
Abstract
Background:
Recently a considerable number of promising clinical trials have been designed to perform infusion of stem cells by pancreatic arterial intervention to improve the endocrine function of the pancreas for better diabetes control. It is necessary to investigate the pancreatic body and tail (PBT) arterial system for human islets located mostly in the PBT and identify the predominant artery or arteries. However, the arterial system in the PBT is complicated and variable. In this study we comprehensively investigated the anatomical characteristics of arteries feeding the PBT.
Research Design and Methods:
One hundred two patients with diabetes underwent 64-slice computed tomography angiography (CTA) and digital subtraction angiography (DSA). The target artery was catheterized, and DSA was performed to show the PBT. All images were documented for later analysis.
Results:
DSA demonstrated that the feeding arteries for the PBT included the dorsal pancreatic artery (DPA) alone (n = 51 [50%]), combined DPA and great pancreatic artery (GPA) (n = 22 [21.6%]), GPA alone (n = 16 [15.7%]), and transverse pancreatic artery (TPA) (n = 11 [10.8%]). DPA was observed to originate from the initial segment of the splenic artery (n = 34 [46.6%]), common hepatic artery (n = 17 [23.3%]), or superior mesenteric artery (n = 14 [19.2%]). The GPA was mostly from the middle (n = 36 [94.7%]), and only two were found to originate from the initial segment of the splenic artery. The TPA (n = 11) was from either the pancreatoduodenal artery (n = 5 [54.5%]) or the gastroduodenal artery (n = 4 [36.4%]). In most case, the predominant artery of the PBT (95.1%, 97 of 102) could be revealed by 64-slice CTA.
Conclusions:
The origins and identities of the predominant artery in the PBT are variable. DSA is superior to CTA for preoperative imaging in arterial intervention therapy.
Introduction
Previous studies have detected MSCs in multiple tissues after systemic injection in nude mice and other animal models. 6 –9 However, the highest levels of MSC engraftment were detected in the lungs, muscles, and bone marrow. MSCs were detectable only in bone marrow and spleen 2 weeks after infusion. Consequently, it was hypothesized that local administration of MSCs directly into pancreas would result in better islet regeneration. Therefore, intra-arterial pancreatic stem cell infusion was protocoled in most of the above-mentioned studies, based on the rationale that it may increase the local level of stem cells resulting in maximization of the effects.
The human pancreatic body and tail (PBT) contains most of the islets, 10,11 and the artery or arteries dominating the PBT were unquestionably the target artery for local infusion. However, anatomical studies of pancreatic arteries have mainly focused on the pancreatic head (for instance, chemotherapy for pancreatic head tumor), 12,13 and studies on the specific topic of the predominant arteries feeding the PBT seemed to be few. In the present study, we retrospectively analyzed the feeding arteries confirmed by digital subtraction angiography (DSA) and computed tomography angiography (CTA) during selective arteriography for cell infusion, and the characteristics of the PBT's predominant artery were evaluated, to lay a foundation for diabetes arterial interventional therapy, as well as to determine the detecting capability in the PBT's arterial network by CTA compared with DSA.
Research Design and Methods
Patient selection
One hundred two patients with diabetes (61 men and 41 women) were enrolled. Diabetes was defined with the World Health Organization 1999 diagnostic criteria. 14 Sixteen patients were with type 1 diabetes mellitus and 86 with type 2 diabetes mellitus. The average age was 43.1 years (range, 19–65 years). Patients with pancreatitis, hepatic cirrhosis, coagulopathy, aortic aneurysm, and chronic inflammation were excluded. The study protocol was approved by the ethic review board of our hospital. All eligible patients underwent standard informed consent procedures in accordance to the Declaration of Helsinki.
