
Abstract
Background:
Insulin pumps and real-time continuous glucose monitoring devices have recently been combined into the sensor-augmented pump (SAP) system. The objective of this study was the evaluation of the clinical use of SAP in a large series of children with type 1 diabetes using insulin pump therapy.
Methods:
A questionnaire was administered in all pediatric diabetologic centers in Italy; data were analyzed only regarding patients 18 years old or younger and using SAP for 6 months or more.
Results:
Among all patients using an insulin pump, 129 (13.5 ± 3.8 years old, with a disease duration of 6.3 ± 3.4 years) have been using SAP for 1.4 ± 0.7 years. Four hundred ninety-three patients (12.9 ± 3.4 years old, with a disease duration of 6.2 ± 3.3 years) using conventional insulin pump therapy for 1.7 ± 0.5 years have been evaluated as the control group. After 0.5–3 years of using SAP or conventional insulin pump therapy, glycosylated hemoglobin significantly improved (8.0 ± 1.5% vs. 7.4 ± 0.8% [P = 0.002] and 8.0 ± 1.6% vs. 7.7 ± 1.1% [P = 0.006], respectively); the improvement was higher with SAP (P = 0.005). Insulin requirement showed a significant decrease only in SAP patients (0.88 ± 0.25 vs. 0.7 ± 0.23 U/kg/day, P = 0.003). Body mass index did not change during the observation period. No diabetic ketoacidosis episodes were observed during the follow-up, and severe hypoglycemia significantly decreased in SAP patients (P = 0.04).
Conclusions:
The increased availability of continuous glucose sensors is likely to have a significant impact on pediatric diabetes therapy and education in the near future. In daily settings, patients using SAP can achieve a better control than patients using conventional insulin pump.
Introduction
More recently, the availability of continuous glucose sensors has allowed the patient to monitor real-time glucose values, review trend graphs for the latest hours, and receive alarms/alerts for impending hypo- or hyperglycemia. 4 Clinical studies on continuous glucose monitoring (CGM) have shown improvements in glycemic control in pediatric patients, 5,6 especially due to decreased postprandial hyperglycemic excursions. This has also been demonstrated in the initial reports about an integrated continuous glucose sensor and insulin pump platform (sensor-augmented pump [SAP]), 7,8 using the MiniMed Paradigm Real-Time® system (Medtronic Inc., Northridge, CA).
On the other hand, the results of a randomized controlled trial have been recently published. 9 This study showed significant benefit in the CGM group over a 26-week period in patients over 25 years of age, but less benefit among those 8–14 years of age and no benefit in the 15–24-year age group, with approximately 50 patients in each control and CGM group by age.
The aim of the present study was the examination of the usefulness and safety of SAP in a large population of pediatric patients with type 1 diabetes mellitus, evaluated at baseline and after a 3-year follow-up.
Subjects and Methods
This is a multicenter observational before–after study. A questionnaire was administered in all pediatric diabetologic centers in Italy (n = 65).
Data were analyzed only regarding patients with type 1 diabetes 18 years of age or younger and using SAP for 6 months or more. Information was returned from 48 (73.8%) pediatric diabetologic units, belonging to the Study Group on Diabetes of the Italian Society of Paediatric Endocrinology and Diabetology. This Group represents the referral centers for the diagnosis and treatment of pediatric diabetes and are located throughout Italy, thus ensuring complete coverage of the country.
Each center filled out a questionnaire, and the following data were collected from medical records: date of birth, date of onset of diabetes, metabolic control evaluated as value of HbA1c (measured at each center using the DCA-2000 analyzer [Siemens/Bayer, Milan, Italy]), insulin requirement, the age at which the pump therapy began, the age at which the SAP therapy began, body mass index (BMI), and hypoglycemic and diabetic ketoacidosis (DKA) episodes. Severe hypoglycemia was defined as a blood glucose value of <70 mg/dL (3.9 mmol/L) with a loss of consciousness or the patient's need for assistance. Data collection was completed by December 2008.
The primary end point was the change in HbA1c between baseline and the end of observation period. Insulin requirement, BMI, episodes of severe hypoglycemia and DKA, and days of sensor use were evaluated too.
The study was approved by the L. Sacco Hospital Ethical Committee and conducted according to the Declaration of Helsinki.
Continuous variables are displayed as frequencies or percentages. To compare groups t test, χ 2 test, and Fisher's exact test were used. Paired t test was used to analyze changes of continuous variables over time. Statistical significance was determined for a P value of 0.05.
