
Abstract
Objective:
This study evaluated the impact on quality of life (QoL) of an algorithm guiding the responses of continuous subcutaneous insulin infusion (CSII)-treated type 1 diabetes (T1D) patients using real-time (RT)-continuous glucose monitoring (CGM).
Research Design and Methods:
Sixty CSII-treated T1D participants (13–70 years old, glycosylated hemoglobin [HbA1c] ≤9.5%), including adult and adolescent subgroups, were randomized in age-, gender-, and HbA1c-matched pairs. Phase 1 was an open 16-week multicenter randomized controlled trial; Group A received CSII/RT-CGM with the algorithm, and Group B received CSII/RT-CGM without algorithm. Phase 2 was the 16–32-week follow-up study; Group A returned to usual care (CSII without RT-CGM), and Group B was provided with algorithm at 16 weeks. QoL was assessed by DQOL (adults) and DQOLY (adolescents) questionnaires at baseline, 16 weeks, and 32 weeks. Higher scores (range 1–5) indicate poorer QoL. Analysis was by analysis of variance (between group for baseline–16 weeks) and paired two-tailed t tests (within group for baseline and 32 weeks) with significance at P < 0.05.
Results:
Withdrawals left 28 of 30 patients in Group A and 27 of 30 patients in Group B at 32 weeks. In Phase 1, QoL in Group A (2.16 [0.44] baseline to 1.86 [0.40] at 16 weeks) improved compared with Group B (2.03 [0.47] to 2.03 [0.50]) (P = 0.002). Change in QoL correlated with changes in HbA1c (R = 0.36; P = 0.007). In Phase 2, Group A QoL was better at 32 weeks compared with baseline (2.16 [0.44] vs. 2.02 [0.43]) (P = 0.04) but was not in Group B (2.03 [0.47] vs. 1.99 [0.51]) (P = not significant).
Conclusions:
An algorithm guiding CSII-treated T1D responses to RT-CGM improved QoL, which persisted post-RT-CGM withdrawal. Algorithm provision at RT-CGM initiation was required to benefit QoL.
Introduction
We evaluated whether the provision of an algorithm to participants using CSII with RT-CGM in the ALG-OS study improved patient QoL.
Subjects and Methods
Details relating to the study subjects and methods have been previously published with the main study results. 2 A schematic of the study design is given in Figure 1. In brief, 60 T1D subjects (36 adults, 24 adolescents; 22 males, 38 females) established on CSII therapy were recruited in pairs matched for age (within 5 years), gender, and HbA1c (within 1%). Subjects were educated to use the MiniMed Paradigm® 722 Real-Time system (Medtronic, Northridge, CA) and randomly assigned algorithm or non-algorithm use. The pump RT-CGM sensor function was not activated until randomization. The algorithm includes both reactive and proactive components. Details of the algorithm are available at www.diabetesccre.unimelb.edu.au.

Overview of the study design and the flow of participants through the study. CSII, continuous subcutaneous insulin infusion; DQOL, Diabetes Quality of Life measure; DQOLY, Diabetes Quality of Life for Youths; RT-CGM, real-time continuous glucose monitoring.
In Phase 1 (baseline to 16 weeks), Group A patients were assigned CSII/RT-CGM with the algorithm for 16 weeks. Group B patients were assigned CSII/RT-CGM for 16 weeks without the algorithm. In Phase 2 (16–32 weeks), at 16 weeks Group A was returned to usual care with CSII alone, whereas Group B continued on CSII/RT-CGM, following 16 weeks of algorithm-naive use, and was provided with the algorithm. Both groups were followed to 32 weeks.
QoL was assessed at baseline, 16 weeks, and 32 weeks in adults using the Diabetes Quality of Life Measure (DQOL) 5 and in adolescents using the Diabetes Quality of Life for Youths (DQOLY) 6 scales. DQOL and DQOLY include sections on “Satisfaction,” “Impact,” and “Worry.” Both scales are scored on a scale of 1–5, with higher numbers indicating a poorer QoL. Prior to randomization a 6-day masked CGM device (Guardian® system, Medtronic) with no wearer access to RT glucose information was worn, and the data were uploaded remotely by users. One week prior to the end of Phase 1 and Phase 2, the masked CGM device was worn again for 6 days along with the unmasked Paradigm device in those on RT-CGM with both linked to a single transmitter.
