
Abstract
Background:
A device developed based on ink-jet printer technology can precisely control the size and volume of droplets ejected. Here, we evaluated the application of this technology to the pulmonary administration of insulin mist as a therapeutic measure for diabetes.
Methods:
Insulin ejected from the ink-jet device was initially characterized by high-performance liquid chromatography (HPLC) and mass spectrometry. Its effects on
Results:
Neither the HPLC nor the mass spectrometry profile of insulin was altered by the ink-jet process. The
Conclusions:
The ink-jet process did not affect the quality or biological activity of insulin, suggesting the potential use of the ink-jet device for insulin inhalation therapy for diabetes.
Introduction
In contrast, drug delivery via the pulmonary route alleviates pain and reduces psychological stress and is suited for children and the elderly, who are incapable of self-injection. For these reasons, expectations have been high regarding the efficacy of therapies delivered via pulmonary administration, such that inhalable medicine and specific devices for its administration have been developed. 2,3 The delivery of aerosolized insulin via the lungs remains a valid possibility in spite of the discontinuation of Exubera® by Pfizer (New York, NY) and the withdrawal by Lilly (Indianapolis, IN) and Novo Nordisk Pharma Ltd. (Bagsvaerd, Denmark) from the inhaled insulin market. AFREZZA™, the product of MannKind (Valencia, CA), is in the final stages of the Food and Drug Administration approval process, and other alternatives to injected insulin are also being developed. Patients with diabetes are likely to prefer a device of a comfortable size for daily use and that can deliver more accurate control of the concentration and size of droplets of inhalable insulin.
To overcome these problems, we investigated the ink-jet process established during the development of printer technology by Canon (Tokyo, Japan). 4 In this technology, the ink stream is heated in a pulsatile fashion by a microheater; as the bubble of ink vapor rapidly grows it increases the pressure upstream of the nozzle, causing fine ink droplets to be ejected from the nozzle. By replacing the ink with liquid medicine, a small amount of medicine in the form of mist can be ejected. Furthermore, this technology has advantages in terms of the precise control of droplet size and amount of mist. With these advantages in mind, we have developed a pulmonary administration device for insulin therapy for diabetes, as a typical hormonal treatment. Here, we provide details of the application of the ink-jet device for this purpose. We found that additives such as surfactants were necessary during the aerosolization of insulin, and thus their effects on insulin activity should also be examined. The ink-jet process also involves heating, to generate bubbles, which may also affect insulin activity. Therefore, it is necessary to investigate whether an insulin solution with surfactants is effectively absorbed in the lungs and retains its biological activity to lower plasma glucose level following pulmonary administration. At present, we are using the device only for in vitro and animal experiments to confirm that the ink-jet process does not alter the biochemical or physical properties of insulin, including molecular weight and biological activity.
We evaluated the efficacy of insulin solutions, with and without additives or ink-jet processing, by high-performance liquid chromatography (HPLC), mass spectrometry, cellular glucose uptake assay, and measurement of plasma glucose levels, following the administration of these solutions via the subcutaneous or pulmonary route.
Materials and Methods
Preparation of solutions
Arginine (Kishida Chemical Co., Ltd., Osaka, Japan) and lauroylsarcosine (Sigma-Aldrich Co., St. Louis, MO) were added to an insulin preparation (0.609 mmol/L, Novo Nordisk Pharma Ltd.) to give final concentrations of 9.3 mg/mL and 1.9 mg/mL, respectively. The pH of the solution was adjusted to 7.4. m-Cresol (Wako Pure Chemical Industries, Ltd., Osaka) was added to give a final concentration of 2.3 mg/mL. Hereafter “additives” indicates this mixture of arginine, lauroylsarcosine, and m-cresol. The prepared liquid solutions were ejected using the ink-jet device, and droplets of the resulting insulin mist were recovered. 5 The insulin content after the ink-jet process was measured to be 0.565 mmol/L or 3.27 mg/mL. The average size of aerosol particle was 3.84 μm (mean).
Fluorescein isothiocyanate (FITC)-labeled insulin (FITC-insulin) was prepared to investigate pulmonary insulin distribution. 6 One part of a 20 mg/mL solution of insulin (Wako Pure Chemical Industries) was mixed with one part of a 13.4 mg/mL FITC isomer I (Sigma-Aldrich Co.) solution and incubated for 2 h. The resulting FITC-insulin was separated from unlabeled insulin on a gel filtration column (Sephadex G-25, Amersham Biosciences, Little Chalfont, UK). Protein concentration was measured using a BCA protein assay kit (Pierce, Rockford, IL). The FITC-insulin solution was formulated such that it had the same composition as the insulin formulation and then supplemented with additives as described above.