Results
From the 48 responding centers, 12,549 patients with type 1 diabetes were identified; 1,437 (11.4%) were identified as insulin pump users. After an evaluation of all data collected, 129 patients younger than 18 years (age 13.5 ± 3.8 years, range 6–18 years; duration of diabetes 6.3 ± 3.4 years, range 0.6–14.5 years) were identified as SAP users, representing 9% of the total population. The mean follow-up period was 1.4 ± 0.7 years (range 0.5–3 years). Four hundred ninety-three patients (12.9 ± 3.4 years old, with a disease duration of 6.2 ± 3.3 years) using conventional insulin pump therapy for 1.7 ± 0.5 years were evaluated as the control group.
Primary reasons for SAP initiation were suboptimal metabolic control (HbA1c >8%) in 45% of patients, recurrent hypoglycemia in 25%, involvement in competitive sports in 10%, wide glycemic variability in 10%, and patient and/or family request in 10%.
Median glucose sensor usage per month was 13.4 days/month, without any significant correlation with HbA1c. After 0.5–3 years, HbA1c significantly improved in SAP users and in controls (8 ± 1.5% vs. 7.4 ± 0.8% [P = 0.002] and 8.0% ± 1.6 vs. 7.7 ± 1.1% [P = 0.006], respectively). However, the metabolic improvement observed was significantly better in the SAP group (0.6% vs. 0.3% [P = 0.005]) (Fig. 1). Insulin requirement showed a significant decrease only in patients using SAP (0.88 ± 0.25 vs. 0.79 ± 0.23 U/kg/day [P = 0.003] and 0.86 ± 0.23 vs. 0.83 ± 0.26 U/kg/day [P = not significant]). BMI did not change during the observational period (21.2 ± 3.2 vs. 21.4 ± 3.4 kg/m2 [P = not significant] and 20.9 ± 3.1 vs. 21.2 ± 3.1 kg/m2 [P = not significant], respectively).
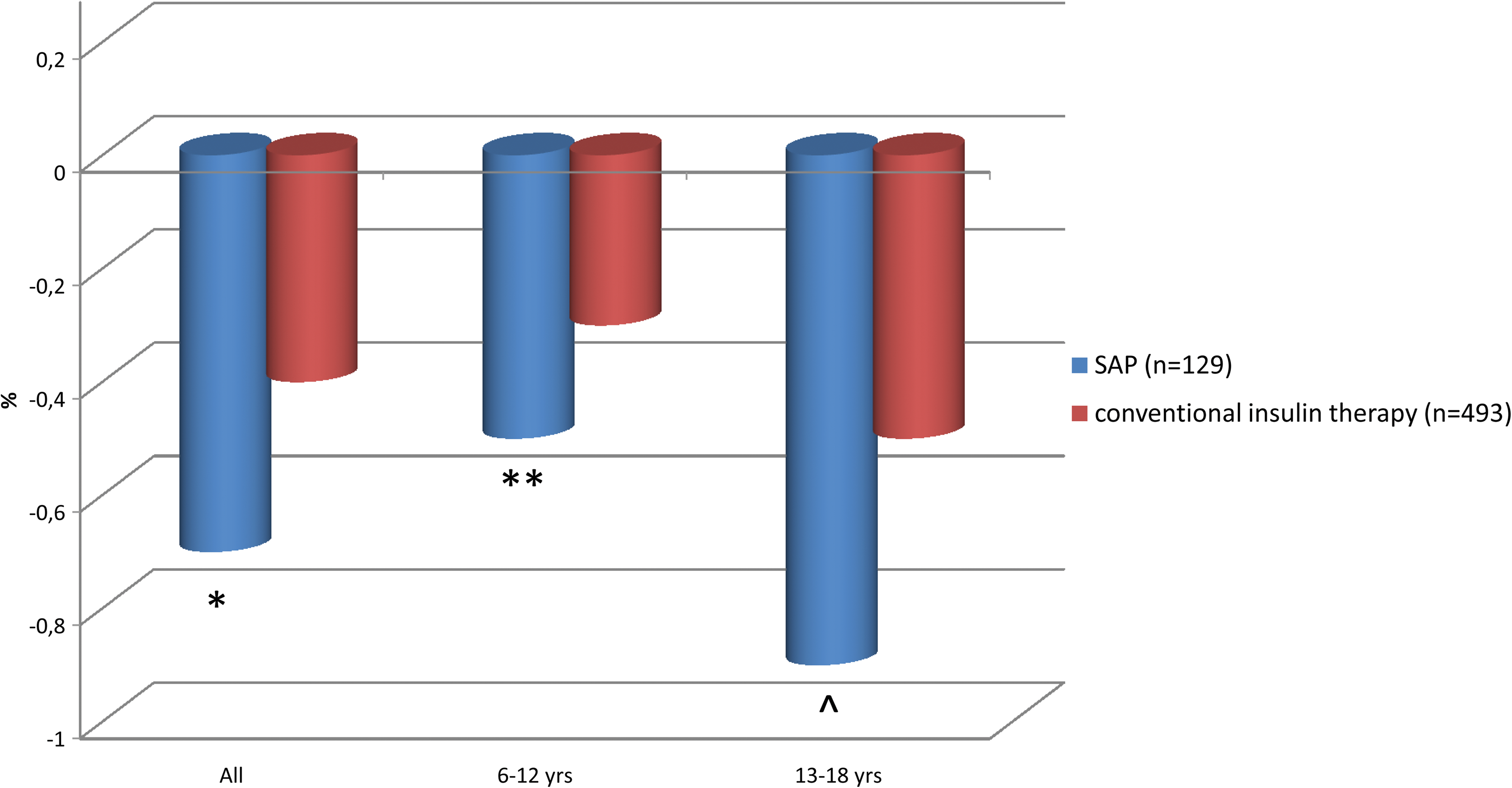
Improvement of glycosylated hemoglobin, expressed as change (baseline vs. end of observation) in patients using sensor-augmented pump (SAP) versus conventional insulin therapy. *P = 0.002, **P = 0.04, ^
P = 0.003 versus conventional insulin therapy. Color images available online at
No difference was observed in DKA episodes during the follow-up in both groups (0.5 vs. 0.3 events/100 patients/year [P = not significant] and 0.5 vs. 0.4 events/100 patients/year [P = not significant], respectively), whereas severe hypoglycemia significantly decreased only in patients using SAP (11.9 vs. 4.1 events/100 patients/year [P = 0.04] and 6.6 vs. 3.9 events/100 patients/year [P = not significant], respectively).