Biochemical and CGM measurements, target glucose time, and mean amplitude glycemic excursion (MAGE) 7 were performed as previously described. 2 Data analysis was by analysis of variance (between group comparisons for baseline–16 weeks) and paired two-tailed t tests (within group comparisons for baseline and 32 weeks) with statistical significance taken at P < 0.05. Results reported are mean (SD) values.
Results
The analysis only includes those 55 subjects who returned for the 32-week visit. Their clinical data are summarized in Table 1.
Data are mean (SD) values.
DQOL, Diabetes Quality of Life measure; DQOLY, Diabetes Quality of Life for Youths; HbA1c, glycosylated hemoglobin.
Phase 1 (baseline to 16 weeks)
QoL at 16 weeks in Group A improved vs. Group B (2.16 [0.44] to 1.86 [0.40] vs. 2.03 [0.47] to 2.03 [0.50]; P = 0.002). In adults this change in QoL (2.16 [0.44] to 1.80 [0.40] for Group A vs. 2.10 [0.46] to 2.02 [0.49] for Group B) remained significant (P = 0.02). In adolescents the difference between groups (2.19 [0.49] to 1.91 [0.40] for Group A vs. 1.89 [0.49] to 1.99 [0.46] for Group B), while statistically significant (P = 0.02), resulted from QoL improvement in Group A and decline in Group B (both P = 0.09) (Fig. 2). There was no impact of gender on outcome.
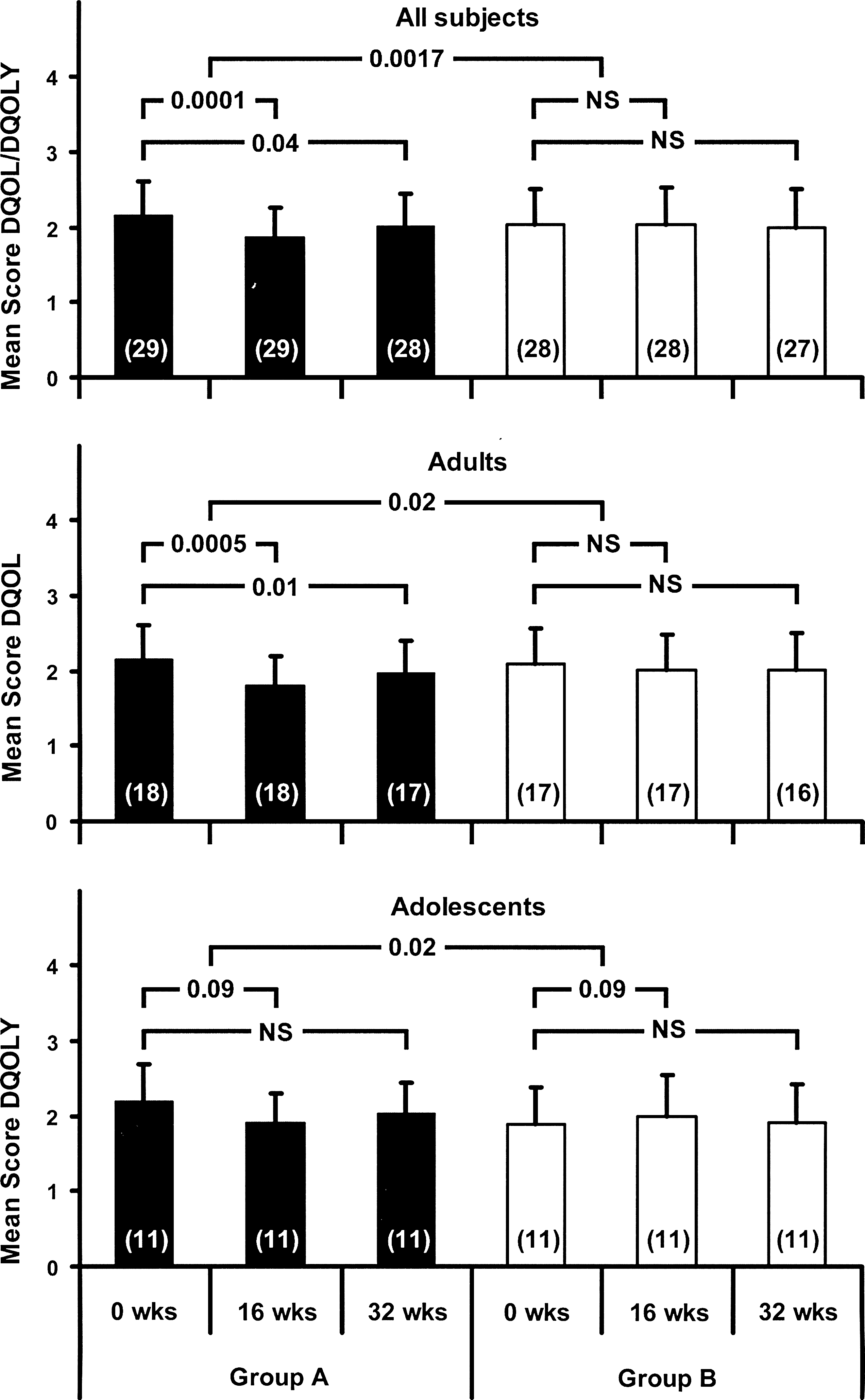
Mean scores for Diabetes Quality of Life measure (DQOL) and Diabetes Quality of Life for Youths (DQOLY) in Group A and Group B subjects at baseline, 16 weeks, and 32 weeks. Group A subjects were assigned continuous subcutaneous insulin infusion + real-time continuous glucose monitoring + algorithm at baseline for 16 weeks and were returned to continuous subcutaneous insulin infusion alone between 16 weeks and 32 weeks. Group B subjects were assigned continuous subcutaneous insulin infusion + real-time continuous glucose monitoring without the algorithm at baseline for 16 weeks; at 16 weeks they were provided the algorithm and continued on continuous subcutaneous insulin infusion + real-time continuous glucose monitoring to 32 weeks. NS, not significant.
Analysis of QoL subsections revealed that only the difference between groups in markers of “impact” were statistically significant: 2.23 (0.53) to 1.90 (0.54) for Group A vs. 2.06 (0.51) to 2.07 (0.53) for Group B (P = 0.005).