The types and preparation methods of insulin solutions used in the following experiments are summarized in Table 1.
The final concentrations of additives (arginine, lauroylsarcosine, and m-cresol) were 9.3 mg/mL, 1.9 mg/mL, and 2.3 mg/mL, respectively.
FITC, fluorescein isothiocyanate; PBS, phosphate-buffered saline.
HPLC and mass spectrometry
Insulin solutions were separated by HPLC using a column (Crestpak C18S, JASCO Co., Tokyo) at a flow rate of 1 mL/min and eluted with a gradient of eluent B (acetonitrile/trifluoroacetic acid, 100:0.1 vol/vol) in eluent A (water/trifluoroacetic acid, 100:0.1 vol/vol) (gradient from 10% to 95% eluent B from 0 to 60 min, linear). Detection potentials were monitored by ultraviolet detection at 280 nm. The amount of insulin analyzed was calculated from the area of the peak for m-cresol after appropriate calibration. Next, insulin solutions were analyzed by matrix-assisted laser desorption/ionization–time-of-flight mass spectrometry using the ProteinChip® system (Ciphergen Biosystems, Fremont, CA).
Measurement of decreases in blood glucose level after subcutaneous injection
This study was approved by the Animal Experiment Ethics Committee of Jikei University School of Medicine (approval number H18-61), and all experiments were conducted in compliance with the regulations, standards, and guidelines for animal experiments in the University.
Male Wistar rats (8–9 weeks old, Sankyo Labo Service Co., Tokyo) were fasted for 15 h but allowed unrestricted fluid intake and then anesthetized with ether and pentobarbital. 7 –9 A small tail incision was made for venous blood collection. The insulin solutions were diluted to 12.2 μmol/L with phosphate-buffered saline (PBS), and 48.8 μmol/kg (rat weight) insulin was subcutaneously injected. 10 Venous blood was sampled 0, 15, 30, 60, and 120 min after subcutaneous administration and centrifuged at 1,000 g for 10 min at 5°C to recover serum. Plasma glucose level was measured using the glucose oxidase method (SRL, Tokyo).
Cellular uptake of d -glucose
L6 cells were plated in six-well dishes and incubated in Dulbecco's modified Eagle's medium containing 10% calf serum at 37°C with 5% CO2 in air until confluent. Cells were washed three times with 1 mL of HEPES-buffered saline and incubated in 1 mL of HEPES-buffered saline for 3 min at 37°C. Each of the insulin solutions was added to a single well to give a final concentration of 100 nmol/L. After addition of 2-
Measurement of decreases in plasma glucose level following pulmonary administration using a microsprayer
Pulmonary deposition
The BCI-3eBK ink-jet printer ink (Canon Ltd.) or FITC-insulin solution was administered to the lungs of 8–9-week-old male Wistar rats, anesthetized with ether, using the Microsprayer™ model 1A-1C (Penn-Century Inc., Wyndmoor, PA). 11 The Microsprayer aerosolizer is made of stainless steel and is 0.64 mm in diameter and 50.8 mm in length. Rats were immediately sacrificed, and the lungs were recovered for the preparation of paraffin and frozen sections to examine the pulmonary distribution of the ink using hematoxylin and eosin staining and FITC fluorescence, respectively.
Plasma glucose-lowering action
Venous blood samples were collected from the tails of 8–9-week-old male Wistar rats that were fasted the day prior to the procedure and anesthetized with ether. 7 –9 Each of the insulin (insulin and control insulin; insulin with additives) solutions was diluted to 0.076 mmol/L with PBS, and 100 μL (0.03 mmol/kg rat weight) was administered to the lungs using the Microsprayer. 12 The particle size of insulin administered by the Microsprayer was 16–22 μm. The rats were anesthetized with pentobarbital, and tail venous blood was sampled 0, 15, 30, 60, and 120 min following the pulmonary insulin administration. Blood samples were centrifuged at 1,000 g for 10 min at 5°C to recover the supernatant, and serum glucose level was determined using the glucose oxidase method.