Imaging techniques
Arterial-phase images were obtained with 64-slice computed tomography (LightSpeed, GE Healthcare, Waukesha, WI). The scanning parameters were 120 kV, effective mA of 300 per section, collimation of 0.67 mm, a reconstruction interval of 0.9 mm with a 0.45 mm overlap, and a table speed of approximately 40 mm/s. The section revolution time was 0.75 s. For contrast enhancement, iodinated contrast material (Omnipaque™, GE Healthcare), at a concentration of 370 mg of I/mL, was administered at 1.8 mL/kg, with an infusion rate of body weight × 1.8/20 mL/s. Data acquisition for the arterial phase was initiated after a threshold level of 120 Hounsfield units was reached in the abdominal aorta. From the images obtained, three-dimensional images of the vascular architecture were reconstructed to show the PBT arterial network. The branching of the PBT predominant artery was then investigated.
DSA was performed using an angiographic system with a 30- × 30-cm flat-panel detector (Innova 3100, GE Healthcare) 2–3 days after CTA. First, selective DSA of the celiac artery, gastroduodenal artery, and superior mesenteric artery was performed by injecting 10 mL of iopamidol (Iopamiron® 370, Bayer Schering Pharma, Berlin, Germany) at a rate of 5 mL/s through a four-French catheter to locate the potential predominant feeding artery of the PBT. The target artery was then catheterized, and DSA was performed to show the PBT by injecting 4–5 mL of iopamidol at a rate of 0.5–2 mL/s. In some cases the predominant arteries originating from the splenic artery curled acutely, which were difficult to directly catheterize. A balloon catheter was used to obstruct the distal segment of the splenic artery, and the PBT was depicted by proximal splenic arterial angiography. All images were documented for later analysis.
Image analysis