There were no statistically significant correlation between changes in CGM-determined time spent in target glucose range, the primary ALG-OS study outcome (r = 0.038; P = not significant) or MAGE (r = −0.19; P = not significant), with changes in QoL. The change in HbA1c and the change in QoL between baseline and 16 weeks correlated (r = 0.36; P = 0.007). A trend in correlation was observed with QoL scores attained at 16 weeks with sensor use (r = −0.34; P = 0.06).
Phase 2 (16 weeks to 32 weeks)
Group A QoL improved at 32 weeks vs. baseline: 2.16 (0.44) vs. 2.02 (0.43) (P = 0.04). QoL improved in adults (2.16 [0.44] vs. 1.97 [0.44]) (P = 0.01) but not in adolescents (2.19 [0.49] vs. 2.04 [0.40]) (P = not significant). Group B QoL did not change significantly (2.03 [0.47] vs. 1.99 [0.51]) (P = not significant), nor did scores for the adult (2.10 [0.49] vs. 2.02 [0.40]) (P = not significant) and adolescent (1.89 [0.49] vs. 1.90 [0.53]) (P = not significant) subgroups (Fig. 2).
Discussion
RT-CGM generates abundant glucose data that patients may find challenging. Previously published data from the ALG-OS study 2 indicated that the provision of a decision-support algorithm to RT-CGM/CSII-treated T1D patients increased the proportion of subjects achieving a target HbA1c of ≤7.0%. This benefit was only observed if the algorithm was provided at the time of initiation of RT-CGM, with no improvement in glycemia when algorithm provision occurred following 16 weeks of naive sensor use. Also, in those subjects provided the algorithm at RT-CGM initiation, following cessation of RT-CGM at 16 weeks and with resumption of conventional glucose monitoring based on finger-prick readings, glycemia returned to baseline. This suggested that both the timing of the provision of the algorithm and the continued use of the sensor were significant factors determining outcome. 2 This report details the QoL data from the same study. The results indicate that provision of the algorithm at the time of RT-CGM initiation improved QoL relative to a control group educated in CSII and RT-CGM device use but not provided the algorithm.
QoL analysis demonstrated that the provision of the algorithm reduced the impact of diabetes on routine functioning. However, there was no improvement in patient satisfaction regarding the time required to manage their diabetes, for social relationships, for work, and for leisure. Nor was there an improvement in worry related to work, leisure, relationships, and diabetes itself. Algorithm provision with RT-CGM/CSII reduces the limitations imposed by diabetes on the individual, but the intellectual, physical, and time demands required to achieve this may be responsible for a lack of improvement in the QoL satisfaction and worry scores.