Measurement of decreases in plasma glucose level following pulmonary administration of insulin solution using the ink-jet device
A ventilator was used to assist in insulin inhalation. 5 Pentobarbital (2.5 mL; 5 mg/mL) was administered to male Wistar rats (8–9 weeks old, weighing 250 g) fasted from the day prior to the procedure. 7,8 An Angiocath™ 14-gauge needle (Becton Dickinson Co., Franklin Lakes, NJ) was inserted into the exposed trachea and fixed with a thread to connect the ink-jet device and a rodent ventilator model 683 (Harvard Apparatus, Holliston, MA) to the bronchi. The ink-jet device was 15 cm in width, 15 cm in length, and 10 cm in height. In the dosing experiment of our rat study, we administered the mist that had been ejected from the ink-jet device and set its density of insulin in the circulating air (36.54 μmol/min) via the assisted inhalation system. The size of the aerosol particle (mean, 3.84 μm; range, 3.1–3.9 μm) was measured in a wet condition, specifically with 25°C and 40% relative humidity. As we planned to administer 0.06 and 0.09 mmol of insulin/kg (corresponding to 0.015 and 0.023 mmol of insulin, respectively, to a 250-g rat, respectively), the duration time of the administration for 0.06 and 0.09 mmol of insulin turned to be 4.2 min and 6.3 min, respectively. The other critical setting was 1.60–1.70 mL for the tidal volume, and for the ventilation frequency it was 60 cycles/min. The timing when the administration was just finished was set as 0 min for the post-administration observation period.
Venous blood was collected as described earlier, and blood glucose level was measured using a simple blood glucose test meter (Glucocard II Data GT-1650, Arkray Inc., Kyoto, Japan). 9,13 To determine plasma insulin level, the blood samples were centrifuged at 1,000 g for 30 min at 5°C following addition of aprotinin (6,200 KIU/mL) and heparin (1,000 U/mL) (both from Wako Pure Chemical Industries Ltd.). The supernatant was analyzed using an insulin enzyme-linked immunosorbent assay kit (YK060, Yanaihara Institute Inc., Shizuoka, Japan) to quantify insulin level.
Statistical analysis
The measured plasma glucose levels (n = 5) were analyzed using two-way repeated-measures analysis of variance and Tukey's test.
Results
This study evaluated the effects of an aerosolization process using an ink-jet device (ink-jet process), as well as additives such as surfactants, on insulin. Insulin solutions before and after being subjected to the ink-jet process and those before and after the addition of additives were compared.
HPLC and mass spectrometry
Possible changes in the mass of insulin caused by the ink-jet process were evaluated by HPLC (Fig. 1a) and mass spectrometry (Fig. 1b). The spectra of both the control insulin and the aerosolized insulin showed single peaks corresponding to an identical mass, when analyzed by either method.

High-performance liquid chromatography and mass spectrometry. The aerosolized insulin was analyzed by high-performance liquid chromatography and mass spectrometry before and after the ink-jet process. (
Decreases in plasma glucose level following subcutaneous injection of insulin
An impairment in the plasma glucose-lowering action of insulin that could possibly be caused by the ink-jet process was examined in rats. The effects of additives used for the preparation of aerosolized insulin were also studied. Figure 2 shows the changes in plasma glucose level after the injection of PBS, insulin, control insulin, and recovered aerosolized insulin. Plasma glucose level was significantly lower at 60 and 120 min post-injection in the group receiving insulin than in the group receiving PBS. Similarly, plasma glucose level was significantly lower at 60 min post-injection in the group receiving control insulin and at 60 and 120 min post-injection in the group receiving the recovered aerosolized insulin. There was no significant difference in plasma glucose level among the groups receiving different insulin preparations. These data show that neither the addition of additives necessary for insulin application to the ink-jet process nor the ink-jet process for preparing insulin mist impaired the blood glucose-lowering action of insulin.

Examination of reductions in plasma glucose level following subcutaneous administration of insulin to rats: phosphate-buffered saline (•), insulin (∘), control insulin (Δ), or recovered aerosolized insulin (□). Plasma glucose level was significantly lower 60 and 120 min after injection in the insulin-administered group than in the phosphate-buffered saline group. Similarly, plasma glucose level was significantly lower 60 min after injection in the group receiving control insulin and 60 and 120 min following administration in the group receiving recovered aerosolized insulin. There was no significant difference among the three types of insulin formulation. *P < 0.05 versus the phosphate-buffered saline group.