No difference was observed between patients using SAP who started using the insulin pump and CGM at the same time and those who started the insulin pump before using CGM.
To evaluate the effect of age on metabolic improvement we divided the patients into two groups: children (6–12 years) and adolescents (13–18 years). Even after this division, we confirmed an improvement in HbA1c (0.6% vs. 0.3% [P = 0.01] in children and 0.9% vs. 0.5% [P < 0.0001] in adolescents) (Fig. 1), with a decrease in insulin requirement in both groups (Table 1). No difference was observed regarding sensor use between children and adolescents.
Data are mean ± SD values.
P = 0.01, **P < 0.0001 versus patients using pump alone; † P = 0.005 versus patients using conventional insulin pump.
HbA1c, glycosylated hemoglobin; NS, not significant.
Stratifying results by sex, diabetes center, disease duration, or baseline HbA1c did not show any further difference.
Discussion
The SAP is a fully external system that allows a continuous insulin infusion along with a continuous recording of glucose values (reading every 5 min) by the use of a subcutaneous glucose sensor, which may be easily inserted under the skin for up to 3 days. The system transmitter is designed to send continuous glucose readings via radiofrequency to the pump, which is expected to display real-time glucose readings and to provide trend graphs as well as hypoglycemia and hyperglycemia alerts to patients, allowing them to monitor trends in their blood sugar levels and make immediate corrective adjustments using their insulin pump. 10
This retrospective review of data demonstrates a significant improvement in glycemic control for patients using SAP compared with patients using conventional insulin pump therapy. It also showed a reduced insulin dose for the SAP group and fewer episodes of hypoglycemia with no reported adverse effects.
The study was designed to address the specific question of whether using CGM and insulin pump therapy improved glycemic control, which it did. Moreover, to the best of our knowledge no other study seems to have examined these questions in as many patients for as long a period: our study sample comprises all patients who used SAP for 6 months or more between January 2006 and December 2008 at 74% of the pediatric diabetes centers in Italy and is nationally representative.