Algorithm provision may provide a greater sense of order and “control.” Subjects who felt most empowered by the knowledge and technology may have been more likely to fully utilize these. Patient involvement in and contribution to management decisions also improve adherence and outcomes, 8 and a review of psychosocial outcomes indicated that QoL improved following education interventions focusing on diabetes self-management. 9 Provision of RT-CGM in the absence of guidance might increase information overload and emotional stress. 10 The observed trend towards decreased QoL in adolescents not provided the algorithm is consistent with these findings.
QoL changes over the first 16 weeks of the study correlated with changes in glycemia determined by HbA1c. QoL scores at 16 weeks also correlated with sensor use. The correlation between improvement in glycemia and the percentage time for which the sensor is worn is established. 2,11 –13 It is of interest that the improvement in QoL persisted at 32 weeks in Group A, following RT-CGM cessation and return of glycemia (HbA1c) to baseline. 2 It may be that the improvement in QoL following the provision of the algorithm in combination with RT-CGM in part reflects a perceived sense of empowerment that persisted despite the withdrawal of RT-CGM and subsequent increase in glucose levels. This suggests that the observed improvement in QoL, unlike HbA1c, is not entirely dependent on ongoing sensor use. Conversely, algorithm provision following 16 weeks of uninformed RT-CGM use had no effect on QoL or glycemia 2 at 32 weeks in Group B subjects. These subjects may have already established their own responses to and expectations of the technology. Our findings indicate that RT-CGM provision alone without guidance does not improve QoL. The provision and timing of patient education in how to respond to the glucose information may determine QoL outcomes.
Study limitations include the small sample size and socioeconomic homogeneity. Only CSII-established patients were studied. As there is no reimbursement for uninsured patients using insulin pumps in Australia, there was a likely bias toward privately insured higher socioeconomic groups. The algorithm evaluated in this study was directed at enhancing patient self-management. Tools measuring self-determination such as the Treatment Self-Regulation Questionnaire or the Diabetes Empowerment Scale may have provided a more focused assessment of the psychosocial impact of the intervention. Furthermore, the QoL tools used, DQOL and DQOLY, were validated approximately 20 years ago and may not be optimal for evaluation of the technologically based management that has developed in recent years. Newer, more sensitive tools appropriate to the technology are required. The literature suggests that a combination of DQOL and SF-36 may provide complementary data, with the former sensitive to lifestyle issues and the latter to functional health status. 14 To maximize adherence, a single questionnaire (DQOL/DQOLY) was selected that provided a broad assessment of QoL, and given the study's short duration it was expected that lifestyle would be impacted to a greater degree than functional health status.
The lack of association between changes in target glucose time and MAGE with QoL may relate to study size and limitations of the algorithm and of the tools used to assess glycemia. Also, wearing the masked CGM device at baseline may have altered subject behavior such that glycemia during the baseline 6-day period was not representative of that in the preceding 3 months. Finally, although the changes in QoL scores observed were statistically significant, the improvement was small (13.8%). The clinical relevance of these findings remains uncertain. It is possible that with more appropriate tools greater changes in QoL may have been observed.
In summary, early, but not late, provision of an algorithm guiding CSII-treated T1D responses to RT-CGM information improved QoL with persistent benefit at 3 months after RT-CGM withdrawal.
Footnotes
Acknowledgments
Ms. J. Horsburgh, Ms. M. Buszard, Ms. E. Fitzgerald, Ms. R. Humphreys, Ms. K. Palmer, Ms. Cheryl Steele, Ms. Kathy Steele, and Ms. M. Williamson made significant contributions to the formulation of the algorithm. This investigator-initiated study was supported by Medtronic Australasia Pty Ltd. and the NHMRC CCRE (Clinical Science in Diabetes). We acknowledge assistance from Ms. Joanna Sader, Ms. Leanne Foster, Ms. Connie Karschimkus, Ms. Katherine Davis, Dr. Alan Marcus, Dr. Christina Jang, Dr. Ayan Dasvarma, and Dr. Andrzej Januszewski. This work is dedicated to Mrs. Louise O'Neal.
Author Disclosure Statement
A.J.J., F.J.C., and D.N.O'N. have received research support, travel support, and honoraria from Medtronic Australasia, Eli-Lilly, Novo Nordisk, and Sanofi-Aventis. M.A.O'C. has received travel and education support from Medtronic Australasia and Novo Nordisk. P.S.H. has received research support, travel support, and honoraria from Sanofi-Aventis. P.G.C., B.K., J.D.B, C.R., and H.T. have no competing financial interests to declare.
This study is identified in the Australia and New Zealand Clinical Trial Registry with ID number ACTRN12607000198426.