Cellular uptake of d -glucose
The effects of the ink-jet process during the preparation of insulin mist on insulin-mediated glucose uptake were examined. The control insulin and recovered aerosolized insulin were applied to L6 cells, and insulin-mediated cellular uptake of
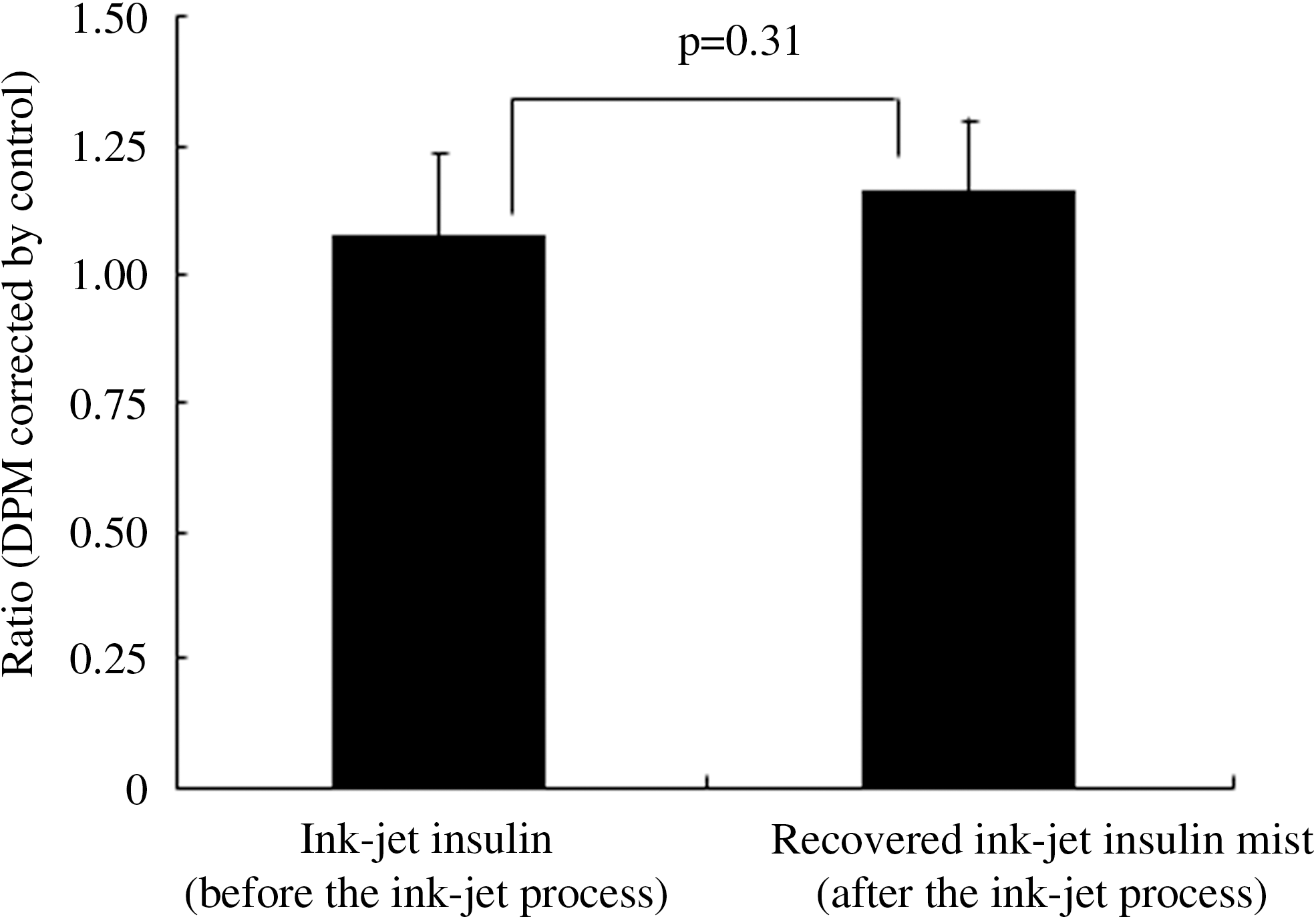
Cellular uptake of
Decreases in plasma glucose level following pulmonary insulin administration using a microsprayer
We examined the lung sites where insulin mist was distributed following pulmonary administration. First, ink was administered to the lungs using a microsprayer, and its distribution in lung tissue specimens observed. As shown in Figure 4, the ink was distributed unevenly in the lungs, with preferential deposition in the bronchi and inner alveoli.