Because of the study design, we could not collect some potentially interesting data such as percentage of time spent in hypoglycemia or hyperglycemia or indexes of glycemic variability, and this is obviously a weakness of the study that we would like to address in a future prospective cohort study we are organizing to start.
Our findings agree with the few literature data available to date. In a pilot trial of 1 month, conducted on 10 children with type 1 diabetes using SAP, 8 the system allowed the patient to access real-time glucose readings, trend data, and hypoglycemic and hyperglycemic alerts, thus permitting patients/families to adjust insulin therapy, improving glycemia, and reducing episodes of hypoglycemia and hyperglycemia over time. Just after its release in 2006, we used SAP in a user evaluation that allow a significant decrease in HbA1c, insulin requirement, and hypoglycemic episodes. 11 Subsequently, some case reports or restricted experiences (small numbers of patients or short follow-up periods) have been published, 12 –15 and all agree on the usefulness of the new device in order to improve the metabolic control.
Even if our study is not a randomized controlled trial, it reflects what happens in the real life of the patients we take care of, and it is encouraging to see such a decrease (even if minimally clinically significant) in HbA1c even after more than 1 year from starting SAP. The improvement observed is slightly better than the mean one reported in recent meta-analysis on the topic 16,17 and even when compared with the conventional insulin pump therapy group, as we have seen in our study and in other studies. 18,19
Considering the patients according to age we found that the glycemic improvement is maintained in the adolescent group (13–18 years) as well: the HbA1c improvement is 0.9%, and, as stated from the Diabetes Control and Complications Trial, 1 this represents a really valuable outcome in terms of sparing microangiopathic and macroangiopathic complications.
In conclusion, the increasing availability of continuous glucose sensors is likely to have a significant impact on pediatric diabetes therapy and education in the near future. Selection of patients able and motivated to use SAP with proper age-appropriate education could be the key factors for the long-term success 20 of these new technological advances in diabetes therapy, as we have seen in our large group of children using SAP. The adolescent group achieved comparable, if not better, results than the younger age group. Education and motivation of the patient/family might be the key factors, and we have to make a great effort to improve our educational strategies.
Appendix
V. Cherubini and A.M. Cester, Ancona; S. Salardi and S. Zucchini, Bologna; G. Radetti and B. Pasquino, Bolzano; E. Prandi, Brescia; F. Gallo, Brindisi; P. Frongia, Brotzu Hospital, Cagliari; M.A. Zedda, Cagliari; A. La Loggia, Caltanissetta; D. Lo Presti, Catania; F. Citriniti, Catanzaro; M. Pocecco, Cesena; R. De Marco, Cosenza; F. Chiarelli and S. Tumini, Chieti; N. Lazzaro, Crotone; A. Vergerio, Feltre; S. Toni and L. Lenzi, Florence; M. Cotellessa, Imperia; S. Lucchesi, Livorno; C. Meossi, Lucca; D. Pardi, Massa Carrara; R. Taccardi, Matera; F. Lombardo, Messina; R. Bonfanti and F. Meschi, San Rafael Institute, Milano; G.V. Zuccotti, A. Scaramuzza, D. Spiri, and A. De Palma, University of Milano, Luigi Sacco Hospital, Milano; S. Boccato, Montebelluna; F. Prisco and D. Iafusco, Second University, Napoli; A. Franzese and P. Buono, Federico II University, Napoli; F. Cadario, Novara; G. Piredda, Olbia; C.M. Monciotti, Padova; F. Cardella, Palermo; M. Vanelli and G. Chiari, Parma; V. Calcaterra, Pavia; S. Cantoni, Reggio Emilia; A. Marsciani, Rimini; M. Cappa and R. Schiaffini, Bambin Gesù Hospital, Roma; M.L. Manca Bitti, Tor Vergata University, Roma; N. Sulli and B. Shashaj, Umberto I Hospital, Roma; M. Delvecchio, San Giovanni Rotondo; A.M. Marinaro, Sassari; F. Cerutti and I. Rabbone, Torino; F. Fontana, Tortona; V. Cauvin, Trento; L. Gargantini, Treviglio; A. Salvatoni, Varese; L. Pinelli and A. Sabbion, Verona; and C. Arnaldi, Viterbo.
Footnotes
Acknowledgments
We would like to thank all children and adolescents with type 1 diabetes and their families who with their great enthusiasm give us the possibility of studying new technologies.
Author Disclosure Statement
No competing financial interests exist for any of the authors listed on the first page or in the Appendix.