Four independent radiologists experienced in pancreatic imaging viewed the DSA and CTA images. The target artery eligible by at least three of the following criteria was identified as predominant artery: (1) the first depicted artery located in the region of pancreas when showing the parent artery; (2) the minimal arterial size was 4 Frenches (1 French = 0.33 mm); (3) the artery traveled through most of the region of the pancreatic neck, body and tail; or (4) most of the fraction of the PBT, even including part of the pancreatic head, was perfused by contrast after target arterial angiography.
Results
Identities and quantities of the predominant arteries feeding the PBT are shown in Table 1, and sample images are shown in Figure 1. The dorsal pancreatic artery (DPA) was identified to be the predominant artery in most cases (50%), as expected. The PBT was generally dominated by one artery in most cases, but in 22 patients the DPA and the great pancreatic artery (GPA) had a similar size and perfusion scale on digital images, which were identified as predominant arteries jointly. In cases with the DPA absent, the GPA or transverse pancreatic artery (TPA) was found to be predominant as its replacement. In one rare case, the predominant artery was the anterior pancreatoduodenal superior artery originating from the gastroduodenal artery. In another rare case, the predominant artery included both the GPA and the caudal pancreatic artery originating from the middle segment of the splenic artery.
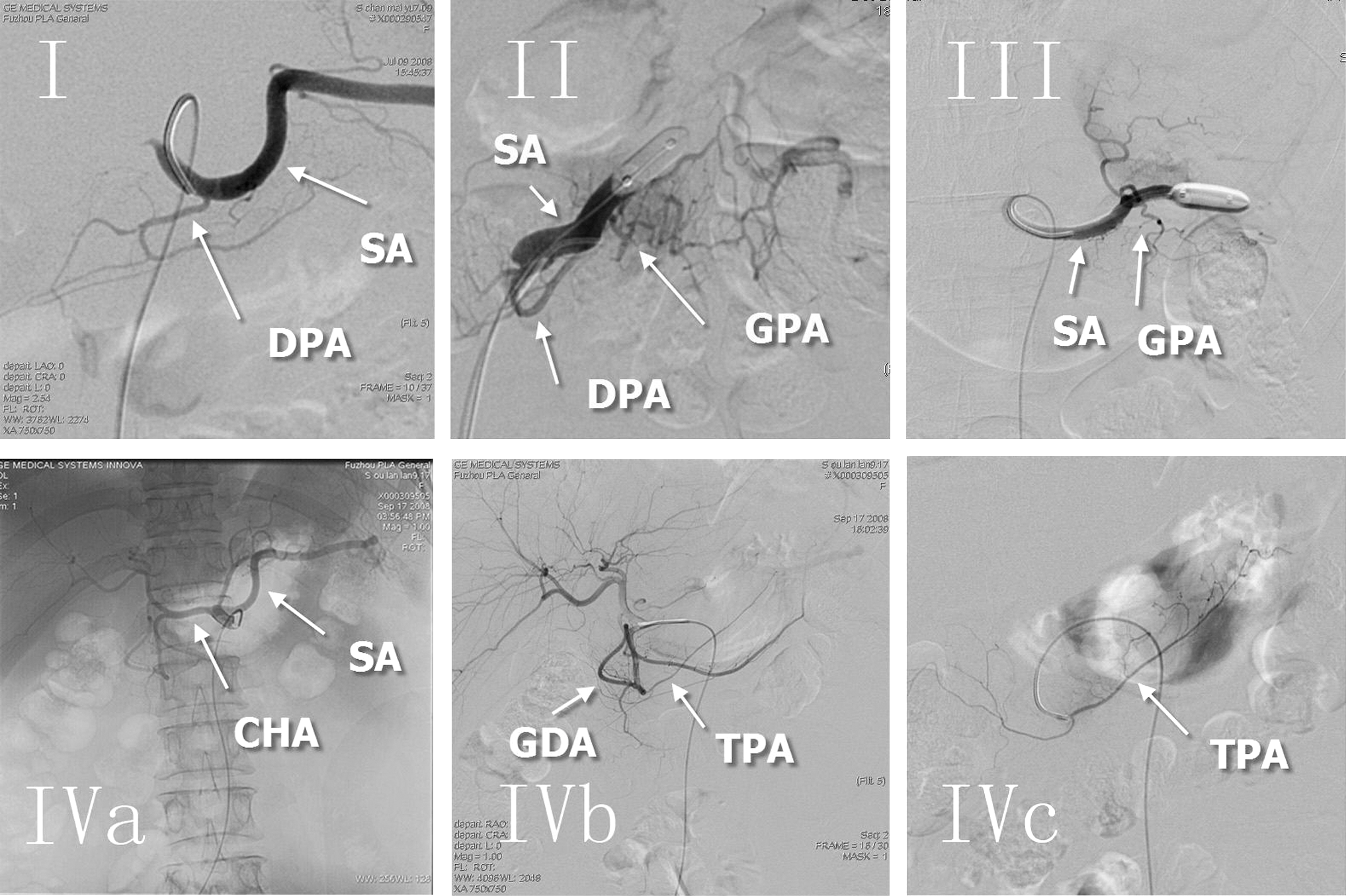
Different identities by digital subtraction angiography of the predominant arteries feeding the pancreatic body and tail: (
All cases of predominant arteries were successfully shown by digital subtraction angiography (DSA). In five cases, predominant arteries failed to be identified by computed tomography angiography (CTA): one was the dorsal pancreatic artery (DPA), one was the great pancreatic artery (GPA), and two were DPA and GPA jointly.
TPA, transverse pancreatic artery.
Origins of the predominant arteries feeding the PBT are shown in Table 2 and Figure 2. The TPA originated from the superior pancreatoduodenal artery in three cases and the inferior pancreatoduodenal artery in two (Table 2).