Lung tissue from rats administered ink using a microsprayer. Black ink was administered into the trachea, and lung tissue was recovered for histological examination. The ink was unevenly distributed to the bronchi and alveoli. Original magnification ×40.
Next, FITC-insulin was similarly administered to the trachea, and its distribution in the lung section was examined by fluorescence microscopy. In good agreement with the distribution of the ink, FITC-insulin was unevenly distributed in the lungs and was found primarily in the bronchi and inner alveoli (Fig. 5).
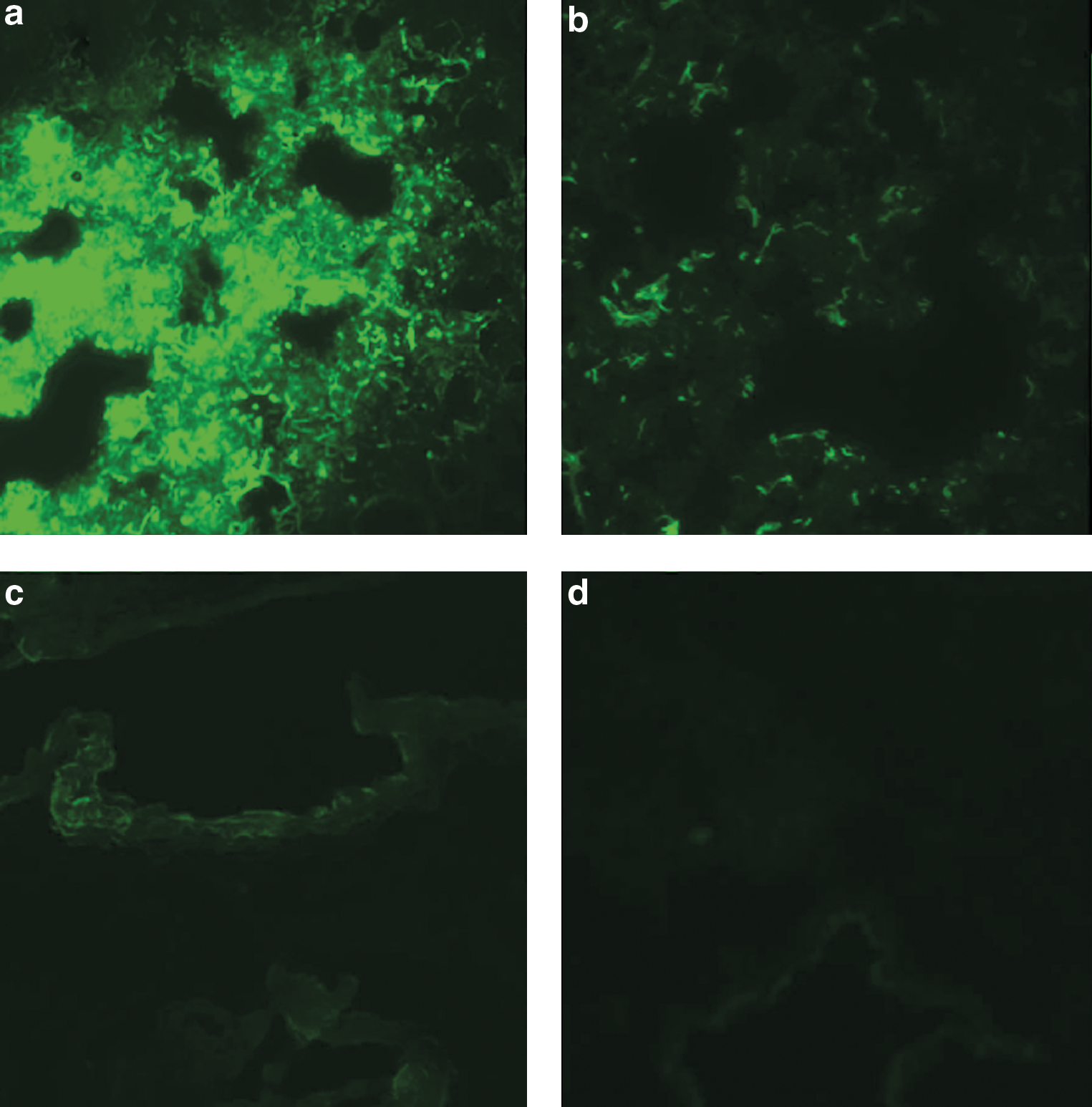
Fluorescence microscopy images of lung tissue from rats administered fluorescein isothiocyanate–insulin using a microsprayer. A total of (
Finally, the plasma glucose-lowering action of insulin administered to the lungs using a microsprayer was examined. Plasma glucose level was significantly lower at 15, 30, 60, and 120 min post-intratracheal administration in the group receiving insulin and at 30, 60, and 120 min following administration in the group receiving control insulin than in the PBS-administered control group (Fig. 6). Both insulin preparations, with or without the necessary additives for the ink-jet process, reduced the plasma glucose level to a similar extent following pulmonary administration.
