period). If no measurements can be carried forward, as a conservative approach the end-of-period data that are available only for one period will be used to impute missing data in the other period. The Per Protocol population for the primary analysis of HbA1c level is defined as the set of successfully randomized subjects (regardless of number of SMBG) with minimum sensor use (Sensor ON arm), with no violation of entry criteria and who are compliant with the protocol. HbA1c data will be included in the analysis also in case the associated blinded sensor data for patients in the Sensor OFF arm are missing.
Secondary end points will be compared using an analysis of variance model similar to the one defined for the analysis of the primary end point. Sensor data for the secondary end points will be extracted from CareLink Clinical during the 15-day period prior the end-of-period visit day (Visit 5 and Visit 10 in Fig. 1). Included subjects will have at least 7 days of data. Summary statistics such as mean, SD, median, range, and percentiles will be given for additional end points. The statistical analysis plan for the SWITCH study was externally reviewed by the Jaeb Center for Health Research, Tampa, FL.
Discussion
The SWITCH study will be the first randomized crossover trial evaluating the inherent impact of sensor therapy in children and adults with T1D with suboptimal glycemic control despite using CSII. The study subjects are established patients using CSII, yet despite good knowledge of the condition and pump therapy and that they attend a highly experienced CSII-specialized center, good metabolic control has still not manifested. The SWITCH study population comprised adults and children with almost equal representation and dictates the same level of sensor usage compliance. SWITCH intends to elucidate whether the possible glycemic benefits seen in participants with suboptimal metabolic control despite previous intensive management with pump therapy are related to the introduction of RT-CGM, rather than reflecting the improvement associated to a better use of CSII technology. Knowledge gained from other studies has been applied by including assessments of the patient's level of knowledge regarding the disease and the therapy via mandatory tests and, by implementing a training checklist, to ensure appropriate therapy coverage by the participating centers teaching RT-CGM.
The last subject visit in SWITCH study is expected in July 2010 and will be followed by comprehensive data analyses.
Appendix
Steering Committee
Tadej Battelino, M.D., Ph.D., University Medical Center, Ljubljana, Slovenia; Ignacio Conget, M.D., Ph.D., University Clinical Hospital, Barcelona, Spain; Jan Bolinder, M.D., Ph.D., Karolinska Institute, Stockholm, Sweden; David Stocker, M.D. and Hannah Gough, M.S.C., Medtronic International Trading Sarl, Tolochenaz, Switzerland.
SWITCH Study Group
Tadej Battelino, M.D., Ph.D. and Nataša Bratina, M.D., University Medical Center, Ljubljana, Slovenia; Ignacio Conget, M.D., Ph.D. and Marga Giménez, M.D., University Clinical Hospital, Barcelona, Spain; Birthe Olsen, M.D. and Jannet Svennson, M.D., Glostrup University Hospital, Glostrup, Denmark; Rudolf Prager, M.D., Ph.D. and Ingrid Schutz-Fuhrmann, M.D., Hietzing Hospital, Vienna, Austria; Eva Hommel, M.D. and Lise Tarnow, M.D., Steno Diabetes Center, Gentofte, Denmark; Roel Hoogma, M.D. and Mrs. Femke Tillemans, Groene Hart Hospital, Gouda, The Netherlands; Ulrike Schierloh, M.D. and Carine DeBeaufort, M.D., Luxemburg Medical Center, Luxemburg, Luxembourg; and Nicoletta Sulli, M.D. and Blegina Shashaj, M.D., “Sapienza University,” Rome, Italy.
Footnotes
Acknowledgments
The authors would like to thank Dr. Kitty Formentin and Dr. Bart Gerritse for their valuable input to the protocol design. The analysis plan for SWITCH was subject to an independent critical review conducted by Craig Kollman, M.D., Director, Biostatistics, Jaeb Center for Health Research. The SWITCH study is sponsored by Medtronic International Trading Sarl, Tolochenaz, Switzerland. Bayer Suisse (AG) Diabetes Care supplied all the blood glucose meters used in the study.
Author Disclosure Statement
I.C. reports receiving lectures and consulting fees from Medtronic Inc., Bayer AG, GSK, Eli Lilly & Co., NovoNordisk A/S, Sanofi-Aventis, Novartis, and MSD. T.B. reports receiving consulting fees from Medtronic Inc. and Bayer AG, speaking fees from Bayer AG, Eli Lilly & Co., Medtronic Inc., and Novo Nordisk A/S, and research grants from Abbott Diabetes Care. M.G. reports receiving lectures fees from Medtronic Inc, GSK, NovoNordisk A/S, Sanofi-Aventis, Novartis, and MSD. H.G. and J.C. are fulltime employees of Medtronic Inc. J.B. reports receiving lectures fees from Medtronic Inc., Abbot Diabetes Care, Sanofi-Aventis, and MSD and consulting fees from Abbot Diabetes Care, Sanofi-Aventis, MSD, and Astra-Zeneca.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.