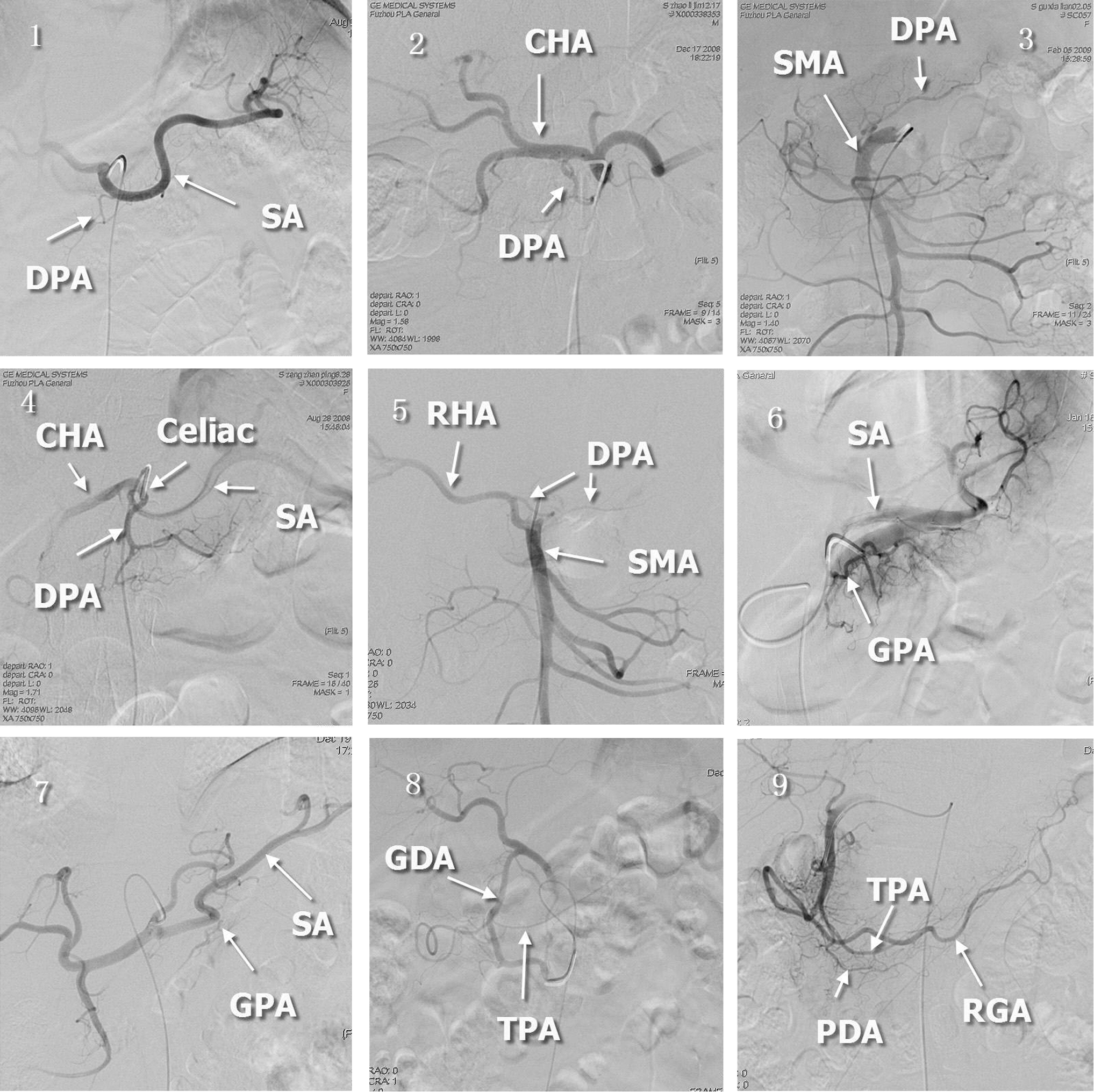
Different origins of the predominant arteries feeding the pancreatic body and tail: (
Seventy-three cases of dorsal pancreatic artery (DPA) as the predominant artery included 51 of DPA alone and 22 cases of DPA and great pancreatic artery (GPA) jointly.
Thirty-eight cases of GPA as the predominant artery also included 16 GPA alone and 22 cases of DPA and GPA jointly.
TPA, transverse pancreatic artery.
CTA satisfactorily showed the predominant artery in most cases (Fig. 3) but failed in five cases (Table 1). The target artery was directly catheterized in 74.5% of patients, while angiography was performed by temporary obstruction of the splenic artery in the remaining 25.5%, of which the feeding arteries were DPA and/or GPA.