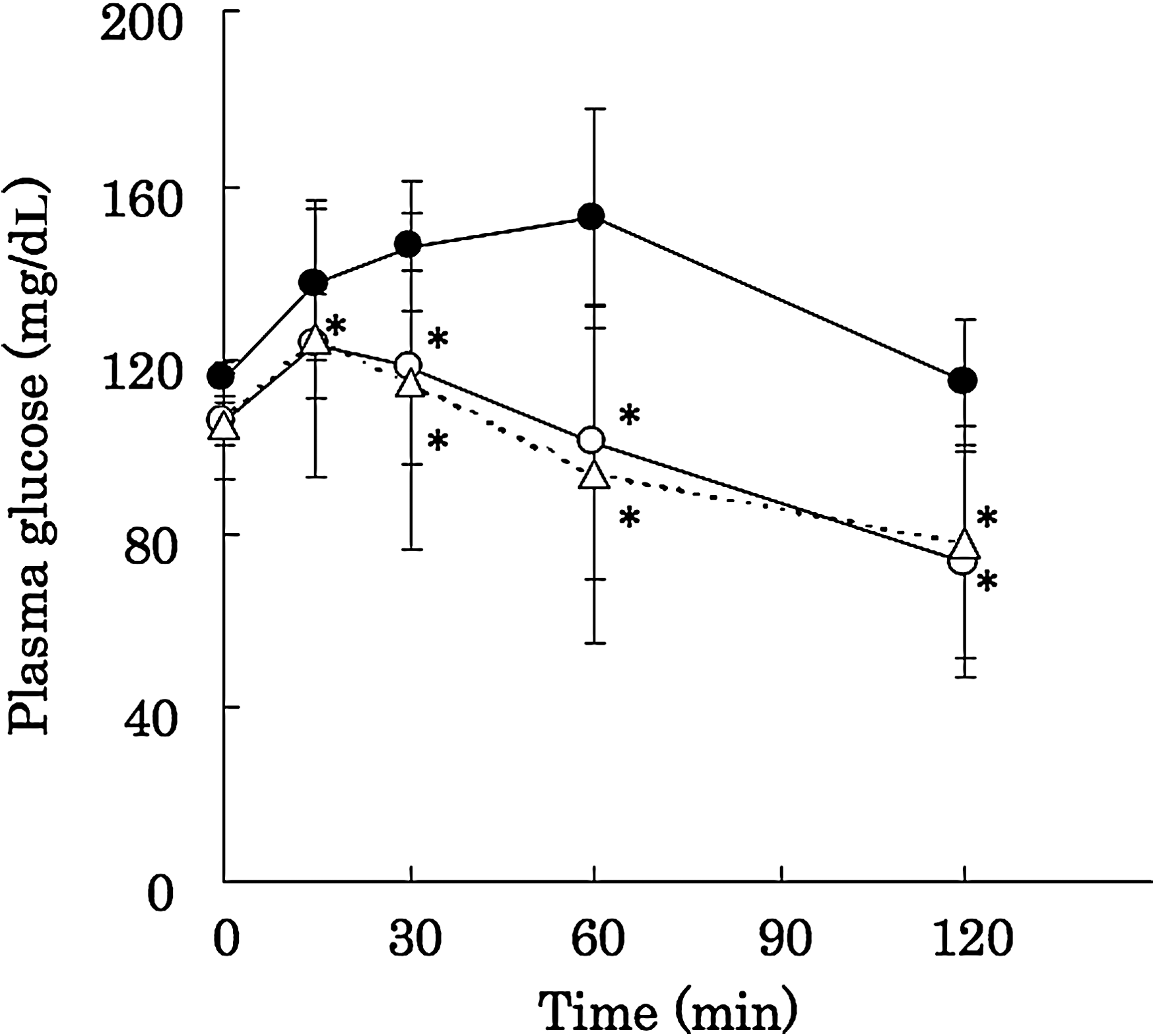
Changes in plasma glucose level after administration of insulin formulations using a microsprayer: phosphate-buffered saline (•), insulin (∘), or control insulin (Δ). The plasma glucose level was significantly lower 30, 60, and 120 min after administration in the group receiving insulin and the group receiving control insulin than in the phosphate-buffered saline-administered group. *P < 0.05 versus the phosphate-buffered saline group.
Plasma glucose-lowering action of aerosolized insulin following pulmonary administration
Insulin was aerosolized using the ink-jet device, and its plasma glucose-lowering action after ventilator-assisted pulmonary administration was evaluated in rats. The plasma glucose level tended to be lower in the group that inhaled the aerosolized insulin than in the control group (Fig. 7). Plasma insulin level was elevated 30 min after the inhalation of 0.06 mmol/kg aerosolized insulin (Fig. 8).

Changes in plasma glucose level after ventilator-aided pulmonary administration of ink-jet insulin mist. Rats were administered 0 mmol/kg (○), 0.06 mmol/kg (▪), or 0.09 mmol/kg (▴) of aerosolized insulin. Pulmonary administration of aerosolized insulin (both 0.06 mmol/kg and 0.09 mmol/kg), but not sham administration (0 mmol/kg), reduced the blood glucose level.
Comparison of plasma insulin level before and after inhalation of aerosolized insulin. The plasma insulin level was elevated 30 min after the inhalation of aerosolized insulin (0.06 mmol/kg) compared with the level before inhalation.
Discussion
Powder and liquid forms of inhalable insulin preparations have been developed and launched for therapeutic purposes. The powder form is stable at room temperature, not prone to microbial contamination, and applicable to large-volume administration. However, it has been reported to trigger coughing in 20–30% of patients. It should be noted that the coughing symptoms reported were transient, gradually disappeared with continuation of therapy, and seldom resulted in withdrawal from treatment; however, they remain a concern. The liquid form is rarely affected by air humidity and can be precisely administered in small doses. Diabetes treatment requires finely tuned administration of small amounts of insulin; therefore, liquid medication is preferable to powder medication. However, it is not possible to administer liquid insulin in a large volume. We hypothesized that a large volume of insulin is not necessary to reduce plasma glucose level if an appropriately controlled size of insulin droplet is used and the effective amount of insulin mist is accurately regulated. We have successfully addressed these requirements by using the ink-jet device. However, questions remain as to whether the bubble-generating process and additives involved in the ink-jet technology affect the biological activity of insulin. Here, we examined the efficacy of the aerosolized insulin.
Biological changes in the insulin mist prepared using the ink-jet device
Heating, drastic pH changes, vigorous mixing, high concentrations of salts and urea, reductants, and strong light cause conformational changes and reduction in the solubility and biological activity of proteins such as insulin. Our HPLC and mass spectrometry data detected no signs of insulin degradation after mist preparation. Arginine, which was used as an additive, inhibits protein denaturation and aggregation. 14 The plasma glucose-lowering action of the control insulin was retained after the ink-jet process, suggesting that arginine added to the control insulin prevented the denaturation and aggregation of insulin during mist preparation using the ink-jet device.
Furthermore, the mist preparation caused no difference in the biological activity of the control insulin in rats and L6 cells. The ventilator-assisted pulmonary administration of aerosolized insulin resulted in a reduction in plasma glucose level, indicating the efficacy of the ink-jet device. This suggests that the ink-jet device is a feasible means for delivering insulin in that the biophysical properties of insulin are not detectably altered by its use and the ejected insulin retains its biological function.
Pulmonary absorption of insulin mist administered using a microsprayer
Pulmonary administration of liquid and solid (powder) medications has been investigated using various animals. 15 The method of Schanker, 16 wherein the exact amount of liquid can be delivered to the lungs by a syringe, is well known as a liquid delivery method to the lungs in small animals. Another method is the delivery of medications in the mist form via air flow created by a ventilator. This method has the advantage of delivering medication deep inside the lungs, but has the disadvantage of not being able to specify precisely the actual amount administered to animals. A microsprayer can deliver a precise volume of liquid to the lungs, similarly to Schanker's method, 16 as well as spray medicine in a mist form like the ink-jet device. Exploiting these features, we used a microsprayer to determine the pulmonary distribution of an insulin solution. The solution was distributed unevenly, but deep inside the lungs, suggesting that the use of a microsprayer is suitable for investigating the actions of control insulin.