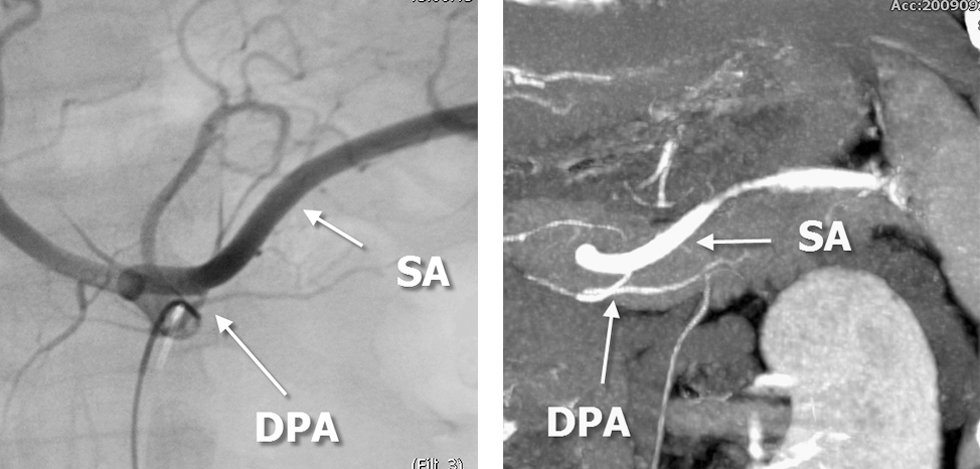
Sample images showed similar depicting performance by computed tomography angiography (
Discussion
The pancreatic head and the PBT are fed by different arterial networks. The head is fed by the anterior and posterior pancreatoduodenal arcs, whereas the PBT is fed by the DPA, GPA, TPA, and caudal pancreatic arteries. Feeding arteries for the pancreatic head have been widely studied because of local chemotherapy for head cancers. 15 Although variation of the DPA has been reported, 16 no reports on the arterial network of the PBT by DSA or CTA have been published. As arterial interventional methodology is being developed for diabetes treatment, the necessity is increased for studies in the arterial network of the PBT.
In the present study, the predominant artery was preliminarily determined by routine DSA of the celiac, gastroduodenal artery, and superior mesenteric artery. Comprehensive routine angiography could avoid omission of the target artery and selection of the minor artery. Although DPA is deemed to be the classic predominant artery, 16 it was found that either GPA or TPA could be predominant as its replacement. The ratio was unexpectedly high as shown in the Results. This finding is practical for future studies in PBT interventional therapy.
The DPA, GPA, and caudal artery generally originate from the initial segment, the middle segment of the splenic artery, and the segment close to the splenic hilum, respectively. TPA is connected to the three arteries, and these conjoined thereby constitute a network. However, it was found that each of the four arteries could originate from two to five positions. For instance, DPA originated from the initial segment of the splenic artery in half of the cases, as well as from the common hepatic, superior mesenteric, right hepatic, and celiac arteries in other cases. This is accordance with previous reports. 13,16
Although DSA is one of the preferred alternatives for preoperative evaluation of the predominant artery feeding the PBT, it is invasive and accompanied with probable serious risks such as vascular injury and pancreatitis. Therefore, an experienced operator and radiologist were required. CTA is convenient, noninvasive, and safe with few contraindications, and the thinnest slice during CTA reaches 0. 625 mm at present, all of which facilitate its wider application. 17 However, CTA is incapable of evaluating arterial perfusion and occasionally fails to show the target arteries.
In conclusion, the origins and identities of the predominant artery in the PBT are variable, and DSA has a better performance than that of CTA in showing the PBT arteries.
Footnotes
Acknowledgments
This study was supported by the Major Research Project Fund of Fujian Province (grant 2009Y4001) and the Technology Innovation Platform Project Fund of Fujian Province given to the Provincial Transplantation Biological Key Laboratory (grant 2008J1006).
Author Disclosure Statement
The authors have nothing to disclose.