Drugs reaching the lungs are transported into blood via the alveolar paracellular or transcellular pathway to become effective. 17 Several agents that aid absorption of macromolecules such as insulin have been investigated in order to achieve effective transport of these molecules to the bloodstream. 18 Surfactants, liposomes, and protease inhibitors are examples of these agents. In this study, lauroylsarcosine, a surfactant, was added to the control insulin. No significant differences in plasma glucose-lowering actions were found between the insulin preparation with additives and insulin without additives at any time point after the microsprayer-aided pulmonary administration. Further studies are anticipated to evaluate more compounds that may improve the preparation of insulin mist using the ink-jet device.
Inhalable insulin
The mean size of the aerosol particle was 3.8 μm. The span, the parameter for polydispersity, was 1.09. The bubble-jet droplets have a volume mean diameter of 3.8 μm, similar to that produced by the AERx® iDMS system (volume mean diameter = 3.5 μm [Aradigm Corp. (Hayward, CA) and Novo Nordisk Phama Ltd.]). 19,20 Moreover, the span of the bubble-jet droplets is significant smaller than that of the NE-U22 nebulizer (volume mean diameter = 5.4 μm, span = 1.83) from Omron Corp. (Kyoto). The bubble-jet device also can easily vary the amount of droplets to be ejected because ejection is digitally controlled, which enable doses to be varied conveniently and extremely reliably. The optimal size for delivery to the alveoli is 1–3 μm in aerodynamic diameter. 21,22 The most effectively respired particles are commonly accepted to be in the range of 2–5 μm. The distribution of particle size is also of critical importance in terms of bioavailability and dosage reproducibility.
In general, the anticipated length of time for achieving adequate dosing of insulin to patients is around 2–3 s, but the key factors and functions of a dosing device should be determined in a patient-dependent manner or based on necessity. From the patient's point of view, the time should be 1 s, which is enough of an interval for a patient's single breath. Patients can repeat the dosing maneuver as needed. In this study, we did not explore conditions for humans because we have addressed specifically the stability in biological properties and the effectiveness of the insulin that was ejected from the bubble-jet device and was administered to animals via the pulmonary route. Therefore, the device was designed only for the animal experiment but was not constructed for clinical use at present.
Exubera is a powder form of insulin briefly marketed by Pfizer. During this short marketing period, various clinical effects were reported. It has been found that inhalable insulin freed patients from pain associated with injection and thus was accepted as a therapeutic modality. The effects of inhalable insulin were also previously investigated; insulin absorption was high in chronic smokers, and smoking enhanced insulin action. 23,24 Insulin action was impaired among patients over 65 years old or slightly impaired among bronchial asthma patients 22,25 and was enhanced or impaired among patients with chronic obstructive pulmonary disease. 26 Patients with chronic obstructive pulmonary disease demonstrated a variable absorption of insulin compared with subjects without this disorder. It is not clear whether this variability is secondary to differences in inhalation devices or to differences in study populations. However, the safety and impact of its long-term administration on the lungs remain unclear because it was only briefly available commercially. Further prolonged observation would be necessary to assess these parameters. Also, a microsphere- and liposome-based method for inhalable insulin has been developed 27 wherein insulin is packed in a phospholipid membrane made from an appropriate material such as lecithin. Encapsulated insulin in phospholipid particles may thus be absorbed without causing toxic effects on the surface of alveolar cells. As these methods were only tested in experimental animals, further studies are anticipated.
Conclusions
The efficacy of insulin solutions with additives prepared using an ink-jet device was evaluated by HPLC, mass spectrometry, cellular glucose uptake assay, and measurement of plasma glucose level, following the administration of these solutions via the subcutaneous or pulmonary route. Pulmonary administration resulted in a reduction in plasma glucose level in rats.
Footnotes
Acknowledgments
Experiments of this study was performed from 2003 to 2008. This study was supported in part by the Ministry of Education, Science, Sports and Culture with Grant-in-Aid 17590948 to T.S., 2005–2007.
Author Disclosure Statement
S.I., N.S., H.K., and M.S. are employees of Canon Inc., Japan. M.N., Y.S., K.S., N.N., M.O., and T.S. declare no competing financial interests exist.